
Abstract
Background:
In Niger, a low-income country, occupational medicine is little known and practiced, particularly in the health sector, where healthcare workers are exposed to numerous occupational risks. This study aimed to assess knowledge, attitudes, and practices about occupational risks and diseases among healthcare providers working at the Hospital of Dosso (Niger) to determine their knowledge, attitudes, and practices level about occupational risks and diseases.
Methods:
A descriptive and quantitative census-based study was conducted among the 105 healthcare providers practicing at the hospital of Dosso between 1 April and 31 May 2023, using a self-administered questionnaire in the French language comprising a sociodemographic part and a knowledge, attitudes, and practices part about occupational risks and diseases. Knowledge, attitudes, and practices scores were calculated and Mann–Whitney U or Kruskal–Wallis tests were used to assess their association with sociodemographic characteristics.
Results:
In total, 83 healthcare providers agreed to participate in the study, with a participation rate of 79%. A total of 28% of participants had received training on occupational risks and diseases. The knowledge score about occupational risks and diseases showed that 55.4% of participants had a knowledge level varying from medium to high. The score of attitudes and practices showed that 68.7% of responders had an attitudes and practices level varying from medium to high about occupational risks and diseases. According to the composite score of knowledge, attitudes, and practices, 53% of participants had a knowledge, attitudes, and practices level between medium and high. A significant association was found between the composite score of knowledge, attitudes, and practices and the workstation occupied, mainly medical imaging service (p = 0.006).
Conclusion:
The study showed that 53% of responders had an overall level of knowledge, attitudes, and practices about occupational risks and diseases between medium and high. Among their sociodemographic characteristics, only the workstation occupied (mainly medical imaging service) was statistically associated with the composite score of knowledge, attitudes, and practices. Considering these findings, the administrators of the Hospital of Dosso must recruit an occupational medicine specialist to provide information and prevention visits on occupational risks and diseases to healthcare providers working in this institution.
Introduction
Occupational health and safety (OHS) aim to ensure, as far as possible, a safe and healthy working environment for all workers to prevent work-related illness and injury. 1 In a report published in May 2021, the World Health Organization (WHO) and the International Labor Organization (ILO) estimate that around 2 million people die every year from work-related diseases (81%) and injuries (19%), and the largest work-related burden of death was secondary to chronic obstructive pulmonary disease, stroke, and ischemic heart disease. 2 This report calls on countries and businesses to ensure compliance with international labor standards and WHO/ILO tools to improve and protect the health and safety of workers. However, in low and middle-income countries, the protection of the health and safety of workers remains a major public health concern. In Niger, a low-income country, occupational medicine is little known and practiced, particularly in the health sector, where healthcare workers are exposed to numerous occupational risks. These occupational risks, to which healthcare workers are constantly exposed, include biological, chemical, ergonomic, physical, and psychosocial risks. 3 As the backbone of any functioning health system, the protection of health and safety of health workers contributes to improving job satisfaction and retention of health workers to increase productivity. 4 Until January 2023, Niger had only 40 occupational physicians, including general medical doctors in specialization in the sub-region countries, because the occupational medicine specialty is not yet available in Niger. In hospital centers and health facilities, the departments of OHS and hygiene and sanitation are mainly managed by nurse technicians in these fields. This lack of occupational physicians in Niger creates problems in diagnosing occupational diseases and training and awareness of workers about occupational risks, particularly healthcare workers. In 2017, the Caisse Nationale de Sécurité Sociale (CNSS) of Niger recorded 160 cases of declarations of occupational accidents and occupational diseases or diseases suspected of being occupational in origin. Among these 160 declarations, 95% were occupational accidents with 8.6% of fatal cases (13/152), and 5% were occupational diseases or diseases suspected of being occupational in origin. 5 These declarations mainly come from workers of mining companies in Niger. In 2019, the CNSS recorded around 600 cases of occupational accidents. 6 Following this report of 2019, the Ministry of Employment, Labor, and Social Protection launched an awareness campaign for the workers intending to minimize the incidence of occupational accidents in the City of Maradi (the economic capital of Niger).
