
Abstract
Objectives. This study aims to determine the prevalence of hemophilia in Thi-Qar, Iraq and study clinical and demographic characteristics of patients with hemophilia. Methods. In this cross-sectional study, data were obtained by reviewing all patient medical records and interviewed with the patients and their parents in 2022. The total number of patients enrolled for this study was 110 children. Results. The prevalence of hemophilia in Thi-Qar was 9.5/100 000 population (18.7/100 000 males). Factor VIII inhibitors were positive in 13.1% of patients with hemophilia A (HA). Target joints were developed among 41.4% and 27.3% of patients with HA and hemophilia B, respectively. Hepatitis C virus was positive in 3% of those with HA. Inhibitors development and arthropathy were more among those with severe disease (22% and 46.3%, respectively). Conclusion. Hemophilia prevalence in Thi-Qar was higher than the total prevalence in Iraq reported by World Federation of Hemophilia in 2022.
Introduction
Hereditary bleeding disorders are a group of multiple diseases that occur due to congenital coagulation factor deficiencies or platelet disorders resulting in abnormalities of primary or secondary hemostasis. 1 Hemophilia and von Willebrand disease are the most prevalent types of hereditary bleeding disorders.
Hemophilia is an X-linked recessive disorder, which may be inherited or arise from spontaneous mutation. 2 The 2 most common forms of hemophilia are Hemophilia A (HA) (factor VIII deficiency), and hemophilia B (HB) (factor IX deficiency). Hemophilia C (Factor XI Deficiency) is a rare type of hemophilia. 3 Based on the level of factor activity, patients with hemophilia may present with easy bruising; post-trauma or post-surgery bleeding or, in the severe cases, spontaneous hemorrhage.3,4 The worldwide incidence of hemophilia A is 1/5000 male births, and that of hemophilia B is 1/30 000.5,6 While, hemophilia C affects 1 in 1 000 000 population. 1
According to the annual report of World Federation of Hemophilia (WFH) in 2022, in 125 countries, 257 146 people with hemophilia were identified, of whom 208 957 had HA, and 42 203 had HB. 7 China ranked first in number of registered patients with hemophilia in 2022, with a total number of 32 638 patients, followed by the India, and United States.7,8 In Iraq, the annual report of World Federation of Hemophilia (WFH) in 2022, identified 3306 patients with hemophilia, 2671 of whom had HA and 635 had HB, with a prevalence of approximately 7.4/100 000 population. 7
Over 90% of the hemorrhagic events involve hemarthrosis that presented in the first years of life and when recurrent results in permanent damage to the joint, arthropathy, chronic pain, and disability. 9
The most important complication in hemophilia treatment is Inhibitor development. It makes treatment with factor concentrates ineffective and causes difficult-to-control bleeding episodes, placing a significant socio-economic burden on the patient. 10 About 30% of patients with severe form of HA and 5% of those with severe HB will develop inhibitors.4,11,12 Inhibitor formation is a multifactorial and results from the interactions between both genetic and environmental factors.5,10 The risk of acquiring transfusion-transmitted infection especially hepatitis C virus (HCV), hepatitis B virus (HBV), and human immunodeficiency virus (HIV) is high among patients with hemophilia because of multiple transfusion of blood, fresh frozen plasma (FFP) and cryoprecipitate that prepared from pool plasma of thousands of donations. 13 The use of recombinant factor concentrates would significantly reduce the infectious complications from replacement therapy. 14
This study aimed to estimate the prevalence of hemophilia in Thi-Qar, Iraq, study the socio- demographic characteristics of the patients, and identify the main complications and treatment regimen used for the patients with hemophilia.
Patients and Methods
Study Design
This cross-sectional analytical study conducted on pediatric patients with hemophilia who have been registered at the center for hereditary blood diseases (CHBD) in Thi-Qar, Iraq.
Data were collected during the period from 4th of June to 30th of July 2022.
