
Abstract
Background. This study assessed determinants of timely vaccination among children aged from 0 to 23 months in Wolaita Zone Public hospitals, southern Ethiopia: A facility-based cross-sectional study in the study area. Methods and material. An institution-based cross-sectional study was undertaken in Wolaita Zone Public hospitals from December 12 2023 to January 12 2024, G.C. Study subjects were randomly selected through systematic sampling method. Data were gathered by structured questionnaire, entered into Epidata 4.6 and transferred to SPSS 23 for analysis. An adjusted odds ratio (AOR) along with a 95% confidence interval at a P < .05 was used to declare significance level. Results. This study found that 71.5% of children were vaccinated timely. Time to reach the health facility, place of delivery, ANC follow-up, attitude, and knowledge of women, significantly attributed to timely vaccination. Conclusion. About 71.5% of study participants vaccinated their children on the national recommended vaccination schedule. Highly strategic interventions should be taken in improving timely vaccination and identified factors.
Plain Language Summary
Vaccine-preventable diseases are a serious problem that contributes to the death rate of children in developing countries such as Ethiopia. Some studies have shown that these VPDs are one of the factors affecting children’s health. Vaccination at the appropriate time is one of the key methods for promoting children’s health by improving the level of body immunity. Various studies have been conducted on the full coverage of vaccination in Ethiopia, but there are limited data on timing of vaccination and its predisposing factors in Wolaita Zone Public hospitals, southern Ethiopia. Participants were accessed through systematic sampling methods. The data were collected through administering structured questionnaires, and the Epi data V4.6 and SPPSS V.25 were used to enter and analyze, respectively.
In this study, we estimate the prevalence and factors associated with the vaccination timeliness in children between the ages of 0 and 23 months in the study area. The results showed that 71.5% of children were vaccinated on time. Possible factors identified for timely vaccination are the time to reach the health facility, the birthplace, and the follow-up of the ANC, the attitude of women and knowledge of the vaccine period. In summary, vaccination time is a gap in the field of research. Consequently, it is necessary to improve vaccines in time and to identify factors. This in turn promotes the health of children.
Keywords
Introduction
The timeliness of vaccination refers to a child receiving their vaccination at the recommended time and is calculated by subtracting the date of birth from the vaccination date. Vaccines were administered on time if they were received within the first year of life and within the time limits set by the World Health Organization (WHO). 1 Vaccination timeliness indicates administering vaccines at the earliest age possible and adhering to the recommended intervals between doses. It is an important mechanism for developing protective antibodies and providing effective disease protection in children. Only when an effective vaccine is administered at the right time it will result in disease protection by strengthening community immunity and preventing the spread of infectious diseases, particularly during illness outbreaks; increased adherence to vaccination timeliness protects children before exposure and lowers morbidity.2 -5
Immunization is crucial, especially for diseases like pertussis and Haemophilus influenza type B (Hib), which cause the majority of deaths within the first 6 months of life. Additionally, prompt vaccination protects infants who are too young to receive a full vaccination and maximizes herd immunity. 6 On the other hand, early immunization may not produce an antibody that protects against the diseases. 7 Because vaccinations given too soon or without a suitable time interval between doses, may not be totally protective (lead to a misleading sensation of protection). 8 And also, postponing immunizations raises a person’s risk of contracting a potentially fatal VPD. 9 These will lead to lower community-level herd immunity and intervention success rates, 10 full vaccination series completion rates, 11 and elevated risk of infectious illnesses under control. 12
Globally, immunization is one of the maximum cost-effective techniques in growing infant survival, saving 2 to 3 million infant deaths every year from vaccine-preventable illnesses (VPDs). 13 A vaccine can also additionally have avoided one disorder out of each twenty that claimed an infant’s life in 2019. 14 Even with the excessive vaccination rate of 85% global in 2017, a few children nevertheless experience delays in receiving fundamental vaccinations, especially in low-income countries.15 -18 Timeliness of vaccination is a measure of the quality of vaccination programs, but it has received less attention than other program performance indicators. 16
