
Abstract
Objective. Neonatal hypothermia is a worldwide health burden with an incidence ranging from 32% to 85% in hospitals and 11% to 92% in homebirths. It is prevalent in Nepal and associated with increased morbidity and mortality. The study objective was to identify key practice standards of newborn thermal management in Nepal. Methods. Our subjects included 6 lead newborn physicians from major birthing centers in Kathmandu. A modified Delphi process was used to identify the top 5 key practice standards for newborn thermoregulation in the hospital, health post, and home, compiled from 14 World Health Organization recommended practices. Results. There was consensus in all ranked practices except using radiant heat sources in the hospital and performing Kangaroo Mother Care in the homebirths. Comments conveyed that interventions during the immediate delivery phase were most impactful and feasible. Conclusion. Nepali physicians prioritized thermoregulatory practices during the immediate resuscitation period over the post-resuscitation period.
Background
Annually, almost 3 million newborns die within 28 days of birth. An overwhelming majority of these deaths occur in low- and middle-income countries (LMICs), 1 accounting for 98% of overall newborn fatalities. Many of these deaths can be prevented with improvements in both newborn care and care provided during the intrapartum period.2,3 Multiple affordable and well-studied interventions prevent or manage common conditions that lead to neonatal mortality, including perinatal asphyxia, sepsis, and prematurity. These interventions have contributed significantly to lowering neonatal mortality. 1 However, neonatal hypothermia is a meaningful contributor to neonatal mortality that is often overlooked. 4
Temperature regulation in newborns is crucial for survival, with premature or low birthweight infants being particularly susceptible to hypothermia. 5 Hypothermia is defined as core body temperature <36.5°C by the World Health Organization (WHO), and has been associated with increased morbidity and mortality in newborns. 6 Neonatal hypothermia is a common global issue, with reported prevalence rates ranging from 11% to 95%.5,7 Hypothermia, especially during the first 12 hours of life, is greatly associated with the risk of death when present with severe infections, prematurity, and asphyxia.5,7-9 Neonatal hypothermia can be effectively managed with appropriate newborn care practices, but implementation of such practices has proven difficult in resource-limited settings.10-12
In 2022, the WHO Guidelines Review Committee approved and released their Recommendations on Newborn Health. 13 These guidelines contain 14 thermal care recommendations to reduce heat loss during and after resuscitation, such as Kangaroo Mother Care (KMC), breastfeeding within the first hour of life, and delaying the bath until 6 hours after birth. These recommendations are supported by robust literature studying these guidelines’ efficacy in preventing hypothermia. For example, based on a meta-analysis of 11 trials with 2000 or more participants as evidence, the WHO concluded that KMC was associated with a reduction in infant mortality and morbidity, including hypothermia.13-15 Additionally, initiation of breastfeeding within 1 hour of birth was found to be effective in preventing neonatal hypothermia, as validated by 9 systematic reviews published by the Cochrane Pregnancy and Childbirth Group, Cochrane Neonatal Review Group, and other independent authors.16-18
In 2022, the neonatal mortality rate in Nepal was 21 per 1000 live births, which was unchanged from 2016. 19 In Nepal, although the number of homebirths has been declining, it was found that 20% of births still occurred in the home. 19 Additionally, the prevalence rates for neonatal hypothermia in Nepal in both rural and hospital settings are still reported to range from 26% to 92.3%. 5 One community-based study found almost all infants in Nepal have hypothermia at birth, 20 while another large study outside of Kathmandu found that 43% of liveborn infants were hypothermic within the first 6 hours of life. 21 This high rate of hypothermia has been linked to excess neonatal death, with one study in rural Nepal finding that for every 1°C decrease in axillary temperature, the adjusted mortality risk increased by 80%. 22 Despite the high prevalence of hypothermia, it has been found that the WHO recommendations on thermal management are not universally followed in Nepal birth settings. One study documented that as low as 10% of Nepali infants receive optimal thermal care. 11 Overall, there is no current nationally accepted standard of care for neonatal thermal management for any birth setting in Nepal. Therefore, the purpose of this study was to develop a set of key practice standards for proper neonatal thermal management in Nepal, based on the expertise of Nepali physicians and aligned with the WHO Recommendations on Newborn Health.
Methods
This study used a modified Delphi technique using in-person discussions and anonymous online surveys to reach a consensus on the most impactful newborn thermoregulatory practices. Delphi studies are a way to reach consensus on a specific question or topic using a relatively small pool of experts in the field, usually over multiple rounds of in-person discussions followed by anonymous surveys. 23 Our study was conducted in the Kathmandu Valley, Nepal’s largest metropolitan area with a population of roughly 3.1 million people. Responses were gathered from May 2022 to December 2022. Interviews were conducted by the lead author of this paper, who was a male MD neonatal/perinatal medicine fellow. The 6 study participants were selected from a sample of lead neonatologists or newborn pediatricians from large hospital birthing centers in the Kathmandu Valley. They were identified by the Nepal National Innovation Center (a nonprofit organization affiliated with Tribhuvan University) as clinical experts and stakeholders in neonatal care. Each participant was invited to join a summit discussing the status of neonatal thermoregulation and future innovations on neonatal hypothermia in Nepal where they met the study team. The exclusion criteria were if any participant was unwilling or unable to complete follow-up surveys after the summit. We did not employ a sample size calculation for our study as there is no consensus on the minimum number of participants to conduct a modified Delphi study. However, we found in the literature samples as low as 4 to 6 can result in adequate expert representation. 24 As this was an initial effort to establish a forum of experts in Nepal the extent of data saturation with respect to the ideal sample of Nepali experts in neonatal resuscitation and stabilization was not evaluated.
