
Abstract
Background. Vaccine-preventable diseases contribute significantly to under-five deaths, particularly in low- and middle-income countries. In Uganda, immunization coverage disparities persist among marginalized communities like the Batwa. This study explores perspectives on pediatric vaccination within the Indigenous Batwa in western Uganda. Methods. A qualitative phenomenological approach was used, with data from 15 mothers/caretakers, 8 health extension workers, and 3 community leaders in Kisoro district. Interviews were conducted privately, audio-recorded, and analyzed thematically. Results. Three themes emerged: (1) Misconceptions and concerns about vaccine safety and distrust in Western medicine; (2) Cultural beliefs favoring traditional healing; and (3) Access challenges, including geographical and socioeconomic barriers. Trust and comfort with healthcare providers, especially Batwa, were vital to reducing stigma. Conclusion. Addressing misconceptions, educating on vaccine safety, and building trust are key. Culturally sensitive programs and engaging Batwa care providers can improve vaccine uptake and acceptance by enhancing comfort and trust in vaccination efforts.
Keywords
Background
Worldwide, an estimated 700 000 children under 5 die annually from vaccine-preventable diseases, with nearly 99% of these fatalities occurring in low- and middle-income countries. 1 This toll is exacerbated by children’s susceptibility to severe symptoms due to immature immune systems and diverse environmental exposures. 2 According to World Health Organization (WHO), immunization prevents 2 to 3 million deaths annually. 3 However, despite this progress, inequalities persist, especially in sub-Saharan Africa, where a significant number of children continue to lack access to crucial vaccines. 4 Approximately 1 in 5 children in Global Alliance for Vaccines and Immunization (GAVI)-supported countries remain under-immunized for the third dose of the essential childhood vaccine containing diphtheria-tetanus-pertussis (DTP3). 5 Among these, 10.6 million children have not received their first dose of DTP, categorized as zero-dose children. 5 These disparities hinder the advancement toward global immunization objectives outlined in initiatives like the Global Vaccine Action Plan (GVAP) and the Sustainable Development Goals (SDGs), which seek to achieve universal vaccine access by 2030.
Infants and preschoolers are particularly vulnerable to illnesses and complications from infections that can be prevented through vaccination. 6 The World Health Organization (WHO) recommends a set of vaccines for all immunization programs globally to support effective immunization schedules. These include Bacillus Calmette–Guérin (BCG) for tuberculosis, hepatitis B vaccine, polio vaccine, diphtheria, tetanus, and pertussis-containing vaccine (DTPCV), Haemophilus influenzae type b (Hib) vaccine, pneumococcal conjugate vaccine, rotavirus vaccine, measles vaccine, rubella vaccine, and human papillomavirus vaccine (HPV). 7 The WHO-endorsed immunization plan indicates that a significant portion of mandatory childhood immunizations is administered before age 7, making this age range particularly relevant for studying parental attitudes toward vaccination. 8 Despite varying levels of socioeconomic development, vaccine hesitancy is a concern in many countries worldwide, with estimates suggesting its presence across WHO member countries. 9 A comprehensive retrospective study involving 149 countries, analyzing global trends in vaccine confidence, revealed that confidence in the importance of vaccines had the strongest single-factor correlation with vaccination coverage. 10 This underscores the need to explore caregivers’ perspectives on pediatric vaccination, especially for preschoolers. 11
Sub-Saharan Africa, particularly East Africa, including Uganda, continues to have the highest rates of infant and under-five mortality worldwide, 12 a situation that may be closely associated with low vaccination uptake. In Uganda, the national immunization coverage conceals inadequate sub-national coverage since there is a lack of specific information on local populations lacking full vaccination. 13 Despite efforts such as setting up vaccination outposts, conducting outreach programs, and initiating community health worker to improve routine immunization programs, marginalized and vulnerable communities like Batwa often remain underserved. 12 Disparities in the adoption of routine vaccines have led to a growing number of un/under-immunized children, closely associated with periodic outbreaks of vaccine-preventable diseases. 12
In 2019, Uganda’s vaccination coverage was relatively high, with Diphtheria, Tetanus, and Pertussis (DPT3) at 93%, Pneumococcal Conjugate Vaccine (PCV3) at 92%, Polio 3 at 92%, BCG at 88%, Rotavirus (RotaC) at 87%, and Measles-containing Vaccine first dose (MCV1) at 87%. 14 Despite this, inequities in access to vaccination persist, particularly affecting marginalized communities like the Batwa. 15 These inequities, combined with vaccine hesitancy, contribute to frequent outbreaks of vaccine-preventable diseases such as measles. 16 The Batwa, as a marginalized and Indigenous group, face unique barriers, including geographical obstacles, inadequate healthcare infrastructure, and socioeconomic constraints. 16 These accessibility issues can exacerbate vaccine hesitancy by complicating the process of obtaining vaccinations, thereby increasing mistrust in vaccine effectiveness and safety. Addressing these barriers is essential to improving the vaccination experience and reducing hesitancy. Understanding the Batwa’s perspectives and experiences is crucial for developing targeted interventions to enhance vaccination coverage and effectively address these challenges.
