
Abstract
Background. Little is known about autism spectrum disorder (ASD) in Qatar. The lack of consensus in ASD screening has led to differences in the reported prevalence with escalating rates over time. Objective(s). To screen for ASD and to identify associate factors among Qatary children aged 18 to 48 months. Methods. A cross-sectional study included 600 eligible children at 10 Primary Health Care Centers (PHCCs) in Qatar. Identification of ASD was based on the M-CHAT™ criteria. Results. The number of ASD screen-positive children in the M-CHAT™ was 25.13 per 10.000, and was significantly associated with older maternal age (10.5%) and history of neonatal hyperbilirubinemia (20.0%) [AOR] = 4.88; 95%[CI]: 1.50-16.30)]. The Odds of detecting ASD was lower in children below 2 years of age (AOR = 0.92; 95% CI: 0.87-0.98]). Conclusion. This study demonstrates the utility of M-CHAT™ for ASD screening in PHCCs. Identification of the factors associated with positive ASD screening can highlight areas suitable for future intervention.
Introduction
Autism Spectrum Disorder (ASD) is a neurodevelopmental disability that is characterized by persistent deficits in social communication and social interaction, along with restricted, repetitive patterns of behavior, interests, or activities.1-3 The causes of ASD are not clear-cut but evidence suggests that several environmental and genetic factors are linked with ASD.4-8
The prevalence of ASD appears to be increasing globally and it has been reported to occur in all racial, ethnic, and socioeconomic groups. In 2022, one in every 100 children was diagnosed with ASD. 9 Previous studies in some Arab countries have shown a prevalence ranging from 1.4 to 29 per 10,000 children.10-12
The significant clinical impact and economic burden of ASD worldwide lead to substantial loss of productivity and health across the patients’ lifespan. Therefore, early diagnosis, therapeutic interventions, and support can potentially improve the outcomes of ASD.13,14
Qatar launched a National Mental Health Strategy in December 2013 as a comprehensive response to address the mental health needs of the population. All babies that visit the Well-Baby clinic (WBC) at the Primary Health Care Centers (PHCCs) are screened at 18 months for hearing loss, delayed speech, ASD, and attention deficit hyperactivity disorder (ADHD). To the best of our knowledge, data on the prevalence and factors associated with ASD in Qatar are scarce. Health-related population-based surveys in Qatar are usually conducted in PHCCs due to their holistic and high standard of care, high utilization of health services, and easy recruitment of representative participants. Alshaban et al conducted a cross-sectional survey from 2015 to 2018 on 176 960 school-aged children in Qatar from national and immigrant families and reported a prevalence of 1.14% (95% confidence interval [CI]: 0.89-1.46) among 6- to 11-year-olds. 15
This study aimed to screen for ASD using a predesigned screening tool and identify the associated factors among Qatari children aged 18 to 48 months attending PHCCs. Determining the epidemiology of ASD in Qatar will provide a foundation for the proper allocation of resources to meet the needs of the affected children.
Methods
Study Design, Setting, and Population
This cross-sectional study was conducted between December 1, 2017, and August 31, 2018, at 10 PHCCs in the State of Qatar. These PHCCs cover a wide area of geographical diversity; they are the popular and first level of contact between individuals in the community and the healthcare system, where comprehensive PHC programs and services are provided to the populace. Each PHCC has a well-defined catchment area and serves a large population from different cultural, social, economic, and educational backgrounds, which offers a good representation of the whole community. Services provided in these centers are free of charge for the entire registered pediatric population, both nationals and expats.
The target population comprised Qatari children aged 18 to 48 months attending PHCCs. No specific exclusion criteria were applied.