In Niger, few studies have been carried out on the knowledge, attitudes, and practices (KAP) about occupational risks and diseases (ORD) among healthcare providers (HPs), and none have been published. The present study aimed to assess the KAP about ORD among HPs working at the Regional Hospital Center (RHC) of Dosso (Niger) to determine their KAP level about ORD.
Materials and methods
Description of the study location
The study was carried out in the RHC of Dosso (Niger). The region of Dosso is located in the southwest of Niger, which covers an area of 121,844 km² (8.7% of the total area of Niger) with 3,056,070 inhabitants in January 2023. The RHC of Dosso was created in 1947 under the name of the Health Center of Dosso and became a District Hospital Center in 1972, and in 2002 became RHC. This hospital is one of the RHCs of Niger that represent the second level of healthcare recourse in the health pyramid of the country. The main missions of the RHC of Dosso are to provide secondary care services and to receive medical and surgical references from the eight departments of the region of Dosso. Another mission of the RHC of Dosso is to serve training terrain for health trainees. The staff of RHC of Dosso is composed of 130 healthcare workers, including 105 HPs, who are the target population of the present study.
Study design
A descriptive and quantitative census-based study was conducted between 1 April and 31 May 2023, at the RHC of Dosso (Niger) among the 105 HPs, including medical doctors, polyvalent nurses, and specialized nurses. Information regarding the purposes of the study is provided to each participant to obtain verbal consent to participate in the study. When the participant agreed to participate in the study, a self-administered questionnaire was provided for him, which he (she) completed himself and anonymously. We stay beside the participant when he (she) completes the questionnaire, and at the end, we recover the completed form.
Inclusion and exclusion criteria
This study was limited to only HPs aged ⩾18 years working at the RHC of Dosso. The study did not include drivers, cooks, cleaners, and security agents because most of them are illiterate. In addition, there were six non-medical technicians and hospital administrators who were not included in the study due to their small number.
Study instrument and data collection
To conduct the present study, we established, while drawing inspiration from the results of previous studies,7,8 a structured self-administered questionnaire comprising two parts: the first on sociodemographic characteristics and the other on KAP about ORD (details in Supplemental Material). Because there are several local languages in Niger, among which the largest of them have no own writings, a self-administered questionnaire in French language (the official language used in all education programs of the country) was used in the present study. The study instrument was pretested among 15 HPs working at the Integrated Healthcare Center of Kore Maïroua (Kore Maïroua, Niger). Errors and ambiguous questions were corrected before starting data collection among HPs working at the RHC of Dosso (Niger). The sociodemographic part comprised seven items: age, gender, marital status, profession, number of years in the