
Abstract
Meningocele, a rare subtype of cephalocele, can manifest in various positions and exhibit diverse characteristics. On the other hand, dacryocystocele, also a rare anatomical disorder, typically presents as a cyst located between the nose and the eye. Generally, distinguishing between these 2 lesions is not difficult. The presented case involves a fetus with suspected dacryocystocele, ultimately diagnosed postpartum as meningocele, underscoring the complexities in distinguishing between these conditions. The article details the patient’s prenatal examinations, imaging findings, and the subsequent surgical intervention, highlighting the significance of meticulous diagnosis for effective prenatal management. The case illuminates the potential oversight and misdiagnosis challenges associated with atypical cephaloceles, contributing valuable insights for clinicians involved in prenatal diagnosis and management.
Introduction
Anterior cephaloceles make up around 20% of all cephalocele cases and are categorized into 2 main types based on their location: sincipital and basal defects.1,2 Sincipital cephaloceles are external lesions occurring near the glabella and are further divided into nasofrontal, nasoethmoid, and naso-orbital types.2,3 Basal cephaloceles are internal lesions located within the nose, pharynx, or orbit, and they are classified into spheno-orbital, sphenomaxillary, transethmoidal, sphenethmoidal, and sphenopharyngeal types. 3 Cephaloceles can be also further categorized into 3 types based on the contents of the herniated sac: meningocele, containing only meninges; encephalomeningocele, containing brain and/or meninges; and encephalomeningocystocele, including part of the ventricular system.2,4
Dacryocystocele is a rare anatomical disorder characterized by cystic dilatations of the lacrimal sac and nasolacrimal duct due to obstructions at 2 specific sites in the lacrimal drainage system.3,5 Typically, anatomical obstructions at the Hasner valve or an imperforate membrane in the lower nasolacrimal duct lead to sac and nasolacrimal duct distension, resulting in compression at the common canaliculus-sac junction and functional obstruction at the proximal end of the dacryocystocele.2,5 This condition may manifest externally as dacryocystoceles or internally as internal nasal cysts, with the potential extension into the orbital cavity, causing proptosis. 6
In typical cases, distinguishing between dacryocystoceles and cephalocele is straightforward. However, when cephalocele occurs anteriorly and its content consists only of brain membranes, it can be challenging to make a definitive diagnosis. Certain cases, characterized by overlapping clinical indicators, may require a definitive diagnosis post-surgical excision of the facial cyst. The following case presentation illustrates a meningocele closely mirroring dacryocystoceles.
Case Presentation
A 37-year-old pregnant woman presented for a prenatal examination at 27 weeks and 5 days gestation. Personal and family histories were unremarkable, with no consanguineous marriage or a history of drug use. She had 2 healthy children. Ultrasound revealed an anechoic structure with well-defined borders between the nose and the right eye, measuring 20 mm × 24 mm, with no color flow on Doppler. The communication between the cyst and the intracranial space was unclear. No other abnormalities were noted.
At the 30-week and 2-day examination, the cyst’s characteristics remained unchanged, measuring about 22 mm × 32 mm (Figure 1). A provisional diagnosis of suspected dacryocystocele was made. The cyst showed minimal changes until the patient underwent a cesarean section around 39 weeks of gestation.

The ultrasound images (A-C), Doppler image (D), and 3D images (E and F) at 30 weeks 2 days reveal a cystic structure between the nose and the right eye.
Postpartum, a protruding cystic structure was observed on the right side, causing elevation, and obscuring the right eye (Figure 2). A follow-up appointment 1 month after delivery indicated that the baby’s condition was stable, with no signs of infection or respiratory distress. As the cystic structure remained unchanged, the patient was admitted for further evaluation and treatment.

The postnatal images, in profile view (A) and in a frontal view (B), depict a large cystic structure in the region between the nose and the right eye, obscuring the right eye.
Magnetic resonance imaging (MRI) performed upon admission revealed a cystic structure with a well-defined border, limited clarity, and no contrast enhancement post-injection, raising suspicion of a dacryocystocele or meningocele. There was a bony defect site that was suspicious for the cystic mass communicating with the intracranial cavity and raised suspicion of meningocele (Figure 3).