A probability 2-stage sampling technique with proportionate allocation of participants was employed to enroll mothers of Qatari children aged 18 to 48 months attending PHCCs. Only mothers were included because the overwhelming majority of caretakers of children in Arab countries are mothers. A list of all PHCCs in the State of Qatar was obtained from the Operations Department in the Primary Health Care Corporation (23 centers, all of which provide WBC services), together with the total number of children aged 18 to 48 months registered in each of these centers. Data were readily accessible and complete due to the presence of a good electronic registration system in PHCCs. The top 10 centers were specifically selected as they serve the highest number of registered children. The total number of children aged 18 to 48 months registered in the selected centers (23 106 children) was used as the total number of eligible children, and it constituted around 83.1% of all children in the same age group in all of the 23 PHCCs. It was used for the proportionate allocation of the calculated sample size in relation to the corresponding percentage of the registered children in each center.
The sample size was calculated to obtain a sufficiently precise estimate of the study sample, and hence, the study power. As there is a lack of information on the local prevalence of ASD in Qatar, we used the latest known population-based prevalence of ASD in a regional Arab country (Lebanon) 12 for the calculation, taking into consideration that they used the same tool with no follow-up diagnosis and prior to positive predictive value (PPV) adjustment. The level of confidence used was 95% and the acceptable error rate was 5%. The following formula was utilized:

Where:
N: Target population (27,805 Qatari children aged 18-48 months registered in all PHCCs at the start of the study period).
n: Sample population (minimum number for the required sample size).
P: Probability or prevalence of ASD in a comparable population (children in a similar age group recruited in the Lebanon study: 26% = [.26]).
d: Acceptable error rate or absolute precision on either side of the proportion: 5% = (0.05)
Z: Statistic for an error of 0.05 corresponding to a 95% confidence level = (1.96).
DEFF: design effect of 2
By adding (DEFF) design effect of 2, the estimated sample size based on this calculation was 592, which was equal to 600 participants after rounding.
In each of the selected 10 centers, daily appointments of the eligible participants were used as a sampling frame, where random selection was deployed to select participants for the day, giving all of them an equal opportunity to participate. Enrollment of eligible participants was continued until the required sample size was reached. The daily appointments were an output of the Electronic Health Record (HER) system used in the PHCCs and caller Cerner®.
Study Tools
The Arabic version of the “M-CHAT™” screening tool was used, alongside a structured-interview administered-questionnaire for the possible associated factors and knowledge sections. The M-CHAT™ is a modification of the “CHAT” (Checklist for Autism in Toddlers). It comprises 23 yes/no questions which are answered by the mothers of the children aged 16 to 48 months. The latest recommended scoring system of the M-CHAT™ suggests that a child is considered at risk for ASD if he/she fails 3 responses or more, regardless of whether the items/questions are critical or not (compared to the older version).
The M-CHAT™ was developed originally in English, 17 but is now available in many languages (Arabic, Chinese, Czech, Dutch, and others). The Arabic version was validated in a study of participants (aged 18-124 months) from 9 Arab countries and published in 2008. The Arabic M-CHAT™ has a sensitivity of 0.86, specificity of 0.80, and PPV of 0.88. 18 Permission to use the M-CHAT tool 17 or its validated Arabic form was obtained from the corresponding author of the aforementioned study. 18
A structured questionnaire was developed in this study (Supplemental File S1). The content and face validity of the questionnaire were established through an extensive literature review and consultation with experts in the fields of community medicine and pediatric psychology to ensure its validity and reliability. The structured questionnaire included domains like characteristics of the children (eg, birth sequence); factors related to pregnancy and delivery (maternal and neonatal complications); and socio-demographic characteristics of the parents (eg, education level, occupation). The questionnaire was originally prepared in English and translated into Arabic language with back translation at an HMC-accredited translation center.
During the process of data collection, the structured questionnaire was administered to the participating mothers first, followed by the M-CHAT™. This sequence aimed to avoid the provision of leading answers, since the questionnaire included questions suggestive of ASD-related features. The final prevalence estimate was obtained by multiplying the results of the positive M-CHAT™ by its PPV of 0.058. 17 Details on the study variables and quality control of the data collection are listed in Supplemental File S2.
Pilot Testing of the Questionnaire
Prior to data collection, a pilot study was conducted in a convenient sample of 20 participants from one randomly selected health center (Al-Wakrah PHCC) to pre-test for any difficulty and/or any inappropriateness of the tool, as well as to measure the time needed to complete each questionnaire, taking into consideration the accompanying logistics to maintain the privacy and anonymity of the interviewees.