Methods
Study Design
A qualitative phenomenological study was designed to investigate the perspectives of pediatric vaccination among the Batwa community in Kisoro district, western Uganda. This study aimed to explore perspectives related to vaccination for children based on the experiences and responsibilities of participants within the Batwa community. A qualitative approach was chosen to delve into and understand the barriers to complete vaccination at the levels of family members, health workers, and vaccination service delivery. The research was conducted in December, 2023.
Study Settings
The study was conducted among the Batwa community, an Indigenous group in Kisoro district, western Uganda. This community resides in the districts of Kabale, Kisoro, and Kanungu. Kisoro District shares borders with Kanungu District to the north, Kabale District to the east, Rwanda to the south, and the Democratic Republic of the Congo to the west (Figure 1). The town of Kisoro is located about 45 km (28 miles) west of Kabale, which is the largest town in the sub-region, reachable by road. The district was selected due to its significant Batwa population and accessibility.

Map of Uganda showing Kisoro district.
Participants
The participants in this study comprised mothers/caretakers and community leaders from the Batwa community and health extension workers from health centers who served as key informants. The inclusion criteria encompassed health professionals working in Kisoro District and mothers/caretakers residing in Kisoro District for a minimum of 6 months before the data collection period. The exclusion criteria involved health workers who had worked in the district for less than 6 months, as they might have lacked experience with child vaccination, and mothers/caretakers who were unable to be interviewed due to illness or hearing problems.
Sample Size Estimation
The sample size for the qualitative study was determined based on achieving the ideal saturation of participants. Sampling and data collection continued until data saturation was achieved. The participants included 15 mothers/caretakers, 8 health extension workers, and 3 community leaders who were knowledgeable about pediatric vaccination within the Batwa community.
Sampling Procedure
In our study, purposive sampling with maximum variance was used to ensure a comprehensive representation of different perspectives within the Batwa community. We purposively selected participants based on specific traits and demographics (age, gender, occupation, religion, residence, occupation, education, caregiver status and vaccination status of children), to capture a wide range of experiences and viewpoints. Health extension workers were chosen for their direct experience with the Batwa community and their knowledge of child immunization. Mothers and caretakers were included if they had children who were not fully vaccinated, thereby providing insights into barriers and challenges related to vaccination. This approach allowed us to gather diverse and relevant information, addressing the varied experiences and perspectives within the community.
Data Collection Methods
The data collection for this study involved key informant interviews and in-depth interviews with health extension workers, community leaders, and mothers/caretakers, utilizing a prepared interview guide with probing questions. This guide, developed using narrative interviewing techniques, emphasized the importance of allowing participants to freely share their experiences. 17 It began with an open-ended question, such as “Please tell me about your experiences with pediatric vaccination among the Batwa community,” followed by specific prompts tailored to their experiences and perspectives. While the interview guide itself was not a validated questionnaire, however, an iterative pilot-testing process was followed. A small sample of participants, similar to the study group were identified an interviewed to assess whether the questions were understandable, culturally appropriate and were capable of eliciting meaningful responses. Feedback from these interviews was utilized to guide refinement of the guide including certain prompts that participants found unclear, while also adding additional probes to encourage deeper exploration of themes. Extended filed notes were also done during the interviews to complement the recorded audios. All the interviews were conducted at home at a convenient time and place suggested by the participants to ensure privacy.
Procedure
Face-to-face, semi-structured interviews were conducted by trained researchers familiar with the local culture and fluent in the local languages of the Batwa community. The interviews were one-on-one, conducted by researchers including 2 psychologists, 1 educationist and a public health specialist. One of the interviewers was female and 3 were males. All interviewers are lecturers at a public university possess over 5 years of experience in conducting qualitative research. In recognition of the community’s strong reliance on traditional healing methods, the interviewers employed culturally sensitive approaches, engaging local leaders and traditional healers in the preparatory phases to ensure that the study respected and incorporated community beliefs and practices. Interviews were carried out in private and quiet settings within the Batwa community to ensure confidentiality and comfort. All interviews were audio-recorded with the participants’ consent and conducted in either English or the participants’ native language, with translations into English performed as necessary. There were 3 males and 1 female interviewers. Prior to the interviews, the purpose, risks, and benefits of participation were explained to the participants. Written informed consent was obtained from all participants or their legally authorized representatives before the study began. For minors, assent was obtained from their parents or guardians. Each interview lasted approximately 40 to 50 minutes.