Sampling
The total number of patients with hemophilia registered at the CHBD in Thi-Qar was 215 (193 with HA, and 22 with HB), 213 were males and 2 were females, 110 were children (aged ≤ 18 years) and 105 were older than 18 years. One-hundred ten children were recruited in this study. Information was obtained by reviewing all patient medical records at this center and interviewed with the patients and their parents. The total population in Thi-Qar in 2021 was 2 263 695, with total number of males 1 136 218. This data was obtained from Central Statistical Organization. 15
Inclusion criteria
All children aged ≤ 18 years with congenital hemophilia and registered in the CHBD.
Exclusion criteria
All patients older than 18 years and those with acquired hemophilia.
Tools
The questionnaire was extracted from several previous studies.2,3,5,9,12,13
The collected data included:
Sociodemographic characteristics like sex, age, place of residence, parental consanguinity, and family history of hemophilia.
Type and severity of hemophilia: The severity of the disease was classified on the basis of the patients’ factor VIII or IX levels, where mild was >5%, moderate was 1% to 5%, and severe was <1% factor level. 2
First clinical presentations (eg, Hemarthrosis, Epistaxis, skin and subcutaneous bleeding [ecchymosis, bruise, hematoma], gum bleeding, umbilical bleeding).
Complications: presence of inhibitors, arthropathy or target joint, viral infections (hepatitis B virus [HBV], hepatitis C virus [HCV], and human immunodeficiency virus [HIV]).
Target joint defined as a joint in which at least 3 or 4 bleeds have occurred within a 3 to 6-month period. 16
Type of treatment: recombinant factor VIII (rFVIII) or recombinant factor IX (rFIX) concentrates, blood and blood products (FFP and cryoprecipitate), and antifibrinolytic drug for example, tranexamic acid (use for mucosal bleeding as epistaxis and gum bleeding). Treatment for inhibitors (recombinant factor VII concentrate [rFVII], emicizumab [Hemlibra], corticosteroid), and on demand or prophylactic therapy were also recorded. The prophylaxis regimen use in the center is low dose of recombinant factor (20 IU/kg) every 3 days. High dose prophylaxis (100 IU/kg) use in preoperative cases.
Hepatitis B vaccine.
All the patients have investigations for clotting factor assay (factor VIII and factor IX), partial thromboplastin time (PTT), prothrombin time (PT), bleeding time (BT), and blood group. Viral screen for HBV, HCV, and HIV using Enzyme linked immunosorbent assay (ELISA) was done routinely for all patients every 3 months. Failure of a bleeding episode to respond to appropriate therapy is the indication for inhibitors screen in the center. Detection of inhibitors was done by mixing study and Bethesda assay method.2,10,11 Clotting factors assay, mixing study and Bethesda assay were not available in the CHBD in Thi-Qar and have been done in hemophilia center of other governorate or in private laboratories.
Statistical Analysis
Data were entered and analyzed using excel program and the Statistical Packages for Social Sciences (SPSS) version 27. Comparisons of proportions were performed using crosstab module using Chi square test when each cell had an expected frequency of 5 or more, and Fisher’s exact test was used when one or more of cells had an expected frequency of less than 5 in a 2 × 2 table. For all tests, a P value of <.05 was considered statistically significant.
Epidemiological Analysis
The prevalence of hemophilia was calculated by dividing the number of existed cases of hemophilia by the total population at risk. This value is multiplied by standard multiplication factor (in this study was 100 000).
Ethical Approval and Informed Consent
Written informed consent was obtained from legally authorized representatives of all the minor subjects to participate in this study and to publish their data before enrollment in the study. The study was approved by the ethical scientific committee of the Medical college/ University of Thi-Qar, (approval No.7/54/248). A written assent (decision No. 2022086/ Thi-Qar) was obtained from Thi-Qar health directorate and the manager of CHBD to reviewing all patient medical records and interview with the patients and their parents.
Results
The total number of patients with hemophilia registered at the CHBD in Thi-Qar was 215 (193(89.8%) with HA, and 22 (10.2%) with HB), from them 213 (99.1%) were males and 2 (0.9%) were females.
The prevalence of hemophilia in Thi-Qar among all age groups was 9.5/100 000 population (18.7/100 000 males). The prevalence of HA was 8.5/100 000 population (16.9/100 000 males), and for HB was 1/100 000 population (1.8/100 000 males).