Previous literature shows that 87.5% in Ghana, 94% in Israel, 82% in Philadelphia, 64% in Ethiopia, 71% in New Zealand, and 87% in Uganda were vaccinated on time.19 -24 Previous studies have shown that the timeliness of vaccination is associated with place of delivery, lower education level, antenatal care visits, unplanned pregnancy and male gender of the child, and the oldest age of the mother/caregiver, maternal age, vaccine hesitancy, multipara, residency, and the poorest quintile. However, these variables vary depending on the study setting.5,17,25 -29 In Ethiopia, vaccinating children at an adequate time interval is the major method in minimizing avoidable childhood mortality from measles, pneumonia, diarrheal illnesses, and other VPDs. 30
According to Ethiopia Demographic Health Survey (EDHS) 2016 report, the overall timeliness of vaccination has improved with coverage increasing from 24% in 2011% to 39% in 2016. 31 However, Diphtheria Tetanus Pertussis (DTP1), Oral Polio Vaccine (OPV1), and measles vaccinations were often delayed beyond the WHO recommended schedule. 31 Beyond the individual immunity level, previous research emphasizes the importance of timely vaccination as a key factor in preventing infectious diseases on a population level. While many countries have high vaccine coverage, there are significant delays in age-appropriate vaccination administration, indicating a need for improvement.26 -29
In general, developed countries have given cautious concept to the timing of childhood vaccinations; however, comprehensive research in low-income countries, especially Ethiopia has been few. 31 Untimely vaccinations have significant impact on immune system functioning and are likely to contribute greatly to the preventable disease burden in Ethiopia, allowing for transmission among those in the age group at which they are the most vulnerable to severe disease with tragic consequences. 32 Previously, most studies conducted in Ethiopia assessed complete vaccination coverage and related factors; however, there is limited information about timely vaccination and its influencing factors, illustrating an essential research gap that must be filled. Full vaccination is most effective in identifying the number of children vaccinated, however it does not provide adequate information about the countrywide vaccination schedule, which is critical for protecting children from vaccine-preventable illnesses if they receive vaccines within the recommended timeframe. In addition, this study included children aged 0 to 11 months, which was excluded from previous research performed in Ethiopia. In order to help program implementers and frontline health workers recognize vaccination timelines and its related factors to plan for default tracing mechanisms. So, this study aimed to evaluate determinants of timely vaccination among children aged from 0 to 23 months in Wolaita Zone Public hospitals, southern Ethiopia: A facility-based cross-sectional study.
Methods and Materials
Study Area, Design, and Period
From December 12, 2023 to January 12 2024, G.C, A facility-based cross-sectional study was conducted in Wolaita Zone Public hospitals, southern region, Ethiopia. Wolaita Zone is located from 328 km from capital city of Ethiopia, Addis Ababa. Based on the 2020 Central Statistical Agency (CSA) report, the population of Wolaita Zone was projected to be 5 385 782. From these, 2 687 021 populations are accounted by males and 2 698 261 populations were females. Currently, there are 8 public hospitals in this zone including Wolaita Sodo university comprehensive specialized hospital (WSUCSH), Bodit primary hospital PH, Gasuba PH, Tebela PH, Bale PH, Halale PH, Bombe PH, and Bitana PH. These public hospitals have been providing health service for all Wolaita zone population and some other surrounding zones.
Source of Population
The source of population for the study was mothers/caregivers with children aged between 0 and 23 months in Wolaita zone public hospitals.
Study Population
All children aged between 0 and 23 months who attended EPI in Wolaita zone public hospitals on the study period.
Inclusion and Exclusion Criteria
Inclusion criteria
The inclusion criterion was all mothers/care givers with children aged 0 to 23 months came to each study area for EPI service during data collection period.
Exclusion criteria
Immune-compromised children, such as a child with clinical AIDS. This population is in risk for developing severe infection if they receipt live vaccines. Thus, most of the time, this group is excluded from receiving vaccination timely.