Data Analysis
In our study, we employed Braun and Clarke’s 18 thematic analysis approach to systematically analyze the qualitative data collected from the Batwa community. The analysis followed 6 detailed steps, beginning with data immersion and transcription to understand the content and context deeply. This foundational step allowed us to familiarize ourselves thoroughly with the data. We then generated initial codes to capture key concepts, acting as labels for the data’s significant aspects. Subsequently, we searched for overarching themes by identifying recurring patterns relevant to our research questions. This involved an iterative process of reviewing and refining potential themes to ensure accurate data representation. Themes were validated against coded extracts, and once confirmed, we defined and described each theme in detail, assigning clear, descriptive names to clarify their meaning and scope. The integration of these themes into a coherent narrative aimed to present a comprehensive understanding of the data. Our analysis was enriched by diverse perspectives from the principal investigator, and 3 experts in qualitative research, as well as collaborative workshops, fostering a holistic and inclusive approach to capturing the complexity of perspectives on pediatric vaccination within the Batwa community. Additionally, we ensured data saturation was achieved by continuing data collection and analysis until no new themes emerged, thus confirming the depth and breadth of our insights.
Rigor
To ensure the rigor of our study on pediatric vaccination perspectives within the Batwa community, we implemented robust measures aligned with Lincoln and Guba’s 19 criteria for qualitative research, focusing on credibility, dependability, confirmability, and transferability. For credibility, we held regular team meetings that fostered a collaborative environment, promoting consensus-building and inclusive decision-making. Our team’s diverse disciplinary backgrounds enriched the analysis, and we actively addressed potential researcher biases during both data collection and analysis.
To enhance dependability, we conducted in-depth individual interviews (IDIs) in a non-judgmental space, encouraging participants to express their perspectives freely. We used enhanced probing techniques and open-ended questions to avoid premature conclusions, allowing participants to guide the conversation organically. By framing interviews as reciprocal conversations, we built trust, minimized power dynamics, and encouraged genuine sharing.
Confirmability was achieved through methodological triangulation, engaging healthcare providers, service users, and village health teams to validate findings from multiple perspectives. Collaborative thematic analysis workshops with “Experts by Experience” further refined our interpretations and mitigated individual biases. These rigorous measures collectively strengthened the reliability and trustworthiness of our study, enhancing its potential transferability to similar contexts. Additionally, a few of the participants were approached to check through the transcripts and the final report to ensure that they represented their views during interviews.
Ethical Approval and Informed Consent
The authors for this study sought ethics approval from the Lira University Research Ethics Committee with approval number (LUREC-2023-87).
Results
Socio-Demographic Characteristics of the Participants
A total of 26 participants took part in the study with an ager range of 20 to 100 years. Most of the participants were female, with no formal education and with at least 2 children.