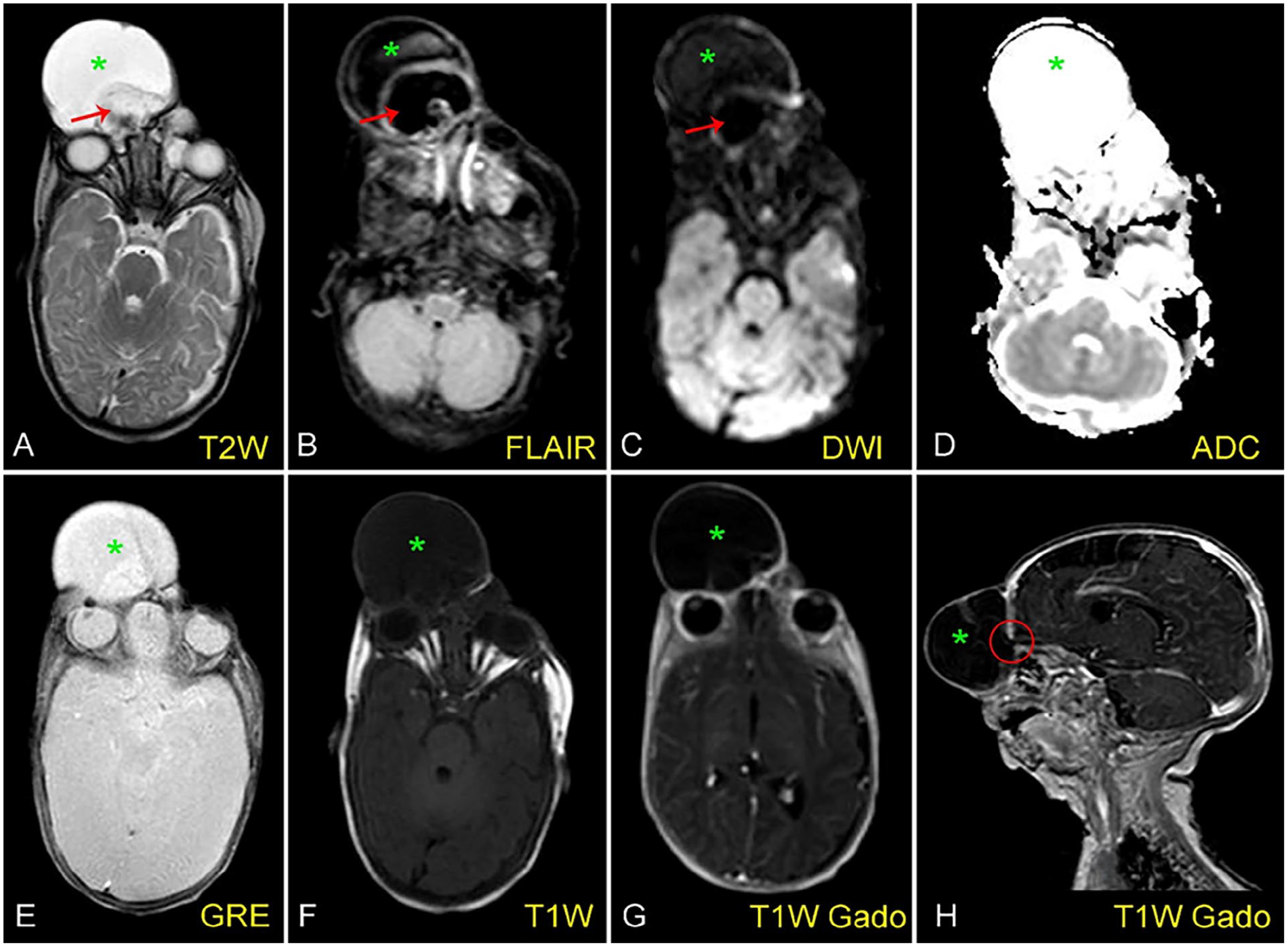
Axial T2W (A), FLAIR (B), DWI (C), ADC (D), T2* (E), T1W (F), T1W Gado (G), and sagittal T1W Gado (H) MR images show a cystic structure (asterisks) occupying most of the patient’s upper face. The signal of the mass content does not match the typical characteristics of pure cerebrospinal fluid and does not resemble brain tissue with noise components (arrows). Sagittal T1W Gado image shows a location that is likely to communicate with the cerebrospinal fluid space (circle).
The patient underwent surgery. The cyst and its attachment near the skull were exposed, revealing a meningocele through a small defect in the frontal bone. Ligation of the hernia and excision of the cyst outside the skull were performed, followed by placement of a prosthetic plate covering the defect (Figure 4). Mild swelling of the face was noted postoperatively (Figure 5A), which gradually resolved, leading to the patient’s discharge 15 days later (Figure 5B). The patient remained healthy during a 3-year follow-up.