Necessary adjustments in the questionnaire and study procedures were made based on the results of this pre-test. The average time required for each participant to complete the questionnaire was about 10 minutes. These 20 participants were later omitted from the study database.
Statistical Analysis
The collected data were revised and fed into the computer software. The database was constructed using the Statistical Package for Social Sciences SPSS™ software version 22. After completion of data collection, data were summarized using frequency distribution tables, percentages, and proportions. Appropriate bar graphs and pie charts were used as required. Mathematical summarization using the mean and standard deviation (SD) was used, whenever appropriate, for quantitative data. Possible associations between categorical variables were statistically assessed using the Chi-Square (χ2) test. Statistical significance was set at P-value ≤ .05. Qualitative data were summarized in a table using commonly shared themes. A stepwise multivariate logistic regression (Backward Wald) model was built using M-CHAT™ categories as the independent variable and variables that showed a significant association (P < .05) in univariate analysis (child age, mother’s age, mother’s age at delivery, neonatal hyperbilirubinemia) as the dependant variables. Only variables with P < .05 were included in the final model.
Results
Sociodemographic Characteristics of the Study Population
A total of 600 mothers of Qatari children aged 18 to 48 months who attended the selected PHCCs and agreed to participate were included in the study. The proportionately allocated frequency distribution in the attained PHCCs is shown in Supplemental Table S1. There were more girls (52.0%) among the participating children with a mean (±SD) age of 29.6 ± 9 months. The enrolled mothers’ age ranged between 18 and 45 years (mean ± SD = 31.3 ± 5.7 years). Most of the mothers (92.2%) had 2 or more children and the birth order of the participating child was second or more (72.2%). A significant proportion of the current marriages of the participating mothers were consanguineous (46.3%), and 5.6% of the participating mothers reported a family history of known major psychiatric illnesses, including depression, bipolar disorders, and schizophrenia. Other sociodemographic factors are detailed in Table 1.
Socio-Demographic Characteristics of Study Participants, PHCCs, Qatar, 2018.

Note. P < .05 is significant.
P value based on Chi-Square test.
PHCCs: Primary Health Care Centers; SD: standard deviation; QR: Qatari Riyals.
Risk of ASD Among the Enrolled Children
The use of the M-CHAT screening tool for the detection of ASD among the enrolled children revealed that 26 out of 600 (4.3%) children had positive disease features (at-risk response; Supplemental Table S2). After adjustment using the PPV of the implemented tool, which was 0.058, the final calculated number of children at risk among the studied sample was 0.2513% (~25 per 10,000 or approximately one child per 398).
Factors Associated With ASD
Positive M-CHAT results suggest that ASD was more frequent among participants in the age group of 18 to 23 months compared to the older age groups (P < .01). Children of mothers aged more than 40 years showed almost 3 times more common M-CHAT positive results compared to the children of mothers in the age group of 20 to 40 years (10.5% vs 3.9%; P < .01), and the same was true for parental age over 40 years at the time of delivery. No association was seen between positive M-CHAT results and the child’s sex, number of mother’s children, child’s birth order, parent’s educational level, the household monthly income category, consanguinity, or familial history of psychiatric illness (P > .05; Table 1).
Childbirth history (low birth weight [<2500 g], being a twin, children born in summer, history of breech presentation, fetal distress, birth injury, meconium aspiration, and feeding difficulty after delivery) was not associated with higher M-CHAT scores although positive M-CHAT results were significantly higher among children with a history of neonatal hyperbilirubinemia (20.0 vs 3.8%, P < .01). Likewise, children with congenital malformation and umbilical cord complications were more likely to have positive M-CHAT results compared to those without the above conditions (16.7 vs 4.2% and 20.0 vs 4.2%, respectively; P > .05), although the difference was not statistically significant (Table 2).
M-CHAT Results in Relation to Participants’ Childbirth History, PHCCs, Qatar, 2018. (n = 600).