Those mothers/caregivers who are unable to respond after details of the study purpose were provided during data collection were excluded.
Sample Size and Sampling Technique
Based on the following assumptions, the sample size was calculated using a population proportion calculation formula. A 95% confidence interval (CI), an error rate of 5%, and a population proportion of 44% were taken from the previous study. 24 Based on the calculations, 378 participants were needed for the study. Accordingly sample size was calculated as:


So, n = 378
Where:-
n = sample size
p = vaccination timelines = 44%
z = confidence interval at 95%
w = marginal errors (5%)
Since the last 6 months baseline number of children in EPI of the selected health facilities was 3615, which is less than 10,000 therefore by using finite population correction formula the final sample size was calculated as:-

where N is the source population which is n = 378/1 + 378/3615 = 342 children’s.
By adding 10% of non-response rate and which is 342 + 34 = 376. So the final sample size was 376 children.
Among 8 public hospitals, 4 public hospitals were selected by lottery methods. The average monthly patient flow to EPI for consecutive 6 months was determined. The estimated number of client is 3615 (from this WSUCSH = 1790, Bombe primary hospital = 679, Tebela primary hospital = 589 and Bitana primary hospital = 556) then final sample size proportional allocated to these service center by considering their monthly client flows. Eventually, the subject was taken by systematic random sampling, thus every Kth client (based on their population proportion) who came to each public hospital was recruited as study unit in each service center till total sample size for the study was obtained (Figure 1).
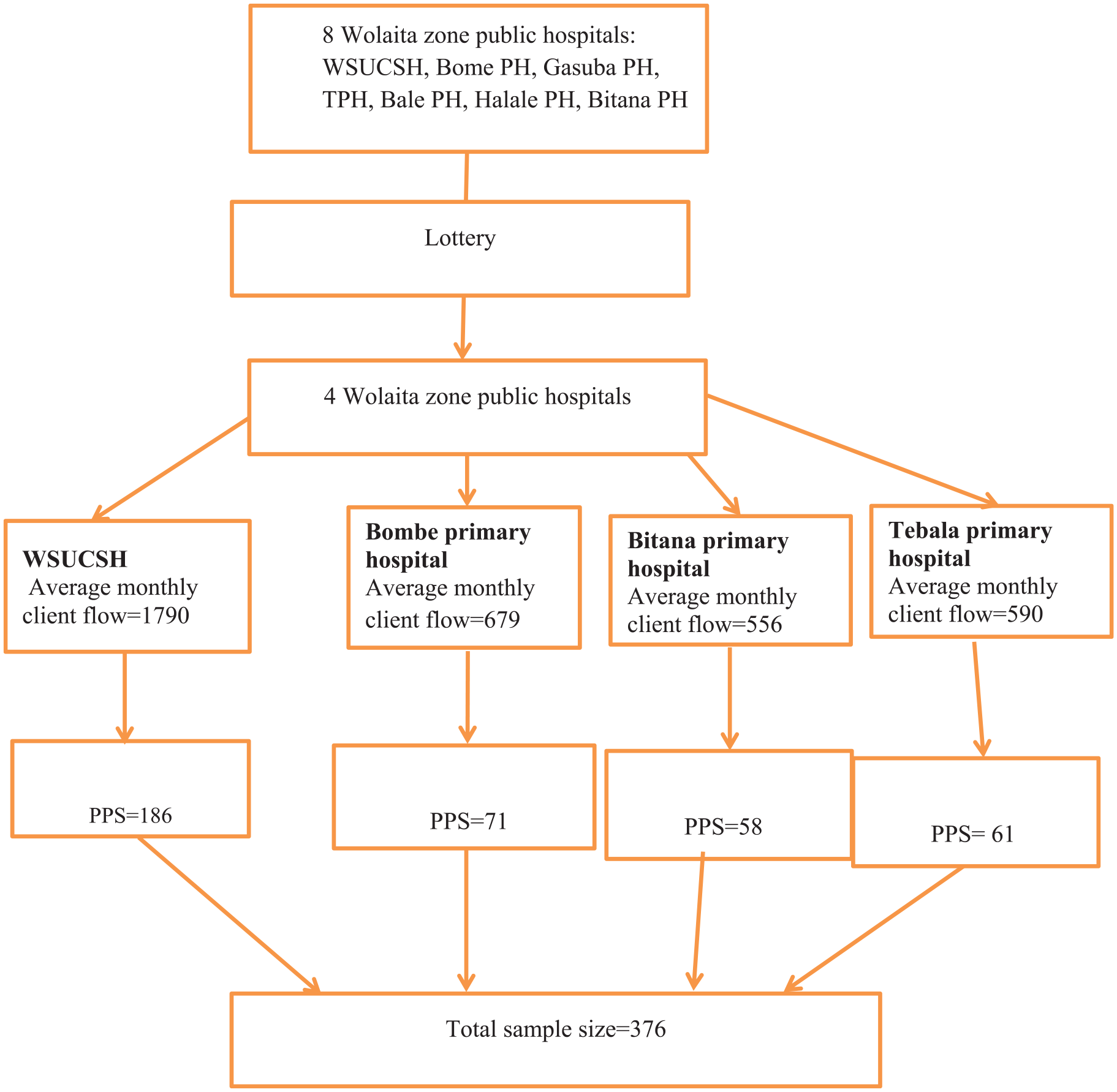
Schematic presentation of sampling techniques of study on vaccination timeliness in Wolaita zone public hospitals.
Data Collection Tool and Procedure