profession, workstation occupied, and number of years in the workstation occupied. Concerning the profession, three socio-professional categories were considered in the study: (1) the doctors’ category, including general medical doctors, specialist physicians, and surgeons; (2) the polyvalent nurses’ category, including certified nurses and state-qualified nurses, commonly known in Niger as superior technicians in nursing care; and (3) specialized nurses’ category, commonly known as superior technicians in Niger, including nurses in anesthesia and critical care, ophthalmology, stomatology, otolaryngology, dermatology, the nurses of operating block, laboratory technicians, radio manipulators (or technicians in Radiology), physiotherapists, etc. The KAP part about ORD comprised 30 questions, 20 on knowledge, 5 on attitudes, and 5 on practices (questions are listed in eTable1 and eTable2 in Supplemental Material). The questions were simple, with preferably “Yes” or “No” responses, or choose answers from a list of proposed answers. For each adapted or correct answer to a question, 1 point was awarded and 0 points for an incorrect or unsuitable answer. The knowledge questions were used to establish a knowledge score for each participant, with a potential score varying from 0 to 20, with a higher score indicating a good level of knowledge about ORD. Participants were grouped into three groups according to their knowledge scores: (1) group of respondents with a score <10 (10 corresponds to the overall median score of knowledge of all respondents), (2) group of respondents with a score between 10 and 14 (14 corresponds to the summation of 10 + 4; 4 corresponds to (lower quartile)/2 = 8/2), and (3) group of respondents with a score between 15 and 20 (15 corresponds to the summation of 10 + 4 + 1 and 20 corresponds to the maximum knowledge score). Group 1 includes respondents with a low level of knowledge and medium and high levels for groups 2 and 3, respectively. The 10 questions on attitudes and practices were used to establish an attitudes and practices score, with a potential score varying from 0 to 10, with a higher score indicating a good level of attitudes and practices toward ORD. Thus, participants were divided into three groups according to their attitudes and practices: (1) group with a score <5 (5 corresponds to the overall median score of attitudes and practices), (2) group with a score between 5 and 7 (7 corresponds to the summation of 5 + 2; 2 corresponds to (lower quartile)/2 = 4/2), and (3) group with a score between 8 and 10 (8 corresponds to the summation of 5 + 2 + 1 and 10 corresponds to the maximum score of attitudes and practices). These groups indicate, respectively, a low, medium, and high level of attitudes and practices. The 30 questions assessing KAP toward ORD were used to calculate a composite score of KAP for each participant, with a potential score varying from 0 to 30, with a higher score indicating a good level of KAP about ORD. Three groups were formed according to the composite score of KAP: (1) group with a score <15 (15 corresponds to the overall median of composite score of KAP), (2) group with a score between 15 and 21 (21 corresponds to the summation of 15 + 6; 6 corresponds to (lower quartile)/2 = 13/2 ≈ 6), and (3) group with a score between 22 and 30 (22 corresponds to the summation of 15 + 6 + 1 and 30 corresponds to the maximum score of composite score of KAP). These groups indicate a low, medium, and high level of KAP, respectively.