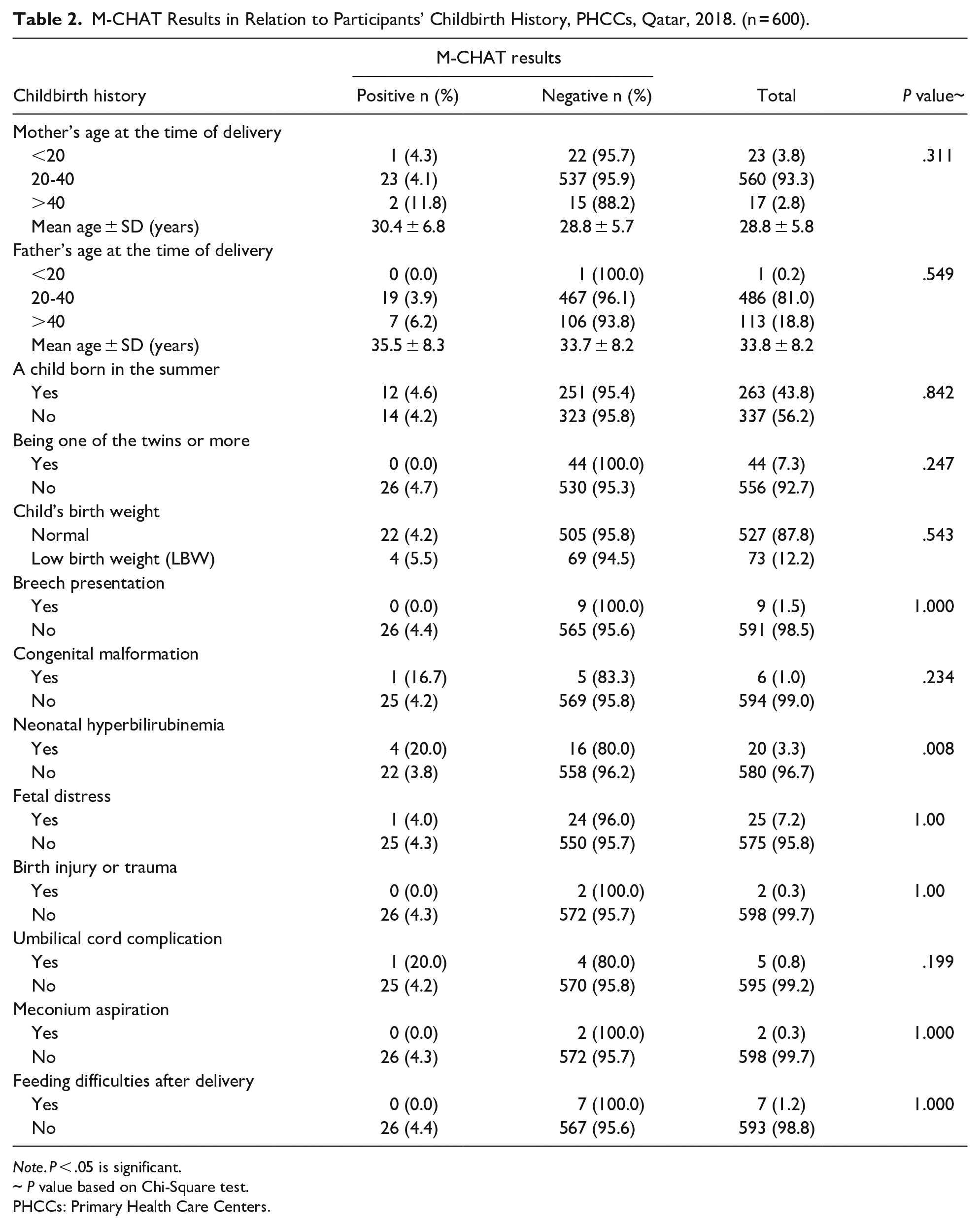
Note. P < .05 is significant.
P value based on Chi-Square test.
PHCCs: Primary Health Care Centers.