The tool was developed after reviewing different literature.25 -30 It consisted of 4 parts, which include socio-demographic characteristics, obstetric characteristics, knowledge and attitudinal factors about vaccination timeliness. The questionnaires have been first prepared in English after which translated through the specialists into local languages (Wolaita version) after which translated again into English to test for consistency. Data have been gathered through face-to-face interviews and referring immunization card using pretested, structured questionnaires after the women have been briefed about the studies on the time of the EPI visit. Data have been collected through 4 BSC midwives who should hear, speak, and read the local language and M.Sc. nurses who already had data collection and supervising experience respectively.
If the vaccination card was available, the data collector copied the dates of each vaccination received in the respective section of the mothers/caregivers questionnaire. If a vaccination was ot recorded in the child immunization card, the mothers or care givers was asked to recall whether particular vaccination had been given. If the mother or caregivers was unable to present the card, she was asked to recall whether the child had received BCG, Polio, DPT-HepB-Hib, measles, pneumococcal, and rotavirus vaccines. If she indicated the child had received the Polio, DPT-HepB-Hib, measles, pneumococcal, and rotavirus vaccines, she asked to the numbers of doses that the child received.
Data Quality and Analysis
Training was held for data collectors and supervisors to ensure data quality. The questionnaire was initially pretested on 5% of women at Bodit Primary Hospital. Throughout the data collection process, the principal investigator and supervisor provided frequent monitoring and observation. After daily data collection, each questionnaire was checked for completeness and accuracy.
Completeness and consistency were checked, coded, and entered into Epidata Version 4.6 and exported to SPSS Version 23 for analysis. One variable with a P-value less than .25 in the bivariate analysis was recruited for the multivariable logistic regression analysis model. An adjusted odds ratio (AOR) along with a 95% confidence interval at a P-value less than .05 in the multivariable logistic regression model was used to declare factors significantly associated with the vaccination timeliness.
Study Variables
Dependent variable
Vaccination timelines.
Independent variable
Socio-demographic characteristics, children and obstetric related factors, knowledge about and attitude toward timely vaccination.