The images taken preoperatively (A-C), intraoperatively (D), and immediately postoperatively (E).

The images 5 days post-surgery (A) and 15 days post-surgery (B).
Discussion
Detecting occipital cephaloceles during the second and third trimesters of pregnancy is straightforward and accurate to diagnose this lesion. However, identifying atypically located lesions, such as anterior or parietal cephaloceles, or diagnosing these conditions in the first trimester can pose challenges.2,3,5 Since cephaloceles develop early in fetal development, they are present during the earliest transvaginal sonography. In the late first trimester, specific sonographic features may be observed, including an abnormal fetal profile, discrepancies in biparietal diameter (BPD) and head circumference measurements, and changes in sagittal and coronal sections of the face.1,4 These features can be assessed as early as 9 to 14 weeks of gestation.3,4
In most cases, antenatal diagnosis of dacryocystocele is made through 2-dimensional and 3-dimensional ultrasound with typical appearances showing an enlarged, well-defined, hypoechoic, cystic mass inferomedial to the orbit.1,3,5,7 Possible alternative diagnoses for a periorbital mass in a fetus encompass facial hemangioma, dermoid cyst, anterior encephalocele, and nasal glioma.5,7 Dermoid cysts typically present as hyperechoic masses located superolaterally to the orbit.5,6 Doppler sonography proves helpful in distinguishing dacryocystocele from other congenital malformations, such as hemangioma, by demonstrating the absence of blood flow.
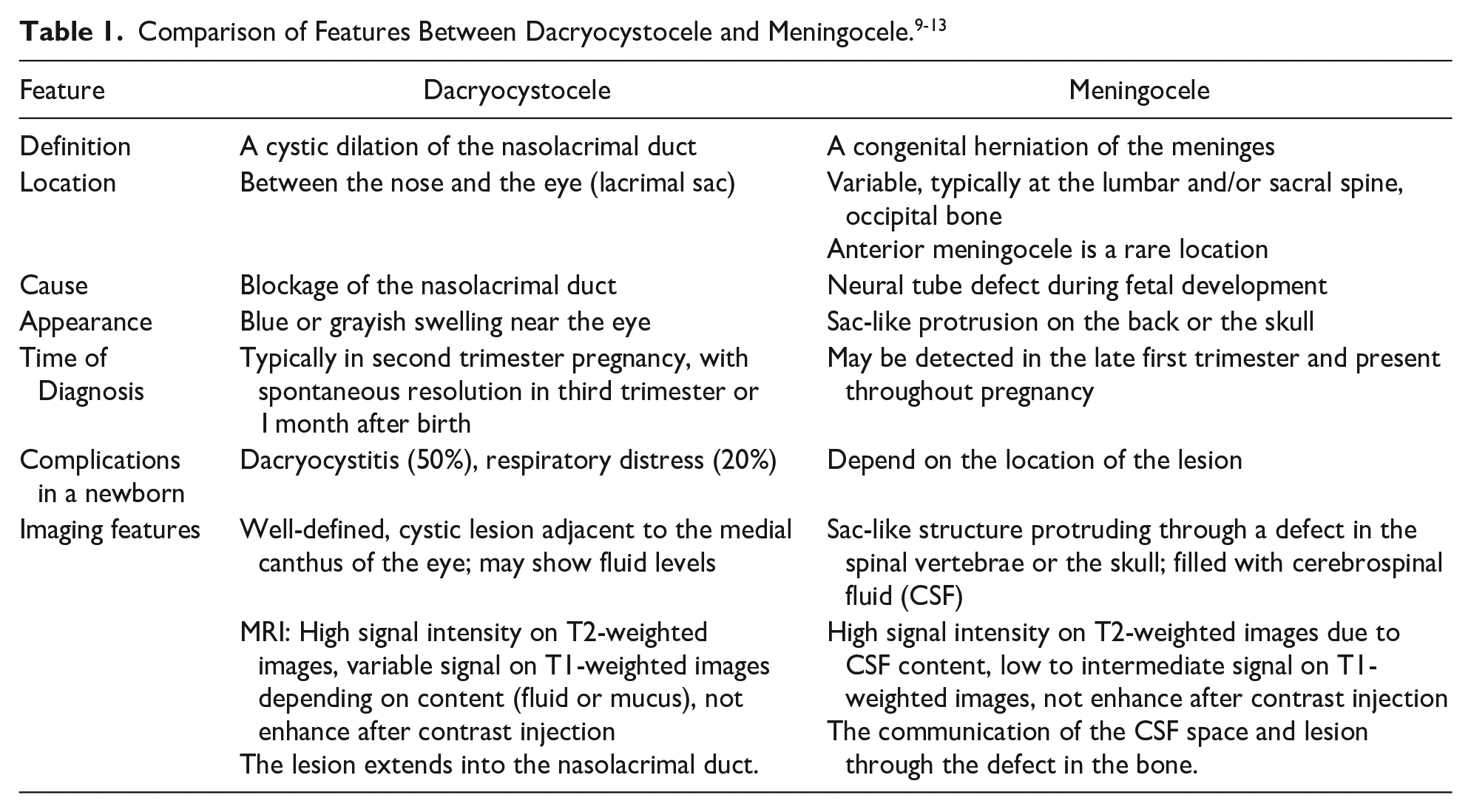
In atypical cases, MRI is employed to differentiate dacryocystocele from conditions such as encephaloceles, nasal gliomas, dermoid cysts, hemangiomas, and choanal atresia.5,7,8 The imaging features of nasal gliomas are distinct, presenting as mass lesions with hypo-to-isodense characteristics, minimal cystic areas, and showing minimal enhancement.2,3,5,7,8 The differential diagnosis between dacryocystocele and meningocele is presented in Table 1.9-13
Spontaneous resolution of dacryocystocele before or at birth is reported in most cases.4,7,8 After delivery, prevalent complications associated with dacryocystocele comprise dacryocystitis (around 50%) and respiratory distress (approximately 20%). 5 The preferred practice pattern across the published literature was an initial trial of conservative management for 2 to 4 weeks, except in cases with respiratory distress at birth.2,3,5,9
In this case, a cyst located between the nose and right eye, lacking color flow on Doppler, raised suspicion of a dacryocystocele. However, a 1-month post-delivery follow-up revealed an unchanged giant cyst, without spontaneous resolution or the common complications associated with dacryocystocele, deviating from its typical course. Furthermore, cephaloceles may present with diverse features and locations. The possibility of a meningocele could not