Themes
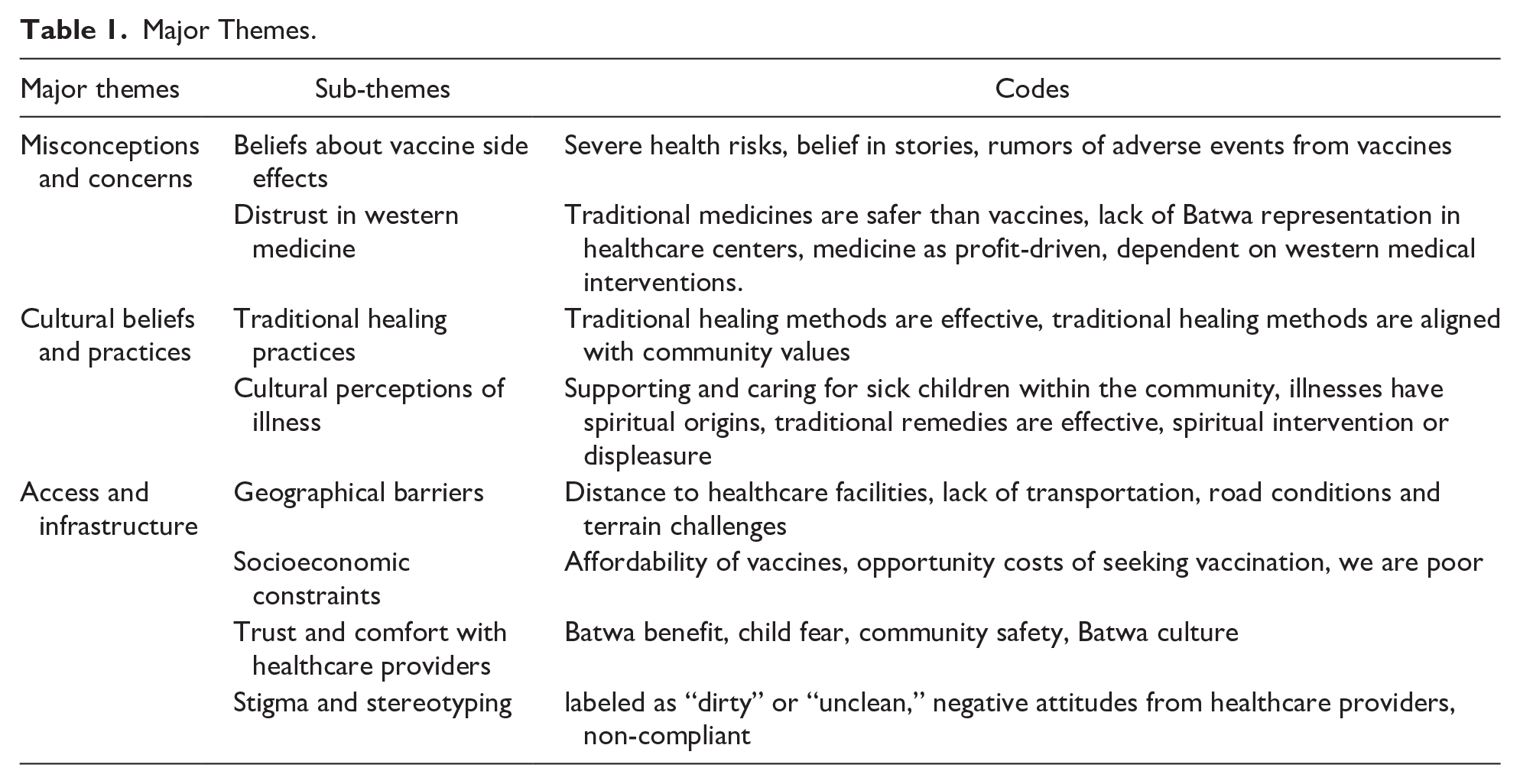
After thorough analysis, 3 overarching themes along with several sub-themes were discerned. The primary themes include: (1) misconceptions and concerns, encompassing sub-themes such as beliefs concerning vaccine side effects and a general distrust in western medicine; (2) the interplay of cultural beliefs and practices with perspectives on vaccination; and (3) the challenges of access and infrastructure, with sub-themes including geographical barriers and socioeconomic constraints like limited access to healthcare facilities, rugged terrain, and financial burdens. Moreover, the study revealed a notable emphasis on trust and comfort with healthcare providers, indicating a marked preference for providers from their own community due to the prevalence of stigma and stereotyping within mainstream healthcare settings (Table 1).
Major Themes.
Theme 1: Misconceptions and Concerns
In the Batwa community of western Uganda, a significant theme emerges concerning pediatric immunization: misconceptions and concerns. Beliefs about vaccine side effects, often fueled by stories and rumors, contribute to a reluctance toward immunization. This reluctance is further compounded by 2 sub-themes: concerns about adverse effects and distrust in Western medicine. Although the study’s sample size is limited, these findings offer valuable insights into the specific challenges and perceptions within the community, providing a foundation for future research and targeted interventions.
Subtheme 1: Beliefs About Vaccine Side Effects
The Batwa community holds beliefs about vaccine side effects, with prevalent fears of severe health risks. Stories and rumors within the community contribute to this anxiety, emphasizing concerns like swelling at the injection site, rashes, unusual crying, and vomiting after vaccination. These fears, ingrained and stemming from notions of vaccines being unnatural and harmful, lead to a preference for traditional healing methods and a general reluctance toward immunization.
“Many in our community fear the swelling that comes after a vaccination. They believe it will leave their child disabled, unable to use their arm. This misconception runs deep, passed down from elders who remember stories of children with swollen arms who never recovered.”
“The swelling after a vaccine is a curse to us. Our people have seen it happen, and they fear it more than the diseases. They say, ‘Better to have a sick child than a child with a useless arm.’”