Regarding the perinatal history, it was observed that higher M-CHAT scores were attained by mothers who reported receiving therapeutic regimens during pregnancy (8.3 vs 3.9%), mothers with a history of maternal complication (6.7 vs 4.3%), or delivery-related hemorrhage (9.1 vs 4.2%), although the difference was not statistically significant (P > .05; Table 3).
M-CHAT Results in Relation to Participants’ Perinatal History, PHCCs, Qatar, 2018.

Note. P < .05 is significant.
P value based on Chi-Square test.
PHCCs: Primary Health Care Centers.
In stepwise multivariate logistic regression analysis, neonatal hyperbilirubinemia was found to increase the risk of having ASD in the screened children by 5-fold (adjusted odds ratio [AOR]= 4.88; 95% CI: 1.50-16.30). The odds of identifying ASD were lower in children below 2 years of age (AOR = 0.92; 95% CI: 0.87-0.98; Table 4).
A Stepwise Multivariate Logistic Regression (Backward Wald) Model of Factors Associates With Positive M-CHAT™ Scoring, PHCCs, Qatar, 2018.
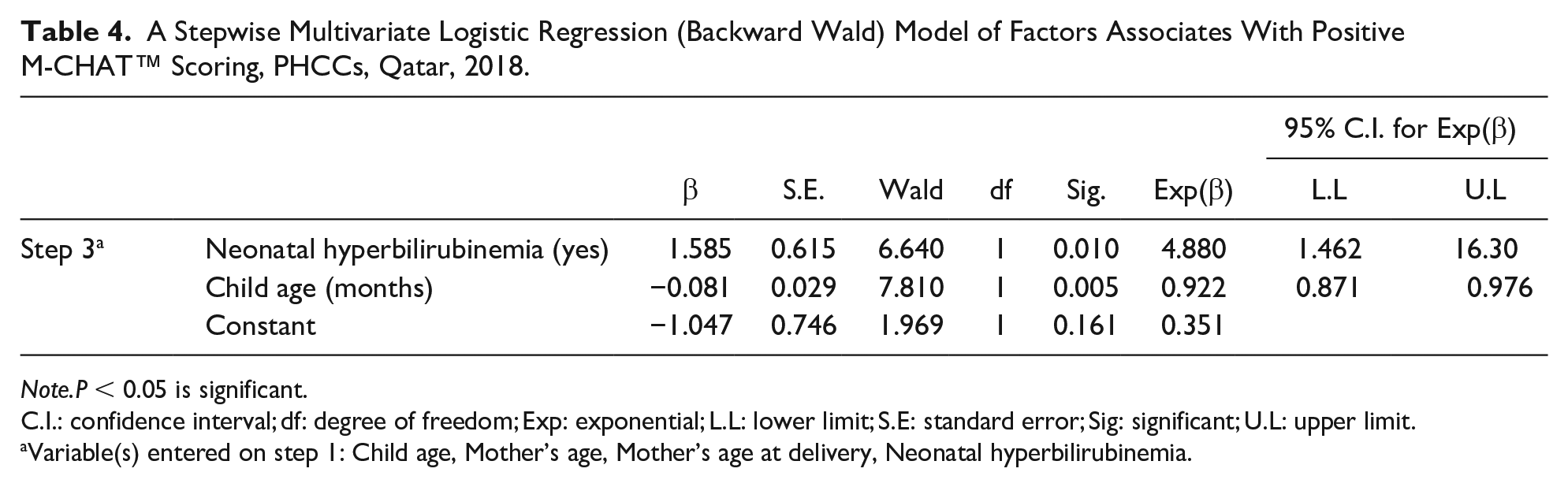
Note.P < 0.05 is significant.
C.I.: confidence interval; df: degree of freedom; Exp: exponential; L.L: lower limit; S.E: standard error; Sig: significant; U.L: upper limit.
Variable(s) entered on step 1: Child age, Mother’s age, Mother’s age at delivery, Neonatal hyperbilirubinemia.