A total of 110 children with hemophilia aged ≤ 18 years were included in this study. Ninety-nine (90%) were HA and 11 (10%) were HB.
The majority of patients with hemophilia were males (98.2%). A significantly higher percentage of the patients (67.3%) were live in the periphery of the city, P < .05. About two-thirds of the patients (64.5%) had another family member with hemophilia, while one-third of them (35.5%) had negative family history. This result was statistically significant, P < .05. The parents of more than half of the patients with HA (53.5%) and more than two-third of those with HB (72.7%) were relatives (Table 1).
Socio-Demographic Characters of the Patients According to Type of Hemophilia.

P < .05 emphasized in bold.
Abbreviations: HA, hemophilia A; HB, hemophilia B.
Fisher’s Exact test was used. **Chi-Squared test was used.
The higher percentage of the patients with HA and HB (42.4%, 54.5%, respectively) have moderate form of the disease (Table 2).
Distribution of Patients With HA and HB by Severity of the Disease.
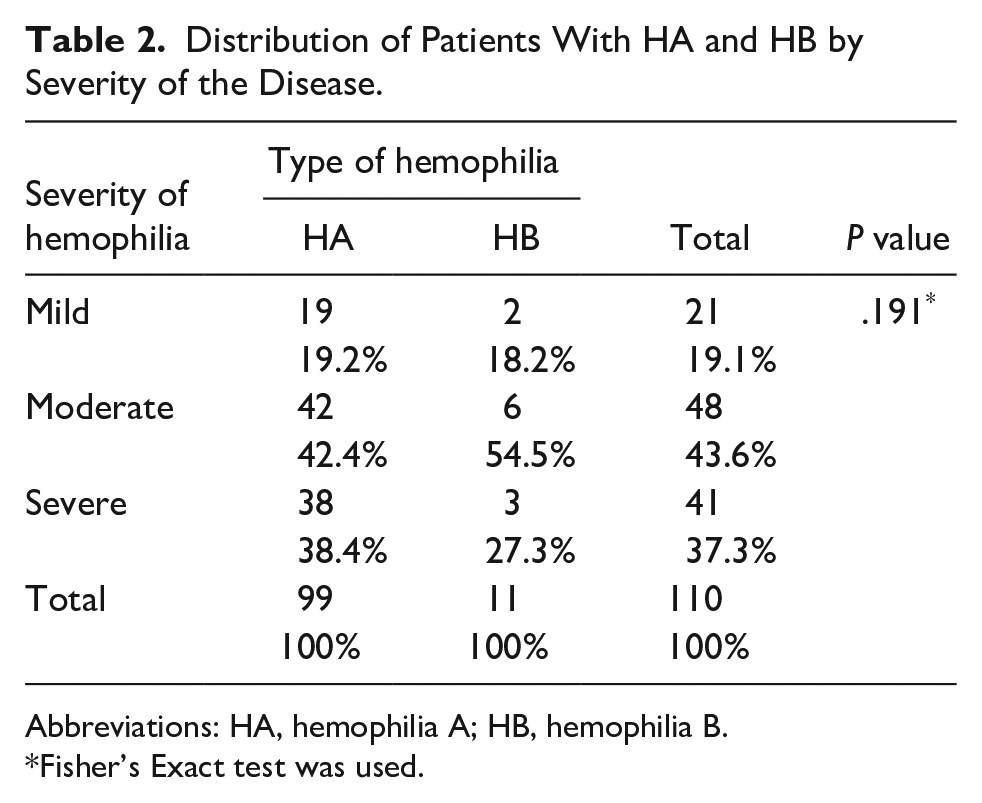
Abbreviations: HA, hemophilia A; HB, hemophilia B.
Fisher’s Exact test was used.
In this study, 13.1% of the patients with HA had inhibitors against factor VIII. Forty-one (41.4%) of the patients with HA and 3 (27.3%) of those with HB were develop target joint. This result was statistically significant, P < .05. Both inhibitors and arthropathy were more reported among children with severe hemophilia (22%, 46.3%, respectively; Table 3).