Ethical approval
The present study was approved by the Ethical Committee of the Direction Régionale de la Santé Publique (DRSP) of Dosso (No. 005/DRSP/P/AS) and followed the Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. All participants provided their verbal informed consent to participate in the study. This procedure for obtaining verbal informed consent from participants was approved by the Ethical Committee of the DRSP of Dosso.
Statistical analysis
Data were entered into the Excel sheet and then imported into the IBM SPSS statistical software package (IBM SPSS Statistics for Windows, Version 25.0; IBM Corp., Armonk, NY, USA) for analysis. In the descriptive analyses, the categorical variables were expressed as percentages and the continuous variables as mean ± standard deviation or medians with interquartile ranges (IQRs). The Shapiro–Wilk test was used to assess the normality of data distribution. The Mann–Whitney U or Kruskal–Wallis tests were used to assess the association between KAP scores and sociodemographic variables. The p-values <0.05 were considered statistically significant.
Results
Sociodemographic characteristics of participants
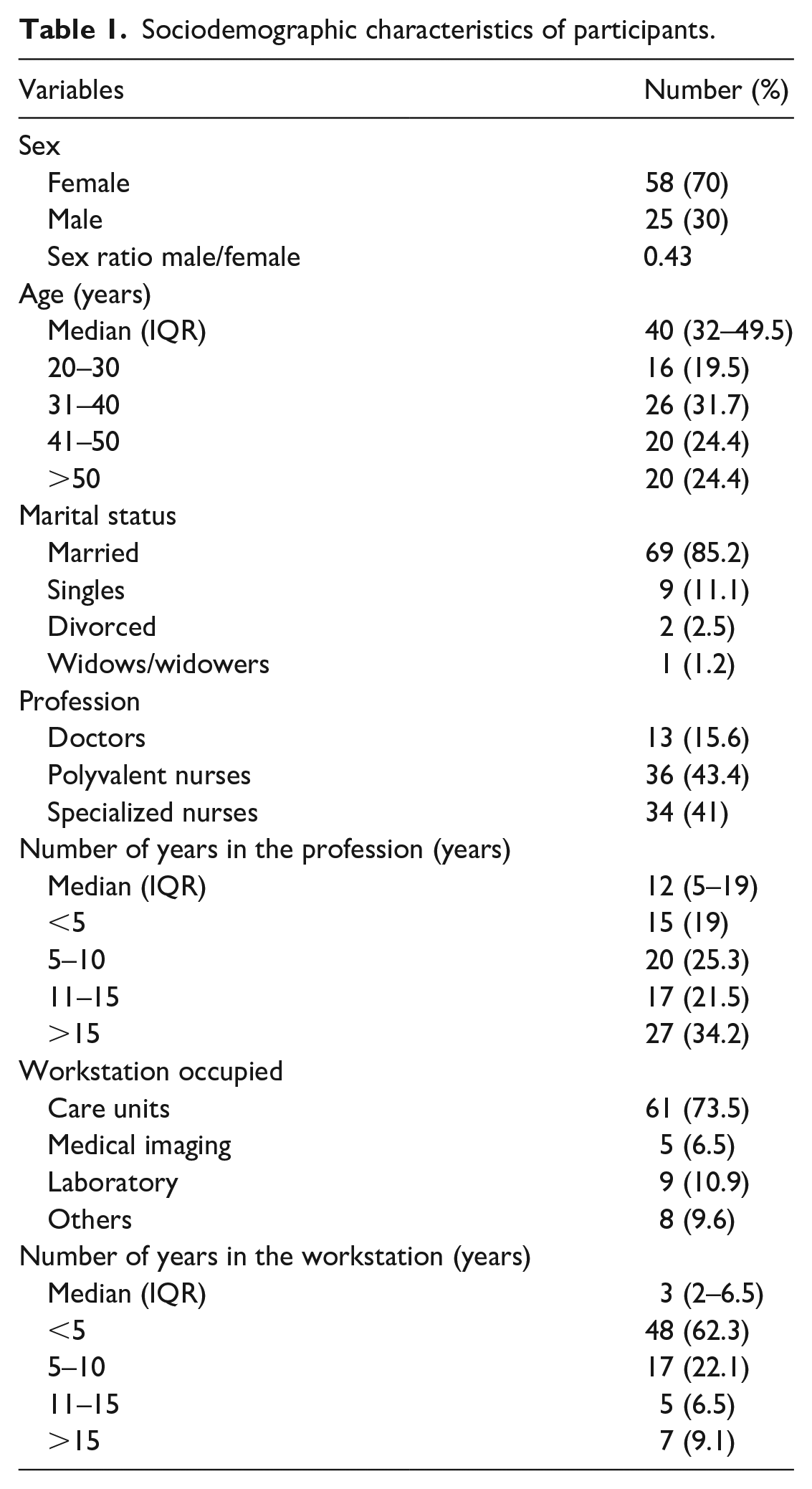
Of the 105 HPs practicing at the RHC of Dosso, 83 had agreed to participate in the study, with a participation rate of 79%. Table 1 details the sociodemographic characteristics of the participants. The median age of participants was 40 years (IQR: 32–49.5), with a female predominance (sex ratio male/female at 0.43). In total, 85.2% of participants were married. Polyvalent nurses were more represented (43.4%). The median number of years in the profession was 12 years (IQR: 5–19). In total, 73.5% of participants worked in care units, with a median number of years in the workstation of 3 years (IQR: 2–6.5).
Sociodemographic characteristics of participants.
Knowledge of ORD
eTable1 (Supplemental Material) details the answers to the questions on knowledge about ORD. Only 43.2% of participants knew the difference between an occupational disease and an occupational accident. However, 56.3% of participants knew the difference between an occupational disease and a disease suspected of being occupational in origin. A total of 16% of participants did not know that occupational risk could be the cause of an occupational disease, and 37.3% thought that exposure to physical factors (such as vibration, noise, bright lights, etc.) outside the workplace could be the cause of occupational diseases. In total, 11.1% of participants did not know the occupational risks to which they are exposed. Less than one-third (27.3%) of participants knew that the declaration of an occupational disease is made by the worker, while only 10% knew that the declaration of a disease suspected of being occupational in origin contributes to modifying the tables of compensable occupational diseases. In total, 16.2% of participants thought that a victim of an occupational disease should be dismissed with increased compensation, while 25% knew nothing about it.