“I took my child for vaccination, but my husband’s family was furious. They said I was risking our child’s future, that the swollen arm would never heal. It’s a battle between what I know is right and the fear they instill in us.”
Healthcare providers emphasized the importance of education on vaccine safety and efficacy. They recognized the need to address fears and misconceptions directly, providing clear and accurate information about immunizations. Providers expressed a commitment to engaging with the Batwa community in dialog and education to promote informed decision-making regarding pediatric immunizations.
“We’ve seen that many in the Batwa community fear the side effects of vaccines. It’s crucial for us to educate and reassure them about the safety and effectiveness of immunizations. We need to address these fears head-on with clear information so they can make informed decisions for their children’s health.”
“Sometimes after vaccination, rashes come up. But it’s nothing new. Our herbalists know how to treat these rashes. They’ve been doing it for generations.”
“Our approach is to engage in open dialogue with the Batwa community, listening to their concerns and providing accurate information. We want them to feel empowered to make decisions based on knowledge, not fear. Education is key to overcoming these misconceptions and promoting vaccination for the health of our children.”
Subtheme 2: Distrust in Western Medicine
A prevailing theme among the Batwa participants was a pervasive distrust in western medicine. They voiced a belief that traditional medicines are inherently safer than vaccines, citing a lack of representation of Batwa culture in healthcare centers. Many perceived medicines as profit-driven, leading to a dependency on western medical interventions that they viewed with suspicion. This distrust seemed to stem from a historical and ongoing sense of marginalization, where traditional healing methods are disregarded or belittled in favor of mainstream medical practices.
“We don’t want to go to those clinics for vaccinations. They say it’s for our health, but we know better. They just want to finish us off, especially us Batwa. They don’t care about us, they see us as less than human. Why else would they give us those injections that make us sick? It’s like they want to kill us slowly.”
“When a child is sick, their body is already weak. Injecting more into them is like signing their death warrant. We have seen it happen.” “I have seen generations grow in this village, and I have seen what these vaccines do. They weaken the child further when they are already fighting an illness. Our traditional healers knew better. They treated us with what the earth provided, not with foreign substances.”
Theme 2: Cultural Beliefs and Practices
The Batwa community’s perspectives on pediatric vaccination are tortuously connected to their profound cultural beliefs and practices. Traditional healing methods, steeped in centuries-old traditions significantly influencing their healthcare perspectives and behaviors. Within this context, 3 distinct sub-themes emerged: traditional healing practices and cultural perceptions of illness.
Sub-Theme 1: Traditional Healing Practices
The Batwa community also shared perspectives on traditional healing practices. They emphasized the effectiveness of these methods, which they believed were aligned with their cultural values. Traditional healing was seen as not only a means of treating illnesses but also as a way of preserving their heritage and identity. Participants highlighted the importance of supporting and caring for sick children within the community, often attributing illnesses to spiritual origins that required spiritual intervention or appeasement.
“A mzee (elder) knows what to do when a child is sick. We have our herbs for stomach aches, fractures, backaches, gapfura (a local term for a condition or illness), malaria, pneumonia. These are things we’ve always used, and they work.”
“Our traditional healing methods have been passed down for generations. When a child falls ill, we turn to our ancestral knowledge. It’s not just about curing the sickness; it’s about honoring our culture and ancestors.”
“Illnesses in our community are often seen as spiritual imbalances. We must perform rituals and use traditional herbs to restore harmony. This is how we’ve cared for our children for centuries, and it’s integral to our identity as Batwa.”
Sub-Theme 2: Cultural Perceptions of Illness
Illnesses were often viewed through a cultural lens among the Batwa, with spiritual explanations intertwined with physical symptoms. This perspective influenced their preferences for traditional remedies, which they deemed effective in addressing both the physical and spiritual aspects of illness. The community’s close-knit nature was evident in their shared responsibility for caring for sick children, emphasizing the communal approach to health and well-being.
“When a child falls ill, we see it as more than just a physical ailment. Our ancestors teach us that sickness can be caused by disturbances in the spiritual world. So, we turn to our traditional remedies because they not only heal the body but also cleanse the spirit.”
Within the Batwa community, supporting and caring for sick children was seen as a communal responsibility. Illnesses were often attributed to spiritual origins, and traditional remedies were viewed as effective interventions. Many believed in the necessity of spiritual intervention or appeasement in cases of illness.
“When a child in our community falls sick, it’s not just the parents' duty to care for them. We all come together as a community. We believe that our unity and prayers can help heal the child, especially when the illness is seen as coming from the spiritual world.”
