
Abstract
Meningocele is a rare congenital malformation of the central nervous system resulting from a herniation of the meninges containing cerebrospinal fluid through a bony defect in the skull. It is part of neural tube closure anomalies. The overall incidence of meningocele is 0.8 to 3 per 10 000 live births; it varies based on geographical location and race, with a predominance of occipital localization. Among diagnostic methods, computed tomography (CT) and magnetic resonance imaging (MRI) remain crucial examinations. Prenatal diagnosis of this malformation primarily relies on ultrasound and screening through maternal serum alpha-fetoprotein (AFP) levels. They typically manifest very early at birth with a highly suggestive radioclinical presentation. Surgical treatment usually allows for a definitive cure. Superinfection and rupture of the meningocele are exceptional, resulting from delayed diagnosis and management. In several developed countries, prevention through genetic counseling and the intake of folic acid during the periconceptional period, along with accurate prenatal diagnosis and the legalization of therapeutic abortion, has led to a decrease in the prevalence of meningoceles. In less developed countries, where there is a delay in diagnosis in exceptional cases, superinfection and rupture may occur. We present the case of an 8-month-old infant with a complicated occipital meningocele with superinfection and rupture.
Introduction
Meningocele is a rare cerebral malformation resulting from a herniation of a portion of the brain and/or meninges due to a congenital anomaly of the cranial bone. 1 It is classified among neural tube closure abnormalities. 2
The incidence of meningocele varies based on geographical location and race, with a global incidence ranging from 0.8 to 3 per 10 000 live births. 3 It accounts for approximately 10% to 20% of all craniospinal dysraphisms. 1
In several developed countries, prevention through genetic counseling and the intake of folic acid during the periconceptional period, along with accurate prenatal diagnosis and the legalization of therapeutic abortion, has led to a decrease in the prevalence of meningoceles. In less developed countries, where there is a delay in diagnosis in exceptional cases, superinfection and rupture may occur.
Case Report
An 8-month-old infant, born from an inadequately monitored pregnancy, within a poor family residing in a rural area, with a first-degree consanguinity. He is the youngest of 7 siblings, all in good health. The mother did not take folic acid during pregnancy and underwent only one prenatal ultrasound at the beginning, which did not detect the meningocele. Since birth, he had a gradually enlarging occipital swelling measuring 2 cm. An MRI was requested to confirm the diagnosis.
Unfortunately, due to the father’s health issues and financial difficulties, there was a delay in seeking medical care. At the age of 6 months, the swelling measured 8 cm (Figure 1). An initial MRI was performed, diagnosing an occipital supratentorial cephalocele of the meningocele type. The MRI revealed an occipital bony defect with a neck measuring 25 × 25 mm, giving rise to a sac of meningeal membranes containing fluid with low signal intensity on T1 and high signal intensity on T2, devoid of brain tissue or ventricles, thus ruling out the diagnosis of meningoencephalocele and meningoencephalocystocele measuring 86 × 77 mm (Figure 2).

Occipital swelling at the age of 6 months.