Distribution of Complications Among Patients According to the Type and Severity of Hemophilia.
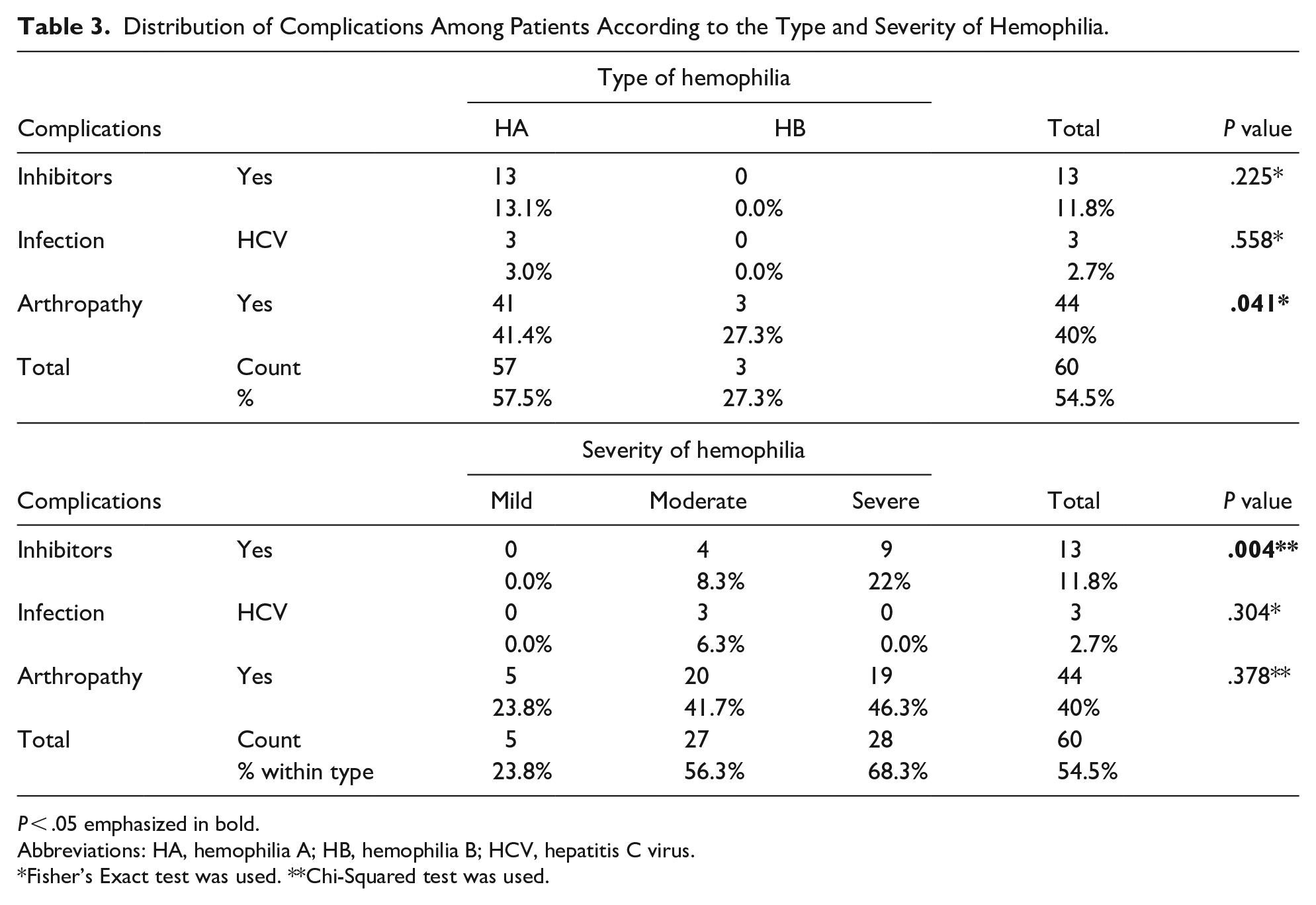
P < .05 emphasized in bold.