Discussion
The current cross-sectional study is an endeavor to explore the prevalence of ASD in the State of Qatar among children aged 18 to 48 months and the associated factors. The study included 10 PHCCs with the highest number of registered Qatari children in the target age group. They were allocated proportionally to enhance sampling probability. M-CHAT was the tool used for disease screening and 26 out of the calculated sample of 600 reported positive results. After applying PPV of the tool (0.058), the resultant prevalence was 25.13 per 10.000 or 1 case per 398 children. The prevalence in the current study is higher than the published figures from some Arab nations. The difference could be attributed to differences in the sample size, target age group, study design, or the screening tool used (Table 5).
Studies Reporting the Prevalence of Autism Spectrum Disorder.
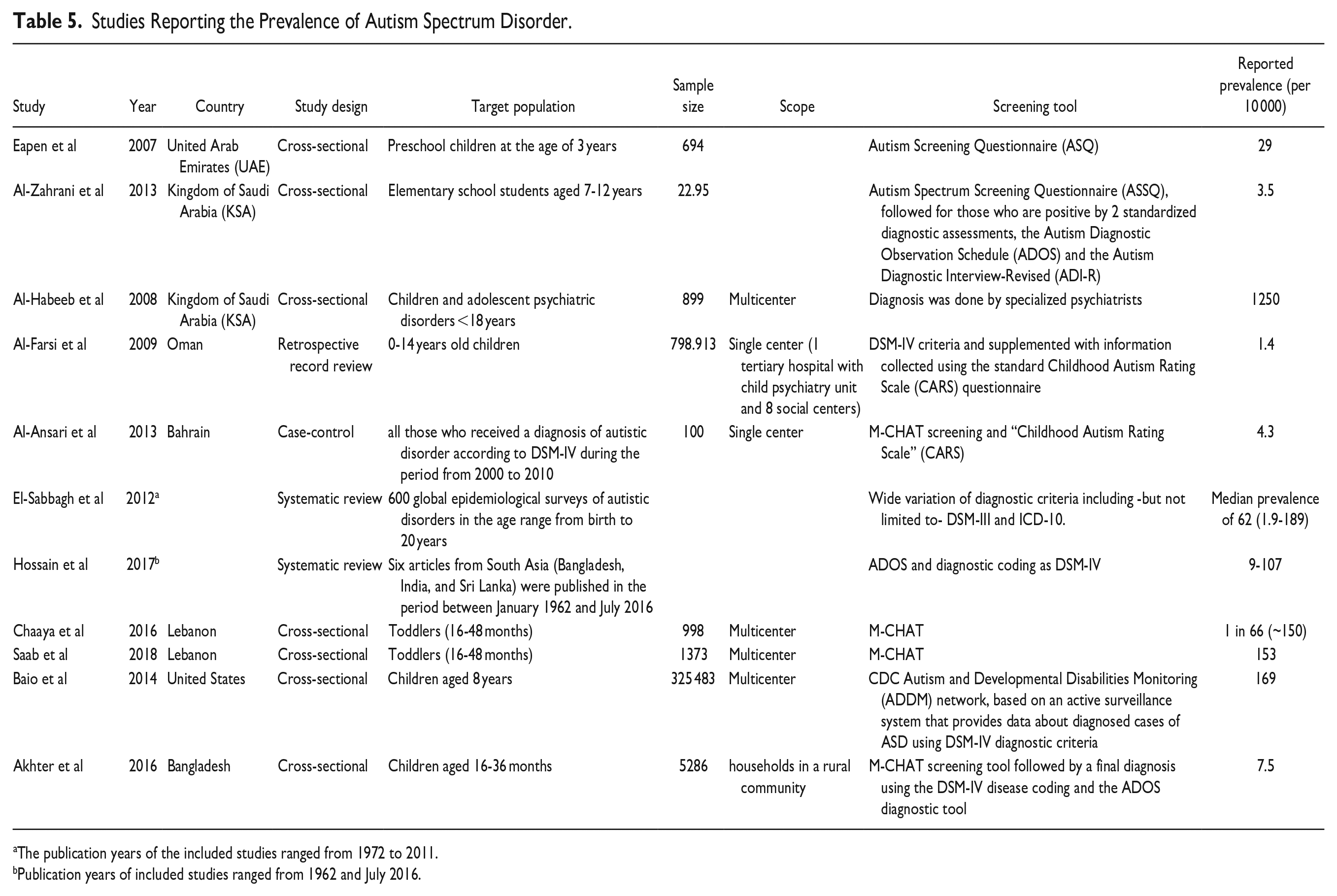
The publication years of the included studies ranged from 1972 to 2011.