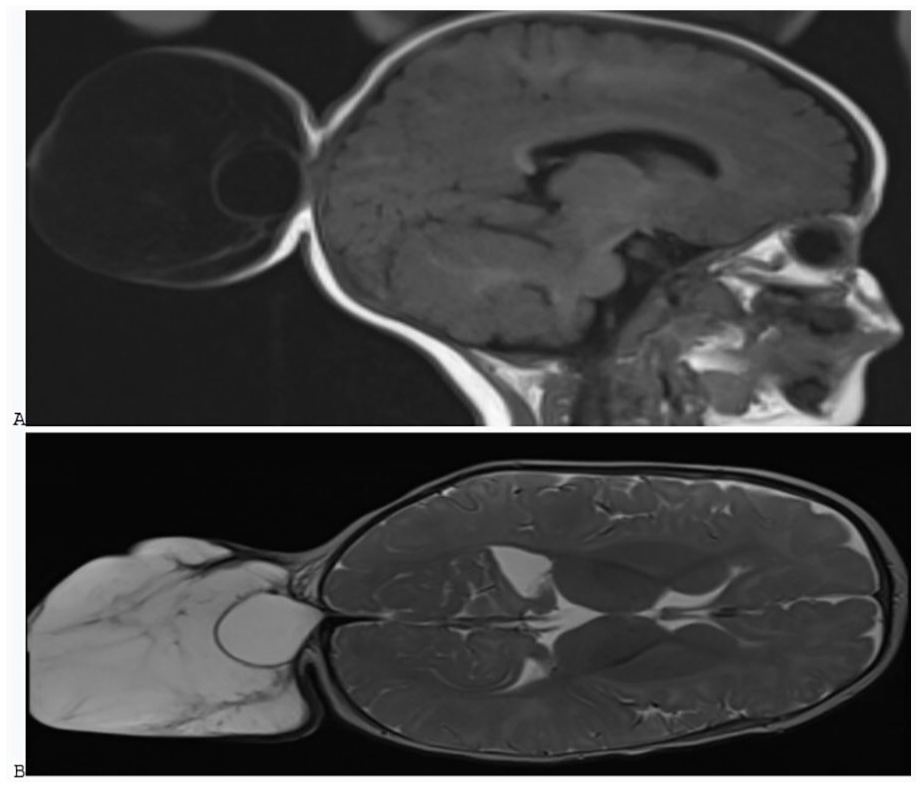
Brain MRI: sagittal section: an occipital bone defect giving birth to a bag of meningeal envelopes containing liquid in hyposignal T1 (A) and hypersignal T2 (B).
A decision for surgical intervention was made, but another 2-month delay, again due to family reasons, led to a change in the clinical appearance of the swelling, which increased in size and exhibited a yellowish fluid (Figure 3). A second MRI revealed an occipital bony defect with a neck measuring 26 × 22 mm, giving rise to a pouch of meningeal membranes containing cerebrospinal fluid without brain tissue or ventricles. A contrast-enhanced portion was noted after contrast injection, indicating thickening of the meninges and vascular structures, suggestive of infectious neo-angiogenesis.

Increase in size of the occipital swelling with the presence of yellowish fluid.
The final diagnosis was a ruptured and infected supratentorial occipital cephalocele of the meningocele type (Figure 4).

Brain MRI: (A) sagittal section T1, (B) Axial section T2: an occipital bone defect giving birth to a bag of meningeal envelopes containing liquid in hyposignal T1 and hypersignal T2, (C) Brain MRI: Sagittal section with injection : Presence of an enhanced portion after injection of PDC related to thickened meninges and vascular structures in favor of infectious neo-angiogenesis.
The infant underwent a successful surgical procedure (Figure 5). Follow-up at 3 and 6 months post-surgery showed highly satisfactory result

The infant after surgery.
Discussion
Meningocele is a rare congenital malformation of the central nervous system resulting from a herniation of the meninges containing cerebrospinal fluid through a bony defect in the skull. It is part of neural tube closure anomalies.
The overall incidence of meningocele is 0.8 to 3 per 10 000 live births; it varies according to geographic location and race, with a predominance of occipital localization.
It must be distinguished from encephalocele, where the herniated sac contains meninges, cerebrospinal fluid, and normal or malformed brain tissue, and from meningoencephalocele, which is characterized by the additional presence of a ventricular horn within the herniated brain tissue.
The etiology of meningocele remains obscure up to the present. Epidemiological studies have led to the suspicion of certain etiologies, especially related to neural tube closure. Factors such as higher frequency among subjects of white race compared to others, consanguinity, 1 malnutrition, particularly folic acid deficiency, 4 and socioeconomic status, 4 which were present in our case, along with factors absent in our case such as heredity, infection, 5 maternal diabetes during pregnancy, 5 alcoholism, and antiepileptic drug use.
Meningoceles can be associated with several malformations, the most common of which are agenesis of the corpus callosum, hydrocephalus, microcephaly, and myelomeningocele, 6 all of which were absent in our case.