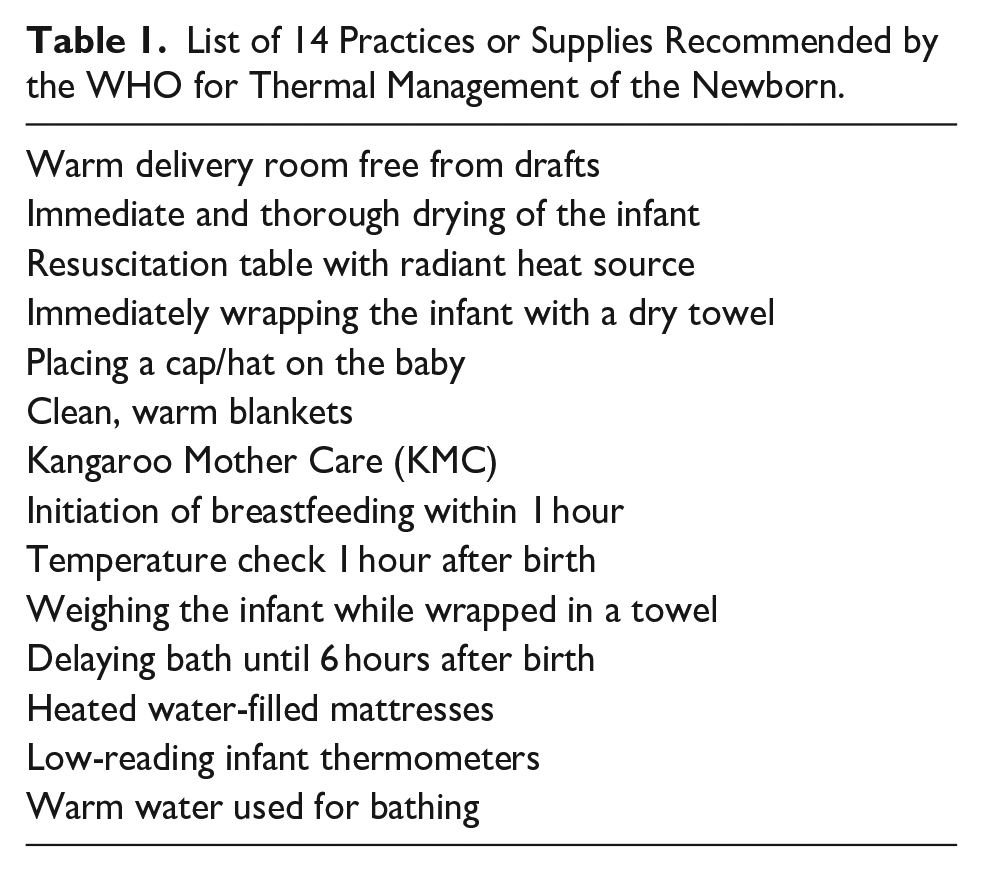
A list of key thermoregulatory management factors was compiled from the WHO Recommendations on Newborn Health. 14 From this document, we identified 14 practices recommended to prevent newborn hypothermia listed in Table 1.
List of 14 Practices or Supplies Recommended by the WHO for Thermal Management of the Newborn.
Our study took place over 1 introductory session and 2 survey rounds. The introductory session was in-person, while the 2 survey rounds were virtually held (Figure 1). The introductory session was held in Kathmandu at a summit discussing the status of neonatal thermoregulation practices and future innovations in Nepal. During the summit, a 2-hour focus group was formed where we shared the 14 practices recommended by the WHO. The strengths and weaknesses of each practice were discussed, as well as whether these practices were already implemented at each of the physicians’ respective hospitals. No audiovisual recording was used, but all 3 study team members present took field notes that were read back to participants at the end of the session for confirmation. After the summit, 2 survey rounds were conducted over an anonymous online survey using Qualtrics software (version June, 2022, Copyright 2024, Qualtrics, Provo, UT) under our institutional license. Qualtrics and all other Qualtrics product or service names are registered trademarks or trademarks of Qualtrics, Provo, UT, USA. These surveys were not validated by previous studies. However, this survey was pilot-tested for functionality and content by multiple users not included as subjects, including two Nepali speakers.