Operational Definitions
Vaccination timeliness
The program of immunization are recommended as WHO at minimum interval at birth (BCG and Polio0), 6_weeks (Penta1, Polio1, Rota1, PCV1), 10_weeks (Penta2, polio 2, Rota2, PCV2), 14_weeks (penta3, Polio3, IPV, PCV3), and Measles at 9_months, and 15 months1,5 (Table 1).
National and WHO Recommended Vaccination Timelines.

Vaccination timely (age-appropriate vaccination)
The delivery of vaccines within the World Health Organization (WHO) approved time frames and checked by immunization card. And/or the delivery of vaccines within 1 month after the minimum age to administer the dose as recommended by WHO.1,5
Vaccination untimely (age-inappropriate vaccination)
The delivery of vaccines earlier and/or delayed than the recommended age by WHO.1,5
Delay vaccination
Delay vaccination was measured as not having received the recommended vaccine doses within 1 month beyond the minimum age.1,5
Early vaccination
Maternal knowledge about vaccination timeliness
Maternal knowledge about vaccination timeliness was measured using 9 questions related to vaccination timeliness. Each correct answer was given a point of one (1) and zero (0) point was given to the incorrect ones. Those who scored less than the mean value were categorized as having poor knowledge and those who scored above the mean were categorized as having good knowledge. 5
Maternal attitude toward vaccination timeliness
Maternal attitude toward vaccination timeliness was assessed using 6 items rated on a five-point Likert scale as [1] strongly agree, [2] agree, [3] not sure, [4] disagree, and [5] strongly disagree. For the purpose of ease of analysis, attitude of mothers toward vaccination timeliness items were condensed into 2 categories as “agree,” which includes strongly agree and agree whereas “disagree,” comprises “strongly disagree, disagree, and not sure.” Furthermore, the attitude measurement Likert scale was summarized as “positive attitude” (those who scored the mean and above on attitude measuring items) and “negative attitude” (those who scored below the mean on attitude measuring items). 5
Ethical approval and participant consent
An ethical clearance was obtained from the institutional review board of Wolaita Sodo University with the reference number of 9/877/2023 and then submitted to the Wolaita Zone Health Office. Then a permission and cooperation letter was obtained from the zonal health office and distributed to each selected Hospital prior to data collection. Written informed consent was obtained from the study participant and data was collected after assuring the confidentiality nature of responses. All methods throughout the study were carried out in accordance with relevant guidelines and regulations.
Result
Socio-Demographic Characteristics
Of 376 mothers/caregivers, all participants responded to the interviews, making a response rate of 100%. Table 1 shows the social and demographic characteristics of the study participants. Among the sample, 186(49.5%) were Relationship with Mother, 34 (9%) were Relationship with Father, 72 (19.2%) were Relationship with Relative, and 84 (22.3%) were Relationship with Sister or brother And from a total of 376 study participants, 9 (2.4%) were Age of mother below 18 115(30.6%) were the age of 18 to 28 169(44.9%) were the age of 28 to 38, and 83 (22.1%) had 38 and above age of mother. The majorities respondent 345 (92%) were married and 12(3%) were widowed. 267 (71%) were protestant religion followers and 16 (4.2%) were Muslim religion followers (Table 2).
Socio Demographic Characteristics of the Respondent Wolaiata Zone Public Hospitals, (n = 376).

Obstetric Characteristics of the Study
Most of the children, 98.7%, were born in a health facility, while 1% was born at home. Furthermore, the majority of children had ever received more than 1 dose of vaccine, and of these, only 2% did not possess a vaccination card at the time of the study. Among 376 respondents (100%), 367 (97.6%) reported their child had received at least 1 vaccine, and 9 (2.4%) had not. Of the 376 respondents (100%), 367 (97.6%) reported that their child had received at least 1 vaccination, with 9 (2.4%) reporting that their child had not been vaccinated. Of the 376 respondents (100%), 368 (98%) were able to provide vaccination card, while 8 (2%) did not have vaccination card. The study found that out of 376 participants, 259 (69%) had good knowledge about the timeliness of vaccination, while 117 (31%) had poor knowledge. Additionally, 241 (64%) of the participants had a positive attitude toward the timeliness of vaccination, while 135 (36%) had a negative attitude. The majority (60.6%) of children were in the 0 to 8 months age group, followed by the 9 to 16 months age group with 24.2% (Table 3).