Theme 3: Access and Infrastructure
The Batwa community’s perspectives on pediatric vaccination are deeply influenced by the accessibility and adequacy of healthcare infrastructure in western Uganda. Limited access to healthcare facilities, coupled with challenges in transportation and geographical isolation, significantly impact their ability to seek and receive immunization services for their children.
Sub-Theme 1: Geographical Barriers
The distance to healthcare facilities posed a significant challenge for the Batwa community. Lack of transportation, coupled with poor road conditions and challenging terrain, hindered access to immunization services. These geographical barriers created substantial obstacles for community members seeking healthcare.
“Sometimes, we have to walk for hours through dense forests and steep hills just to reach the nearest health center. It’s not easy, especially with young children. Many times, we just can’t make it in time for vaccinations.”
“The roads here are very bad, especially during the rainy season. When it rains heavily, they become muddy and slippery, making it impossible for vehicles to pass. So, even if we somehow arrange transport, we often get stuck on the way.”
Healthcare providers recognized the significant challenges posed by geographical barriers in reaching the Batwa community. They mentioned efforts to improve access, such as mobile clinics and outreach programs. However, providers also noted the ongoing struggle with inadequate infrastructure and limited resources, hindering efforts to provide equitable healthcare services.
“Sometimes, we have to walk for hours through the forest to reach a health center. The roads are difficult, especially during the rainy season. It’s not easy for us, especially with young children.” - “The mobile clinics are helpful, but they don’t come often enough. We need more consistent access to vaccines. Sometimes we hear about outreach programs, but they never reach our village.” -
Sub-Theme 2: Socioeconomic Constraints
A prevalent sub-theme related to the affordability of vaccines and socioeconomic constraints. Participants expressed the challenges of affording vaccines, citing opportunity costs of seeking vaccination and their overall economic status. The sentiment of “we are poor” resonated throughout discussions, highlighting the financial barriers that hindered access to immunization services.
“. . . . . . . . . . But where will we get the money? People don’t have enough to eat, let alone pay for health services. The District Officer of Health can’t appeal to empty pockets.”
“Every time we think of taking our children for vaccination, we also think about what we are losing by not working. We have to choose between feeding our family today or protecting them for the future. It’s not an easy choice when we are struggling to survive.”
“We want to vaccinate our children, but the cost is too much for us. We barely have enough for food and shelter, so spending money on vaccines feels impossible. It’s not just about the cost of the vaccine itself, but also the transport to get there, and the time away from work. Our poverty shouldn’t determine our children’s health, but it often does.”
Sub-Theme 3: Trust and Comfort With Healthcare Providers
Trust and comfort with healthcare providers emerged as a significant sub-theme. Participants expressed a strong preference for healthcare workers who were part of their own community, highlighting a sense of familiarity and understanding that they felt was lacking with external healthcare providers. One participant noted,
“Maybe they would feel free with people of their own, so they don’t have extension health workers within themselves.”
Health Extension Worker (
“Our children feel more comfortable when it’s someone from our own community, you know? These extension health workers mean well, but sometimes, they don’t understand our ways. Our kids get scared, they hide. If it was someone from the Batwa, maybe they would feel free, more at ease to take the vaccines.”
“Our kids, they see these Health Extension Workers (HEWs) as strangers. They don’t want to be touched by them, they don’t want their needles. But if it was someone from our community, they would feel safe, they would know it’s for their own good.”
These sentiments reflect the desire for healthcare providers who are not perceived as outsiders, but rather as integral members of the Batwa community. The use of “people of their own” emphasizes the importance of cultural congruence and shared identity in fostering trust.
Sub-Theme 4: Stigma and Stereotyping
The Batwa community reported feeling stigmatized and stereotyped in healthcare settings. Negative attitudes from healthcare providers were cited, with some participants feeling labeled as “dirty” or “unclean.” This perceived stigma contributed to a lack of trust in healthcare workers, affecting their willingness to engage with healthcare services
“When we go to the health center, some nurses treat us as if we are dirty people. They look at us differently, like we are not worthy of their care.”
“I remember one time, my child had a fever, and when I took her to the clinic, the nurse said, ‘Oh, you’re from the Batwa community, you must have brought this sickness from your village.’ It made me feel so small and unwelcome.”
Healthcare providers highlighted the challenges of building trust among the Batwa community. They acknowledged the stigma and stereotyping faced by Batwa individuals, often labeled as “dirty” or “unclean.” These negative attitudes from healthcare providers were cited as contributing factors to the community’s distrust in medical services, as seen in the excerpt below:
“. . . . . . . . . . They are unfairly labeled as ‘dirty’ or ‘unclean,’ and these attitudes seep into healthcare encounters. It’s disheartening because we know this hampers their trust in us, in modern medicine. We must work to change these perceptions.”