Publication years of included studies ranged from 1962 and July 2016.
The determinants of ASD included socio-demographic characteristics, consanguinity, family history of major psychiatric diseases, childbirth history, and perinatal history. One of the most consistent findings in ASD research is a higher rate of ASD diagnosis in males compared to females, which was not in accordance with our results. The frequently stated 4:1 ratio is based on an average from multiple studies worldwide.12,19-24 However, the reasons for this disparity are not yet clear. The stated difference in prevalence between males and females may be due to diagnostic/ascertainment differences. Boys and girls without cognitive impairment may present autism symptoms differently. 25 Girls may score higher because of their better social skills while they still have ASD, which is not detected by the screening or diagnostic tools. Thus, the ratio may be inflated due to biological and sociological sex differences not specific to ASD since inherent sex differences between males and females without ASD are not considered as the baseline to draw comparisons. Likewise, the detection rate of ASD was lower in younger children because the social and behavioral skills can be evaluated better in older children, and some developmental delays may not be detected by parents at an early age (below 2 years) as the parents may consider them as normal variations. Therefore, the influence of age as well as the biological sex on ASD symptomatology should be considered.
ASD is a complex disorder resulting from a combination of genetic and environmental factors. Thus, prenatal exposure could be related to ASD. Children with low birth weight (<2500 g) showed positive M-CHAT results more frequently in the present study, although this did not reach statistical significance. This is in line with the data from a case-control study in Finland, where the calculated AOR of childhood autism among the very low (<1500 g) and moderately low birth weight (<2500 g) children were 3.05 (95% CI: 1.4-6.5) and 1.57 (95% CI: 1.1-2.3), respectively. 26
Being the first child in the birth order has been reported as a possible risk factor for the development of ASD compared to children who are third in order or more, 27 which is contrary to the results of the present study where no association was found between the birth order and positive M-CHAT screening results.
The likelihood of positive M-CHAT results in the current study was higher among children with congenital malformations, which is in agreement with the findings of Timonen-Soivio et al, who reported that congenital anomalies occurred more frequently among children with ASD, suggesting the role of early risk factors during fetal neurodevelopment. 28
Being born to mothers aged more than 40 years at the time of delivery was a significant risk factor for M-CHAT positivity. This finding was similar to the results of a study conducted in the United States by King et al 29 that linked birth records of 4.906.926 children to autism diagnostic records between 1992 and 2000 to calculate the risk of ASD diagnosis associated with maternal and paternal age. The risks associated with maternal age over 40 years ranged from as high as 1.84 (95% CI: 1.37-2.47) to as low as 1.27 (95% CI: 0.95-1.69) according to the birth cohort category.
Unbound unconjugated bilirubin may cause neurotoxicity in preterm babies and thus predispose them to ASD.23,30 In the present study, children with a history of neonatal hyperbilirubinemia attained higher M-CHAT scores, which was found to be a predictor of ASD in our logistic regression model. This was consistent with the results of a meta-analysis where jaundice was strongly associated with ASD. 30
Consanguineous marriage has been consistently linked to high rates of congenital malformations and is widely practiced in several global communities, including in Arab populations where it has been a long tradition. 31 In a large case-control study conducted in India, consanguinity was associated with 3-fold increased risk of ASD in the offspring. 32 However, the current study and another similar study conducted in Qatar did not show an association between consanguineous marriage and positive M-CHAT screening results. 15
A family history of psychiatric illness is not uncommon in children with positive M-CHAT results. In a case-control study in Finland, where having ASD was associated with 2 odds of parental psychiatric diagnosis. 33
Several studies have described the relationship between perinatal history and risk of ASD.26,34,35 Our results showed that a history of perinatal intake of medications, maternal complications, and antepartum hemorrhage were associated with positive M-CHAT screening results among the participating children.