Obstetric Characteristics of the Study in Wolaiata Zone Public Hospitals, 2024 (n = 376).

Abbreviation: VT, vaccine timeliness.
Vaccination Timelines by Card Plus Maternal Recall
Combining vaccination timing reminder cards and parent-recorded evidence, 128 (83.1%) were vaccinated on time and 26 (16.6%) were vaccinated early at birth. Regarding the 6-week schedule, 57 (72.2%) were vaccinated on time within the recommended period and 17 (24.5%) were vaccinated late. About 45 (72.5%) were vaccinated on time after 10 weeks and 7 (11.3%) were vaccinated early after 10 weeks. 26 (49.1%) received the vaccine on time at week 14 and 19 (35.8%) received the vaccine late at week 14. Nine (52.9%) was vaccinated as scheduled at 9 months, while 6(35.3%) was vaccinated late after 9 months. Four (36.4%) took 15 months, while 45.4% received early vaccination after 15 months. A total of 269 (71.5%) were vaccinated on time and 107 (28.5%) were vaccinated untimely. Of the total 107 children who were not vaccinated at the recommended interval, 9.1% and 19.4% were vaccinated earlier and later than the recommended schedule, respectively (Table 4).
Vaccination Timelines by Card Plus Maternal Recall in Wolaita Zone Public Hospitals, 2024 (n = 376).

Reasons for Vaccination Untimely
Among the reasons given to justify untimely vaccination, the majority of respondents 43 (40.2%) said they forgot the vaccination schedule, 35 (32.7%) lacked awareness about importance of vaccination, 19 (17.8%) said they had lost their child’s vaccination records and were concerned about poor reception from medical professionals, 10 (9.3%) said they fear their children will get sick (Figure 2).

Reasons for vaccination failure among partially vaccinated children.
Factors Associated With Vaccination Timeliness
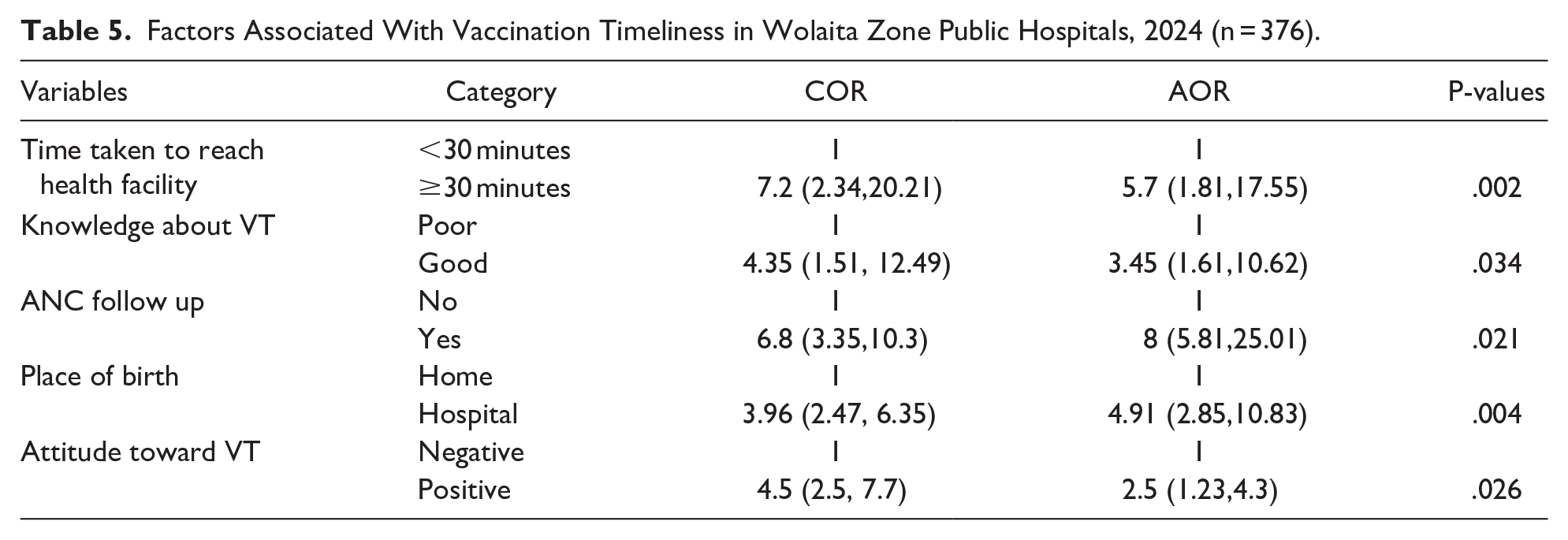
Time to health facility, antenatal care follow-up, place of delivery, knowledge about vaccination timeliness, and attitudes toward vaccination timeliness remained significantly associated with timely vaccination in multivariable logistic regression. Compared with those who took less than 30 minutes, the odds of timely vaccination were nearly 6 times [AOR = 5.7; 95% CI (1.81, 17.55)] was higher in women who took more than 30 minutes to get to the health facility. In addition, the rate of vaccination for children according to the recommended schedule is 3.45 times [AOR = 3.45; 95% CI (1.61, 10.62)] was higher in women with good knowledge about timely vaccination compared to the opposite group.
The chance of being vaccinated on schedule is 8 times higher [AOR = 8; 95% CI (5.81, 25.01)] in women who attended antenatal care compared with women who did not attend antenatal care. Additionally, the odds of receiving the vaccine at the recommended time were nearly 5 times [AOR = 4.91; 95% CI (2.85, 10.83)] was higher in women giving birth at a health facility than in women giving birth at a home. Furthermore, 4 times more women had a positive attitude toward timely vaccination [AOR = 2.5; 95% CI (1.23, 4.3)] were more likely to vaccinate their children within the recommended time than those with negative attitudes (Table 5).