“The Batwa face enough challenges without the added burden of being stigmatized. As healthcare workers, we need to be aware of how our own biases can affect their willingness to seek medical care, including vaccinations. We must respect their traditional healing methods while educating on the benefits of immunization.”
The above reflects the acknowledgment by healthcare providers of the detrimental impact of stigma and stereotyping on the Batwa community’s trust in healthcare services. They highlight the need for healthcare workers to actively combat these negative perceptions and to approach the community with cultural sensitivity and respect for traditional healing practices.
Discussion
The study aimed to explore the Batwa community’s perspectives on pediatric vaccination and revealed key insights: misconceptions and concerns were prevalent, particularly regarding vaccine side effects and distrust in Western medicine, driven by community stories and rumors that favor traditional healing methods. Cultural beliefs intertwined with views on vaccination, with a strong preference for traditional remedies and communal care for sick children, often attributed to spiritual causes. Additionally, access and infrastructure barriers, such as geographical challenges and socioeconomic constraints, were significant obstacles to vaccination. Trust and comfort with healthcare providers, especially those from their own community, were crucial factors due to stigma and stereotyping in healthcare settings. These findings show a need to address misconceptions, improve access, respect cultural beliefs, and foster trust to enhance pediatric vaccination efforts among the Batwa community.
The prevalent theme from our results is the presence of misconceptions and concerns, particularly about vaccine side effects and distrust in Western medicine. Participants expressed significant fears of severe health risks associated with vaccines, often influenced by local stories and rumors, leading to a preference for traditional healing methods. These findings align with another study on pediatric vaccination perspectives across various cultural contexts, which also highlight common themes of misconceptions and distrust in Western medicine.20,21 Similar research on marginalized group in Kenya has shown recurring patterns of vaccine-related fears and a preference for traditional remedies. 22 These findings show a need for public health strategies that address these specific fears and misconceptions through culturally sensitive approaches. Targeted campaigns led by trusted community members or health practitioners could be pivotal in building trust and improving vaccination rates within the Batwa community and similar populations.
Our results show a strong relationship between cultural beliefs and the Batwa community’s views on vaccination, with a preference for traditional healing practices due to their perceived effectiveness and alignment with community values. Participants often attributed illnesses to spiritual origins, shaping their reliance on traditional remedies and communal care. 23 This how cultural beliefs influence vaccination attitudes, a trend also observed in other cultural contexts, such as among the Maasai in Kenya 22 and the San people in Southern Africa. 24 These groups similarly emphasize traditional healing and spiritual causes of illness, as seen in literature on cultural perspectives on healthcare. However, this study uniquely focuses on the Batwa community, a marginalized group with distinct practices. The findings suggest that successful vaccination programs should respectfully incorporate cultural beliefs, working with traditional healers and community leaders to integrate Western medicine with traditional practices, thereby building trust and improving vaccine acceptance. This approach has been effective in other contexts, indicating potential applicability to the Batwa community.
Our results show a relationship between cultural beliefs and practices and the Batwa community’s views on vaccination. The preference for traditional healing practices was underscored, highlighting their perceived effectiveness and alignment with community values. Many participants attributed illnesses to spiritual origins, shaping their reliance on traditional remedies and communal care for sick children. This study adds to the existing body of research by emphasizing the strong influence of cultural beliefs on vaccination attitudes, a common trend seen across different cultural contexts. 23 The emphasis on traditional healing practices and the belief in spiritual causes of illnesses aligns with literature on cultural perspectives on healthcare. 25 However, what distinguishes this study is its specific focus on the Batwa community in western Uganda, shedding light on a marginalized group with unique cultural practices. These findings have significant implications for public health interventions, indicating that successful vaccination programs should respectfully involve these deeply ingrained cultural beliefs. Working together with traditional healers and community leaders creates a chance to connect Western medicine with traditional practices, building trust and improving vaccine acceptance within the Batwa community.