Abbreviations: HA, hemophilia A; HB, hemophilia B; HCV, hepatitis C virus.
Fisher’s Exact test was used. **Chi-Squared test was used.
The most common first clinical presentation of patient with HA and HB was skin bleeding (39.4%, and 54.5%, respectively), followed by hemarthrosis (16.2%) in HA and gum bleeding (18.2%) in HB, Fisher’s Exact Test = 13.948, P = .20.
This study founded that 47.5% of the patients with HA and 54.5% of those with HB were on prophylactic therapy. From 13 patients with HA and inhibitors, 7 (53.8%) patients received Hemlibra (emicizumab) drug (Table 4).
Distribution of the Patients With HA and HB by Treatment Regimen and Types of Treatment.

Abbreviations: rFVIII, recombinant factor VIII; rFIX, recombinant factor IX; rFVII, recombinant factor VII.
Chi-Squared test was used.
Discussion
Hemophilia is one of the most common hereditary bleeding disorders and has been recognized in all areas of the world and in all ethnic groups.
This study detected that the prevalence of hemophilia in Thi-Qar, Iraq, was approximately 9.5/100 000 population (18.7/100 000 males) which was higher than the prevalence reported by Kadhim et al in Baghdad in 2016 which was 8.1/100 000 population (15.9/100 000 male), 17 and higher than the total prevalence in Iraq which was 7.4/100 000 population according to the annual report of WFH in 2022. 7
In this study, the prevalence in Thi-Qar was compared with that reported by one study in Baghdad. 17 No recent researches on the hemophilia prevalence in other areas in Iraq which are necessary for more accurate comparison.
The actual prevalence of hemophilia in Thi-Qar may be higher than the reported prevalence in this study.
This underestimation may be related to the lack of screening tests and genetic study for individuals with family history of hemophilia and delayed in diagnosis especially those with mild hemophilia, because the disease may be discovered only after surgical intervention or trauma resulting in prolonged bleeding. Therefore, screening tests for all members with a family history of hemophilia, those with carrier mothers, and those with bleeding symptoms at birth, with accurate registry system and improving the health care resources can help address this challenge. 18
In comparison with the estimated prevalence per 100 000 population in some neighboring countries in 2022, the prevalence in the current study (9.5/100 000 population) was higher than that reported in Saudi Arabia (3.9), Jordan (4.6), Syria (5.3), and Egypt (6.1), while it was lower than that reported in Iran (13.3) and in UK (14). 7 The prevalence of hemophilia is increasing worldwide. This increment may be related to the availability of a well-designed, patient-centered registry system, better diagnostic and treatment facilities, with improving survival.7,18-20 The variation in the reported prevalence among different countries could be due to inaccurate reporting practices, lack of diagnostic tools, poor availability of factor replacement therapy and consequent death of those with severe hemophilia, and difference in access to hemophilia care in countries with low prevalence. 19 Although hemophilia is an X-linked recessive disorder and transmitted through heterozygote female (carriers), homozygosity (two identical hemophilia alleles) in a female most often occurs because of a cousin marriage within a hemophilia family, with the father having hemophilia and the mother a heterozygote by inheritance. As a result, consanguineous marriage may influence hemophilia prevalence through this inheritance pattern.21,22 In fact, consanguineous marriages are common in Iraq and may affect disease prevalence. 23
In this study, HA was more prevalent than HB. This result was in agreement with that of other studies in Iraq, 17 Brazil, 24 and India. 25 More than two-thirds of the patients (67.3%) in the current study were live in the periphery of the city. Similar result was reported by Al-Zubaidy in Al-Ramadi City 26 and Khuntdar et al in Bengal. 27 Being an inherited disorder, about two-thirds of the patients (64.5%) in this study had a positive family history of hemophilia, whereas one-third of them (35.5%) had negative family history that mean result from spontaneous mutation. These results are consistent with the results of other studies.3,27 Parental consanguinity was present in more than half of the patients with HA (53.5%) and more than two-third of those with HB (72.7%), this result was statistically not significant. Similar result reported by other study. 26 More advance researches on the relation of parental consanguinity with the disease prevalence among their offsprings are important. Education, awareness and genetic counseling for parents and those with family history of hemophilia is essential to reduce the spread of these bleeding disorders in the community.