Superinfection of meningocele or other cephaloceles is exceptionally rare because treatment is carried out before the occurrence of superinfection. There are hardly any cases in the literature that have reached the stage of superinfected or ruptured meningocele. In many developed countries, prevention through genetic counseling and folic acid supplementation during the periconceptional period, accurate prenatal diagnosis, and the legalization of therapeutic abortion have reduced the prevalence of meningoceles. As a result, superinfection is extremely unusual. Even in certain underdeveloped countries where adequate pregnancy monitoring and prevention measures are lacking in rural areas, its occurrence is very rare, and the development of superinfection is exceptional in cases of delayed intervention.
Screening can be performed through prenatal ultrasound, especially during the third trimester, as this period provides the most detailed morphological information. However, during the 2 semesters preceding the diagnosis, it can also be achieved by observing 2 elements: a defect in the perimeter of the cranial vault and a purely liquid-filled cystic mass (meningocele), or a heterogeneous mass with a varying proportion of brain tissue (encephalocele). 7 Unfortunately, in our case, this screening was not conducted.
CT scan can be performed in a bone window, and it is an essential method for accurately defining the bony contours due to its excellent resolution at this level. It allows for the assessment of the bone structure and visualization of the bony defect. Additionally, a parenchymal window enables the study of the nature of the sac’s contents and the search for malformations.
MRI is the best examination for highlighting cephaloceles and the sometimes associated brain malformations. 8 The main drawbacks of this examination are its relatively long duration for young children and the impressive noise generated by the magnetic field. Therefore, it is necessary to administer pre-medication to children.
In cases of superinfection, MRI will reveal a sac of meningeal envelopes containing cerebrospinal fluid with vascular structures related to infectious angiogenesis.
Differential diagnoses can be easily ruled out, including: cephalhematoma, lipoma, midline dermoid cyst, cystic hygroma, and teratoma. 9
The treatment involves surgical resection, and various surgical techniques are proposed based on the location of the malformation. 10
The operative indication must take into account several elements, namely the patient’s general condition, associated anomalies, and the characteristics of the encephalocele (its size, its contents, its anatomical location).
The goal of treatment is the reintegration of the herniated content and the closure of the meningeal gap. Reintegration can only be performed for small encephaloceles when the herniated brain tissue appears functional and is operated on early enough. On the contrary, the reintegration of large meningoencephaloceles exposes to sudden intracranial hypertension. 11
The closure of the meningeal envelopes must be as watertight as possible, reinforced by an aponeurotic coat overlay, and followed by tension-free skin closure. These are the best assurances of success. Any failure in this area exposes to infectious incidents and fistulas. 12
The vital and functional prognosis of encephaloceles depends on several factors, first and foremost the presence of associated neurological or systemic anomalies, or the presence of hydrocephalus from the outset or microcephaly. It is generally of poor prognosis. 13
Occipital forms have a rather unfavorable prognosis when the malformation is of significant size, or when it contains brain tissue or if microcephaly is present. According to Sanoussi et al, 2 in a series of 161 cases of occipital encephaloceles, the mortality rate at 3 months was 22.36% (36 patients), and the morbidity was close to 80% at 3 months.
A meningomyelocele has a significantly more favorable prognosis than encephalocele. 14
It is very difficult to assess long-term outcomes as there are few observations where the patient is followed for a sufficiently long period. However, a study conducted on 34 cases of anterior meningoencephaloceles with a follow-up of 70 months showed excellent esthetic results in 22 cases, good results in 6 cases, and fair to poor results in 5 cases. 15
In the literature, despite all the advancements, the mortality and morbidity rates remain somewhat high. In the long term, psychomotor development is at stake in cases of encephaloceles. There is no study on a long-term outcome of an infected or ruptured meningocele or other encephalocele.
Conclusion
Superinfection of a meningocele is exceptional and should be avoided by suspecting the diagnosis before birth through prenatal ultrasound or clinically and radiologically after birth, intervening before reaching this stage.
Footnotes
Author Contributions
All authors contributed equally to this work and have read and approved the final version of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
No ethical approval is required for de-identified single case reports based on our institutional policies.
Informed Consent
Written informed consent was obtained from a legally authorized representative.