Our findings reveal significant barriers to vaccination within the Batwa community in western Uganda, primarily related to access and infrastructure. Sub-themes such as geographical challenges and socioeconomic constraints emerged as key factors hindering immunization services. These results align with a growing body of research on vaccination barriers in diverse communities, emphasizing the pervasive impact of limited access to healthcare facilities due to remote locations, difficult terrain, and financial limitations. 26 These barriers not only impede vaccination rates but also reveal broader disparities in healthcare access and resources across different cultural contexts. The urgent need for targeted interventions to address these challenges is evident, with potential solutions including improved infrastructure through initiatives like mobile vaccination clinics or community outreach programs. Moreover, addressing socioeconomic factors, such as providing financial support or subsidies for vaccines, could alleviate the financial burden. By recognizing and proactively addressing these challenges, public health initiatives can strive toward more equitable vaccination coverage, thereby improving pediatric health outcomes within the Batwa community and similar marginalized populations.
Our findings show a critical aspect of healthcare access and utilization within the Batwa community in western Uganda: trust and comfort with healthcare providers. Participants strongly preferred providers from their own community, citing feelings of stigma and stereotyping in mainstream healthcare settings. This result resonates with a similar study emphasizing the significance of cultural competence and community representation in healthcare services.27 -29 The preference for local healthcare providers signifies a profound need for culturally sensitive care that recognizes and respects the unique experiences and perspectives of marginalized groups like the Batwa. This highlights the pivotal role of trust and familiarity in healthcare interactions, particularly in environments where historical marginalization and discrimination can influence healthcare-seeking behaviors. For public health interventions aiming to enhance vaccination rates and healthcare access, these findings stress the importance of involving community members as trusted healthcare providers, potentially bolstering vaccine acceptance and healthcare utilization within the Batwa community.
Conclusion
The results highlight the need for targeted strategies to address misconceptions about pediatric vaccination within the Batwa community. Key areas include educating about vaccine safety, addressing fears of adverse effects, and building trust in Western medicine. Efforts should focus on culturally sensitive programs and community engagement to foster understanding and dispel myths, enhancing vaccine uptake. Respecting cultural beliefs and using trusted Batwa care providers can improve comfort and trust in vaccination efforts. By integrating community members into healthcare delivery, particularly in administering vaccines, there is potential to improve accessibility and acceptance, boosting vaccination rates.
Strengths and Limitations of the Study
The study’s focus on the perspectives of the Batwa community in western Uganda providing valuable insights into a marginalized population’s views on pediatric vaccination. Also, the inclusion of various stakeholders such as mothers/caretakers, health extension workers, and community leaders provides a comprehensive view of the issues surrounding pediatric vaccination within the Batwa community. This diversity of perspectives enhances the credibility of the study’s findings. However, the current study had limitations including; While pilot-tested for effectiveness, the interview guide was not formally validated as a standardized questionnaire. This may impact the consistency and reliability of the data collected, as the guide was specifically tailored to the study’s context and population. While the study included a diverse range of participants, the sample size (15 mothers/caretakers, 8 health extension workers, and 3 community leaders) might be considered relatively small. A larger sample size could have provided even more comprehensive insights into the Batwa community’s perspectives on pediatric vaccination. The study’s focus on the Batwa community in a specific district of western Uganda limits the generalizability of its findings to other communities or regions. Cultural beliefs and practices can vary widely among different groups, so the findings may not fully apply to other marginalized populations. Despite these limitations, the study’s findings contribute valuable knowledge to the field of pediatric vaccination in marginalized communities, emphasizing the importance of culturally sensitive approaches to improve immunization rates and health outcomes.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241298834 – Supplemental material for Perspectives of Pediatric Vaccination Among the Batwa Community in Western Uganda: A Qualitative Study
Supplemental material, sj-docx-1-gph-10.1177_2333794X241298834 for Perspectives of Pediatric Vaccination Among the Batwa Community in Western Uganda: A Qualitative Study by Eustes Kigongo, Marc Sam Opollo, Viola Nalwoga, Marvin Musinguzi, Gad Kwizera and Amir Kabunga in Global Pediatric Health
Footnotes
Acknowledgements
The authors wish to acknowledge the study participants for taking time to participate in this study. We also acknowledge that we used ChatGPT to proofread the manuscript, but authors take responsibility for the analysis and all write-ups.
Author Contribution
EK was involved in the conceptualization, study design, data collection, analysis and manuscript writing. VN, MM and GK were involved in study design, developing and pretesting data collection tools, screening validity and reliability as well as refinement of tools. MSO and AK supervised the work, conducted data analysis, and reviewed the manuscript for submission. All authors were involved in the writing, review and final approval of the manuscript. Additionally, all authors made substantial contributions to the concept design, data acquisition, analysis and interpretation as well as refinement of the manuscript. Finally, all agreed to submit in the current journal.
Data Availability Statement
The transcripts used for this study are available from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This study was approved by Lira University Research Ethics Committee with approval number (LUREC-2023-87).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.