be ruled out, prompting an MRI examination. A well-defined, cystic lesion without enhancing after contrast injection is observed between the nose and the right eye, with suspicion of a connection to the intracranial space. However, the dilated nasolacrimal duct is not clearly visualized. While the presence of brain tissue within the lesion would facilitate diagnosis, it is not visible in this case. Additionally, the cyst shows an inhomogeneous hyperintense signal on T2-weighted imaging, making it challenging to confirm the presence of pure cerebrospinal fluid content. Overall, the MRI findings lean toward a diagnosis of meningocele rather than dacryocystocele. Biopsy is strongly contraindicated due to the risk of infection and meningitis.
Surgical intervention was conducted, and pathological findings subsequently confirmed the diagnosis of meningocele. Over a 3-year follow-up period, the patient remained free of infection, meningitis, and cerebrospinal fluid leaks.
This case highlights the significance of careful diagnosis and consideration of alternative possibilities in preparation for labor plans and surgical interventions. Cephaloceles has been observed in some cases within the nasal cavity, resembling nasal polyps or masses in that area.4,9,10 Typically, cephaloceles involve brain tissue and display a clear skull defect, making a straightforward diagnosis. However, in certain cases, such as the one mentioned above, the herniated mass may appear with benign features, consisting only of meningeal tissue, creating a cystic appearance that provides minimal clues to the presence of meningocele. Therefore, meningeal herniation can exhibit diverse morphologies and may occur in atypical locations, making it prone to oversight and misdiagnosis with other lesions.11,13
Conclusion
This case underscores the importance of careful diagnosis and considering alternative possibilities in labor plans and surgical interventions. While cephaloceles typically involve brain tissue and present with a clear skull defect, there are instances, as mentioned above, where the herniated mass may appear with benign features, resembling a cyst. This variation in presentation, along with the potential occurrence in atypical locations, increases the risk of oversight and misdiagnosis with other lesions. MRI is the best modality to evaluate a meningocele. It confirms the intracranial connection and defines its contents before surgery, thereby enhancing surgical planning and prognosis assessment for the disease.
Footnotes
Acknowledgements
Not applicable.
Author Contributions
All authors contributed equally to this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Ethical Statement
Our institution does not require ethical approval for reporting individual cases or case series. The surgical procedure was conducted in accordance with the principles of the Declaration of Helsinki.
Informed Consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.