The median score of knowledge about ORD was 10 (IQR: 8–12), with 53% of participants having an average level (score between 10 and 14) of good knowledge of ORD (Table 2). We did not find a statistically significant association between participants’ sociodemographic characteristics and their knowledge score about ORD (Table 3).
Score of KAP about ORD.

Score of knowledge about ORD by sociodemographic characteristics.

Attitudes and practices regarding ORD
eTable2 (Supplemental Material) details the answers to the questions on attitudes and practices regarding ORD. A total of 13.4% of participants would not advise a colleague who develops symptoms of any disease in the practice of its profession to consult the occupational health service. In total, 7.3% of participants thought that the declaration should not be made when they are diagnosed with an occupational disease. More than 4/5 (91.4%) of the participants had never consulted the document that assesses the occupational risks concerning their workstation. In total, 72% of participants had never received training on occupational risks and occupational diseases. Only 15.7% of the participants had benefited from a pre-recruitment (hiring) medical visit. A total of 19.5% of respondents report not respecting occupational risk prevention measures in the exercise of their profession. In total, 6.4% of respondents report that information and prevention visits on ORD are not helpful for a HP in the practice of their profession.
The median score of attitudes and practices about ORD was 5 (IQR: 4–6) and 63.9% of the participants had an average level (score between 5 and 7) of good attitudes and practices about ORD (Table 2). The median score of attitude and practices of participants working in medical imaging was significantly higher than those of participants working in the laboratory, care units, and other units such as pharmacy, social service, etc. (p = 0.006; Table 4).
Score of attitudes and practices about ORD by sociodemographic characteristics.

The median composite score of KAP about ORD was 15 (IQR: 13–17), and 50.6% of participants had an average overall level of KAP (score between 15 and 21). The median composite score of KAP of participants working in medical imaging was significantly higher than those of participants working in the laboratory, care units, and other units (p = 0.006; Table 5). The median composite score KAP of specialized nurses seemed to be higher than those of polyvalent nurses and physicians (p = 0.057).
Composite score of KAP about ORD by sociodemographic characteristics.

Discussion
In this census-based study, we examine, through a self-administered questionnaire with simple answers, the views held about ORD of HPs practicing in the RHC of Dosso to determine using scores their overall level of KAP about ORD. The study respondents were mainly nurses and females. These results are consistent with those reported by Aluko et al.7 in Nigeria.
General knowledge of respondents about ORD
In our study, 55.4% of the respondents had a medium to high level of knowledge about ORD. Around 57% of participants did not know the difference between an occupational disease and an occupational accident. Although only about half of the respondents of our study had a medium to high level of knowledge about ORD, ergonomic and psychosocial risks appear to be well recognized by the respondents as being occupational risks in 58.5% and 58.8% of cases, respectively. Kamese
11
reports in 2020 in Guinea-Conakry a result close to ours (51.1%). Aluko et al.
7
reported,
Attitudes and practices toward ORD
In our study, 68.7% of participants had a medium to high level of good attitudes and practices toward ORD. The hiring medical visit does not seem to be a routine procedure, and 79.3% of respondents had not benefited from it. In addition, only one (1.4%) participant had benefited from a medical visit when returning to work after childbirth, disease, or occupational accident. Ibrahim Souley 8 reported 52.6% of participants that had not benefited from a hiring medical visit, and 11.2% that benefited from a medical visit when returning to work after childbirth, disease, or absence of more than 30 days. This situation shows that, in Niger, most hospitals did not have occupational physicians but nurse technicians in OHS and hygiene and sanitation who are not authorized to provide certificates of aptitude for employment. The study findings showed that 13.4% of participants would not advise a colleague who develops symptoms of any disease in the practice of its profession to consult the occupational health service, 7.3% thought that the declaration should not be made when they are diagnosed with an occupational disease, and 91.4% had never consulted the document that assesses the occupational risks concerning their workstation.