In the current study, the higher percentage of the patients with HA (42.4%) and HB (54.5%) had a moderate type of the disease followed by severe type and the least one was the mild type. In comparison with other Iraqi governorates, Kadhim et al in Baghdad, 17 and Lateef et al in Diyala 28 reported that severe type was the most prevalent one. Similar result was detected by Nigam et al in Bhopal, India. 29 This result may be due to mild cases may go undetected till later years especially those who do not undergone surgery in early life and not registered in the hemophilia center. In addition, many cases with severe hemophilia often die early in life. 19
In the present study, the percentage of FVIII inhibitors among patients with HA was (13.1%), which was higher than that reported for Iraq by WFH in 2022 which was (8.9%). 7 No inhibitors were detected among those with HB in this study. In other Iraqi governorates, Taresh and Hassan, in Basra reported that 18.6% of the patients with HA presented with inhibitors, and none in those with HB. 10 In Baghdad, Albeldawi DH reported that 12.8% of the patients with HA and 9% of those with HB had inhibitors, 30 whereas in Diyala, Lateef reported that the frequency of inhibitors in patients with HA was 5.3%, and none in those with HB. 31 In neighboring countries, Oudat et al reported that the prevalence of FVIII inhibitors was 12% in Jordan, 32 whereas Owaidah et al founded that the rates of inhibitors in patients with HA was (29.3%) in Saudi Arabia. 33 The prevalence of inhibitors varies from country to country, and this variation may relate to several factors including genetic characteristics of the patients, type of product used as treatment, duration and intensity of treatment, or type and sensitivity of the diagnostic test detecting the inhibitors.25,32,33
The prevalence of HCV (2.7%) among patients with hemophilia in the current study was less than that reported by studies in other Iraqi governorates17,28,30 and in other countries like Saudi Arabia, 33 Egypt, 34 Iran, 4 and Brazil. 24
In comparison with other areas of Iraq and neighboring countries, the relatively low percentage of HCV infection in the current study may be due to this study included only children aged ≤ 18 years old, while other studies included hemophilic patients from all ages. In addition, more availability of the recombinant factors in the CHBD in the last years with more effective screening of blood and its products for viral infection may have a role. Infection with HCV was likely related to treatment due to shortage or sometimes unavailability of therapeutic factor concentrates in the center with exposure of the patients to the blood and blood products (fresh frozen plasma, or cryoprecipitate). Patients with HCV infection in this study treated with Epclusa drug (antiviral medication that contains Sofosbuvir and Velpatasvir) which is available in Baghdad city (capital of Iraq). No HBV cases reported in this study. Hepatitis B vaccine is available in CHBD and received by all patients. This study demonstrated that a statistically significant percentage (40%) of the patients with hemophilia (41.4% with HA and 27.3% with HB) develop target joints. This result was less than the results of other studies conducted in Baghdad 17 and in Diyala, 28 and that conducted in Brazil. 24 This study founded that chronic complications of hemophilia as inhibitors development and arthropathy were more among those with severe disease (22% and 46.3%, respectively), findings similar to that of other studies.10,24,28,32,33
More than one-third of patients with HA and half of those with HB in this study presented firstly with skin bleeding, followed by hemarthrosis and gum bleeding, and less commonly with umbilical bleeding and epistaxis, a finding similar to that of other studies.3,27 In the current study, 48.2% of the patients with hemophilia were on prophylactic therapy either alone or with on demand regimen, which is less than the percentage reported for Iraq (100%) in WFH, 2022. 7 Prophylaxis therapy is important in reducing bleeding episodes and hospitalization and thus improves the quality of life for patients with hemophilia. 4 The low percentage in this study may related to poor adherence of the patients to the treatment regimen or unavailability of recombinant factor concentrate in the center. From 13 patients with HA and inhibitors against FVIII in this study, 7 patients (53.8%) received emicizumab drug which is humanized monoclonal antibody that bridges activated factor IX and factor X to restore the function of factor VIII. 35 In Thi-Qar center for hereditary blood disease, emicizumab drug has been available for patients with hemophilia A and inhibitors against FVIII since April 2021.