Conclusion
In conclusion, the findings of this study may identify the risk of ASD in children that will help in early diagnosis followed by tailored evidence-based intervention. Children born to older mothers and those with a history of hyperbilirubinemia should be closely monitored for the development of ASD. Given the accuracy of M-CHAT scoring, the application of the ASD screening tool in primary healthcare should be further assessed and revised. Further analytical studies are needed to comprehensively assess the risk factors for ASD, which may have preventive implications.
Limitations of the Study
This study has several limitations. First, we did not confirm the diagnosis of ASD in the M-CHAT screen-positive children; consequently, the prevalence estimate was calculated from the PPV of the screening tool. Differences in the applied screening and diagnostic tools for ASD across different studies have limited the ability to make a precise comparison. Moreover, studies on ASD among children aged 18 to 84 months are rare. Therefore, comparison of the prevalence of ASD in the target age group with that in other age groups could not be performed. Second, data collection with regard to some independent variables was based on the recall of past events, which might have introduced foreseeable biases, third, because of the few significant determinants in this study, multiple logistic regression identified few significant factors associated with ASD. Another limitation of this study is that we did not conduct follow-up interviews with the M-CHAT screen-positive children to ascertain the results. This was not possible because this was an anonymized study and we expected that the parents would be more reluctant to participate if their child(ren) and their own identification had to be provided.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241284476 – Supplemental material for Risk of Autism Spectrum Disorder (ASD) Among 18 to 48 Month Old Children: A Multi-Center Study in Qatar
Supplemental material, sj-docx-1-gph-10.1177_2333794X241284476 for Risk of Autism Spectrum Disorder (ASD) Among 18 to 48 Month Old Children: A Multi-Center Study in Qatar by Aisha Abdulraheem Sameea, Ekram Wassim Abd El-Wahab and Sherif Omar Osman in Global Pediatric Health
Supplemental Material
sj-docx-2-gph-10.1177_2333794X241284476 – Supplemental material for Risk of Autism Spectrum Disorder (ASD) Among 18 to 48 Month Old Children: A Multi-Center Study in Qatar
Supplemental material, sj-docx-2-gph-10.1177_2333794X241284476 for Risk of Autism Spectrum Disorder (ASD) Among 18 to 48 Month Old Children: A Multi-Center Study in Qatar by Aisha Abdulraheem Sameea, Ekram Wassim Abd El-Wahab and Sherif Omar Osman in Global Pediatric Health
Footnotes
Acknowledgements
We would like to acknowledge the study participants for agreeing to participate in the study.
Author Contributions
AAS: Recruitment of the study participants, clinical evaluation and follow up, development of the data collection tools, data collection, statistical analysis and interpretation of data, contributed to writing of the manuscript, revised and approved final version of the manuscript.
EWA: Data curation, statistical analysis and interpretation of data, major contribution to writing, revised and approved final version of the manuscript.
SOO: Conceptualization, developed the theoretical framework and study design, took the lead for overall direction and planning, development and validation of the data collection tools, data curation, statistical analysis and interpretation of data, major contribution to writing, revised and approved final version of the manuscript.
Data Availability
All data are fully available without restriction by the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The study was approved by the institutional review board and the Ethics Committee of the Hamad Medical Corporation (HMC) in Doha, Qatar [ref. no. PHC/IEC/17/10/035]. The research was conducted in accordance with the ethical guidelines of Helsinki’s Declaration (2013). Data sheets were coded with numbers to maintain the anonymity and confidentiality of patient’s data.
This article does not contain any studies with animals performed by any of the authors.
Informed Consent
Informed oral consent was obtained from legally authorized representatives of minor subjects prior to study initiation after explaining the aim and concerns of the study. The ethical committee has approved this form of consent.
Consent for Publication
All authors approved the manuscript for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.