KAP toward ORD by sociodemographic characteristics
In our study, 53% of participants had an overall level of KAP about ORD between medium and high. Only 2.4% of the respondents in our study had a high level of KAP about ORD, while Aladini et al. 10 reported a high level in 30.3% of their respondents. This difference could be explained not only by the fact that the questionnaires of the two studies are different but also by the difference in the methods of categorizing participants into groups with low, medium, and high levels of KAP.
The study showed that HPs working in the medical imaging service (mainly represented by radio manipulators or technicians in Radiology because the RHC of Dosso only has one radiologist) had a significantly higher level of KAP about ORD than HPs working in the care units, laboratory, or other services (including pharmacy, physiotherapy, etc.). HPs working in care units (mainly represented by polyvalent nurses) had the lowest level of knowledge about ORD. This could be explained by the fact that HPs working in the medical imaging service are more informed about ORD, probably because they received a more detailed module on occupational safety and health during their training course.
Limitations of the study
First, the relatively small sample size is one of the limitations of the study that could be explained by: (1) the RHC of Dosso is a small hospital of 130 care workers, including 105 HPs, and (2) the study did not include drivers, cooks, cleaners, non-medical technicians, security agents, and hospital administrators. Secondly, the results of the study need to be interpreted with caution due to the use of a structured self-administered questionnaire, which may have a risk of bias in the responses of the participants. Third, the study was conducted in a secondary healthcare facility, a model of average practice in the healthcare sector, and for this purpose, the results of this study do not reflect the knowledge level of Nigerien HPs. The main strength of this study is that it is the first study assessing the KAP regarding ORD among Nigerien HPs working in a secondary healthcare facility. Thus, the results of this study would attract the attention of administrators of RHCs in Niger to take necessary measures to provide information and prevention sessions on ORD to HPs working in their institutions.
Conclusion
The present study showed that 53% of HPs working at the RHC of Dosso had an overall level of KAP about ORD between medium and high. Among the sociodemographic characteristics of the HPs, only the workstation occupied (mainly medical imaging service) was statistically associated with the composite score of KAP. Considering the results of the study, the administrators of the RHC of Dosso must recruit an occupational medicine specialist to provide information and prevention visits on ORD to HPs working in this institution, specifically related to their workstations. It is also primordial in Niger to strengthen occupational medicine courses in the training program for HPs to provide them with knowledge about ORD and ensure their health and safety at work. Healthcare workers must consult, on their own initiative, the document related to ORD to have a good understanding of the extent of the occupational risks to which they are exposed. Larger studies on several hospitals in Niger are needed to determine the level of knowledge of the healthcare workers about ORD to determine the weak points to be corrected.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231224549 – Supplemental material for Assessment of knowledge, attitudes, and practices of occupational risks and diseases among healthcare providers of the Regional Hospital Center of Dosso, Niger
Supplemental material, sj-docx-1-smo-10.1177_20503121231224549 for Assessment of knowledge, attitudes, and practices of occupational risks and diseases among healthcare providers of the Regional Hospital Center of Dosso, Niger by Halimatou Nassirou-Sabo and Moussa Toudou-Daouda in SAGE Open Medicine
Footnotes
Acknowledgements
We thank the healthcare providers of the Regional Hospital Center of Dosso for their contribution to the realization of this work by agreeing to participate in the study.
Author contributions
H.N.-S. substantially contributed to the conception, drafting, design of the work, the acquisition, analysis, and interpretation of data for the work and M.T.-D. contributed to the study design, interpretation of data for the work, drafting the work, and revising it critically for important intellectual content. The authors read and approved the final submitted version of the manuscript.
Data availability statement
The data that support the findings of the study are available upon a reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The present study was approved by the Ethical Committee of the direction régionale de santé publique (DRSP) of Dosso (No. 005/DRSP/P/AS) and followed the Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. All participants provided their verbal informed consent to participate in the study. This procedure for obtaining verbal informed consent from participants was approved by the Ethical Committee of the DRSP of Dosso.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.