Limitations of the Study
It is a single-center study, relatively small sample size, unavailability of screening and genetic testing for diagnosis of asymptomatic patients, and lack of recent studies on hemophilia prevalence in the other Iraqi governorates for more accurate comparison.
Strengths of the Study
It is the first study that calculated the prevalence of hemophilia in Thi-Qar, therefore it is useful as a baseline study for comparison with future advanced studies.
Conclusion
From this study we can conclude that the prevalence of hemophilia in Thi-Qar was higher than the total prevalence in Iraq and some neighboring countries. The inhibitors are detected primarily among patients with HA. Arthropathy and HCV were less prevalent than in some Iraqi governorates and other countries. About half of the patients with hemophilia were on prophylactic therapy. Emicizumab drug has been available for treatment of patients with HA and FVIII inhibitors.
Hemophilia is uncommon disease but imply a great impact on the patient life, their family and health care system. Improvement in comprehensive health care like early diagnosis, proper supportive therapy, as well as rehabilitation of individuals with arthropathy make those patients live longer with better quality of life.
Supplemental Material
sj-doc-4-gph-10.1177_2333794X241280119 – Supplemental material for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq
Supplemental material, sj-doc-4-gph-10.1177_2333794X241280119 for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq by Ghada Mansoor Abood, Raid Kareem Dehiol and Hayfaa Mohammed Mones in Global Pediatric Health
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241280119 – Supplemental material for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq
Supplemental material, sj-docx-1-gph-10.1177_2333794X241280119 for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq by Ghada Mansoor Abood, Raid Kareem Dehiol and Hayfaa Mohammed Mones in Global Pediatric Health
Supplemental Material
sj-docx-2-gph-10.1177_2333794X241280119 – Supplemental material for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq
Supplemental material, sj-docx-2-gph-10.1177_2333794X241280119 for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq by Ghada Mansoor Abood, Raid Kareem Dehiol and Hayfaa Mohammed Mones in Global Pediatric Health
Supplemental Material
sj-docx-3-gph-10.1177_2333794X241280119 – Supplemental material for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq
Supplemental material, sj-docx-3-gph-10.1177_2333794X241280119 for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq by Ghada Mansoor Abood, Raid Kareem Dehiol and Hayfaa Mohammed Mones in Global Pediatric Health
Supplemental Material
sj-docx-5-gph-10.1177_2333794X241280119 – Supplemental material for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq
Supplemental material, sj-docx-5-gph-10.1177_2333794X241280119 for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq by Ghada Mansoor Abood, Raid Kareem Dehiol and Hayfaa Mohammed Mones in Global Pediatric Health
Supplemental Material
sj-docx-6-gph-10.1177_2333794X241280119 – Supplemental material for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq
Supplemental material, sj-docx-6-gph-10.1177_2333794X241280119 for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq by Ghada Mansoor Abood, Raid Kareem Dehiol and Hayfaa Mohammed Mones in Global Pediatric Health
Supplemental Material
sj-docx-7-gph-10.1177_2333794X241280119 – Supplemental material for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq
Supplemental material, sj-docx-7-gph-10.1177_2333794X241280119 for Prevalence of Hemophilia and Clinicodemographic Characteristics of Hemophilic Patients Aged ≤ 18 Years in Thi-Qar, Iraq by Ghada Mansoor Abood, Raid Kareem Dehiol and Hayfaa Mohammed Mones in Global Pediatric Health
Footnotes
Acknowledgements
The authors are particularly grateful to the staff and the medical records department of the CHBD for their cooperation during the study. We would like to thanks all study individuals and their families to participate in this study, CHBD manager, and the scientific committee of the Medical college for their permission to do this research.
Author Contributions
GMA: Contributed to conception and design; contributed to acquisition; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
RKD: Contributed to acquisition and analysis; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
HMM: Contributed to conception; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.