Factors Associated With Vaccination Timeliness in Wolaita Zone Public Hospitals, 2024 (n = 376).
Discussion
Immunization is one of the most cost-effective interventions to promote child survival, preventing 2 to 3 million child deaths each year from vaccine-preventable diseases. 1 This study evaluated timely vaccination in children aged 0 to 23 months. Thus, 71.5% of children were vaccinated on schedule as recommended. This study is supported by a previous study. 23 However, this result is higher than previous studies conducted in North Shewa Zon (33.7%), 29 Gondar city (31.9%), 22 West Shewa Zone (23.9%). 33 Possible reasons for this difference could be due to differences in study period, geographic location, methodology, quality of EPI services, and caregivers’ attitudes and knowledge toward with timely vaccination. The present study is lower than the study conducted in Ghana by 87.5%, 19 94% in Israrel, 20 82% in Philadelphia, 21 and 87% in Uganda. 24 Study participants, geographical location, methodological differences, socio-demographic characteristics of participants, policies and strategies, women’s perceptions, EPI infrastructure and quality Services may be the cause of the difference.
Time from home to health facility, previous antenatal visit, and place of birth, knowledge and attitude about timely vaccination were identified as relevant factors influencing timely vaccination. Women who visited a health facility in less than 30 minutes were 5.7 times more likely to have their children vaccinated within the recommended time than the opposite group. This suggests that time spent vaccinating imposes high opportunity costs on caregivers by creating the need for multiple visits. To improve access to timely vaccination, it is best to expand the vaccination program through health promotion programs in community services. This is consistent with other studies.33,34
Having good knowledge about timely vaccination increases the chances of vaccinating your child according to the recommended schedule. This study is consistent with previous studies.26,35 The explanation may be that knowledge reduces the likelihood of negative feelings about timely childhood vaccination, thereby reducing its use and timeliness. At the same time, knowing the appropriate vaccination time, vaccine-preventable diseases, and reasons for vaccination will increase the chance of timely vaccination. 33 This implies that adequate maternal knowledge is necessary to vaccinate children on schedule and requires special attention.
According to this study, women with a history of prenatal care are more likely to have their children vaccinated on time. During prenatal care follow-up, caregivers will be fully informed about the child’s vaccinations, which can increase their knowledge about timely vaccinations and how to use them. A study from Ethiopia confirmed and found that use of prenatal care increased timely vaccination. 22 In this study, delivery at a health facility was statistically associated with timeliness of vaccination. The results of this study are consistent with other studies,33,36 which indicate that if the mother gives birth at a health facility, timely initiation of vaccination at the recommended intervals will be increased. Therefore, mothers who give birth at health facilities are more informed about the benefits and risks of timely vaccination and health education. Additionally, women who give birth at home may face misconceptions and cultural practices related to childhood disease prevention other than vaccination.
Finally, attitudes toward timely vaccination were significantly related to timeliness of vaccination. This may be related to how women or caregivers feel about it. Having a positive attitude enhances maternal health care-seeking behavior at the facility.
Regarding reasons for not being vaccinated at the recommended time, 40% of women reported that their children were not vaccinated at the time because they forgot the date of vaccination. This study supported by previous studies, 37 indicates that the main reason for mothers not attending the vaccine schedule in time was forgetfulness. It is the fact that if mothers forget the exact date of vaccination, their children are at risk of not being vaccinated on time. Therefore, health care providers should strictly follow or remind mothers to vaccinate their children at the recommended time.
The limitations of the study included the inability to establish causal relationships between outcomes and variables, excluding immune compressed children, and recalling bias. These could affect generalizability of the study. Future research should explore women’s perceptions, health provider and stakeholder opinions, and contextual factors influencing on-time vaccination. Additionally, separating analyses for children who seek vaccines early or late should be considered in future studies.
Policy Implication
This study emphasizes the importance of timely vaccination in Ethiopia and provides data for stakeholders in the child health care system. It suggests strategies such as community health education and mobile technologies to address factors contributing to maternal forgetfulness and improve vaccination timeliness.
Conclusion
This study found that 71.5% of caregivers had vaccinated their children at the nationally recommended vaccination times. The study also identified time from home to health facility, previous antenatal check-up, and place of birth, knowledge and attitude about timely vaccination were factors affecting timely vaccination. By collaborating with non-governmental organization, stakeholders should work together to overcome barriers and challenges that hinder timely vaccination. Finally, policy maker and health care providers should strengthen the call for interventions that target knowledge improvement, attitude change, and healthcare access, especially in remote areas.
Footnotes
Acknowledgements
We would like to express our appreciation to Wolaita Sodo University for continued support and follow-up. We acknowledge the study participants and health care providers for their commitment and cooperation.
Author Contributions
TG: Conceived data and designed the study, supervised the data collection, performed the analysis and interpretation of data, drafted the manuscript, and finally approved the revision for publication. TG had full access to all the data in the study and takes responsibility for the integrity of data and the accuracy of data analysis. EE, BA, and TG assisted in designing the study and data interpretation, and critically reviewed the manuscript. All authors read and approved the final manuscript.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are not publicly available to prevent any kinds of misuse by the public before publication but are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Participant Consent
An ethical clearance was obtained from the Institutional review board of Wolaita Sodo University with the reference number of 9/877/2023 and then submitted to the Wolaita Zone Health Office. Then a permission and cooperation letter was obtained from the zonal health office and distributed to each selected Hospital prior to data collection. Written informed consent was obtained from the study participant and data was collected after assuring the confidentiality nature of responses. All methods throughout the study were carried out in accordance with relevant guidelines and regulations.
Consent for Publication
Not applicable.