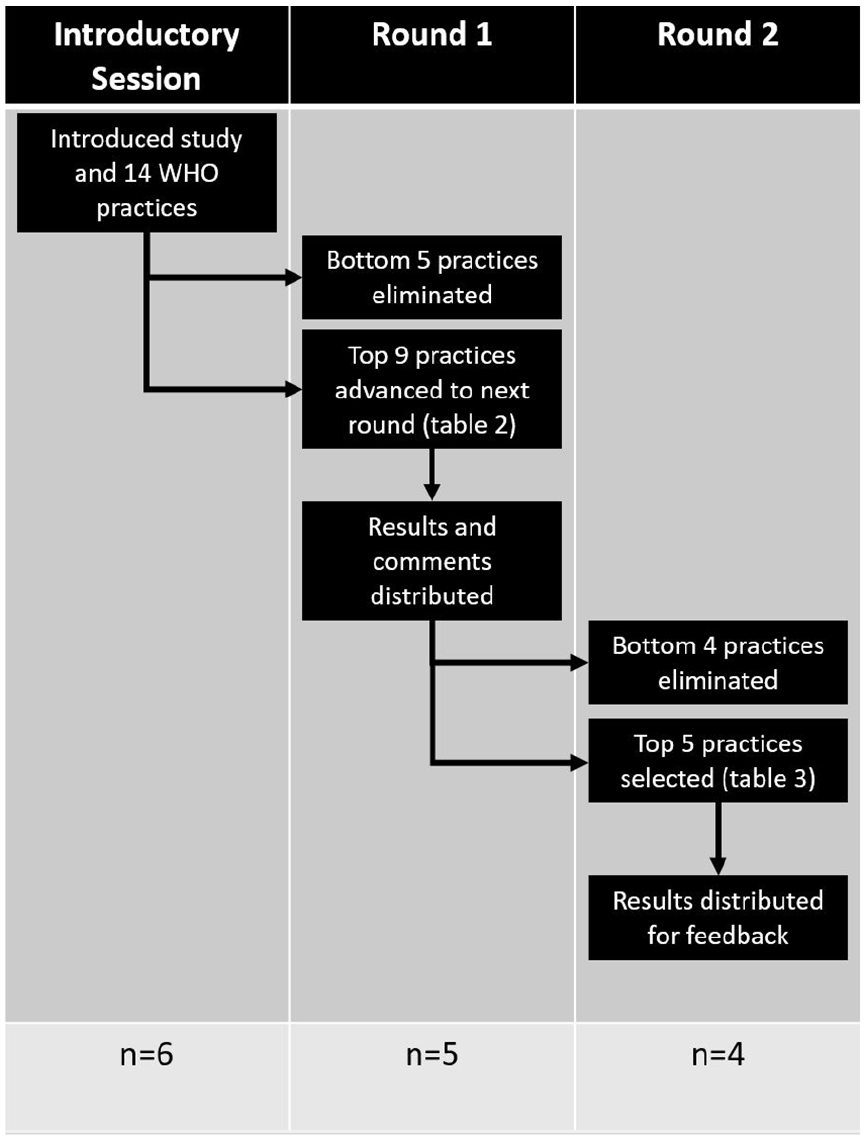
Flowsheet of Delphi survey process over 2 rounds with the number of respondents.
In both of the survey rounds, the physicians ranked each of the WHO practices from “most important” to “least important” in descending order for 3 distinct birth settings: (1) in a hospital, (2) in a health post, and (3) in the home. The subjects were also asked to provide free-text rationale for their rankings. For the first round, the scores were aggregated, and of the 14 practices, the bottom 5 (ie, designated as “least important”) were removed. For the second survey round, a de-identified document summarizing all the first survey round responses was redistributed to the group, where the physician participants were again requested to rank the remaining 9 practices. A final list comprised of the top 5 factors identified as “most important” was distributed to the participants, and final comments on this list were obtained. Our primary outcome was the top 5 “most important” thermoregulation practices in the above 3 settings. Our secondary outcomes were explanations from the of the qualitative feedback on why some factors were more important or feasible than others. As this was an initial effort to determine barriers for further study and our access to the subjects for follow up was limited, general feedback was obtained without using a team to code the responses and develop themes or reengaging participants until saturation was reached. The comments from the surveys were summarized and edited for spelling and grammar, since English was a second language for all participating physicians. The general summery of comments for each round were compiled and circulated between each round and in the final results.
Statistical Analysis
The final ranking of each thermal regulatory practice was assessed for agreement amongst respondents. The mean and standard deviation of the final rank were calculated to evaluate the agreement. There are many ways to define agreement in Delphi studies, but for our purposes, we defined agreement as the final ranking having a standard deviation (SD) of ≤25% of the range of ranks, which for our final round was ≤2.25. 25
Ethical Approval and Informed Consent
This study was submitted the University of Utah institutional IRB (ref: IRB_00157939) and found to be exempt under Category 2 as the study only included an anonymous survey and interview procedures. All subjects gave their written informed consent electronically to be anonymously included in the study via the survey process. The language of this consent was approved by our institutional IRB.
Results
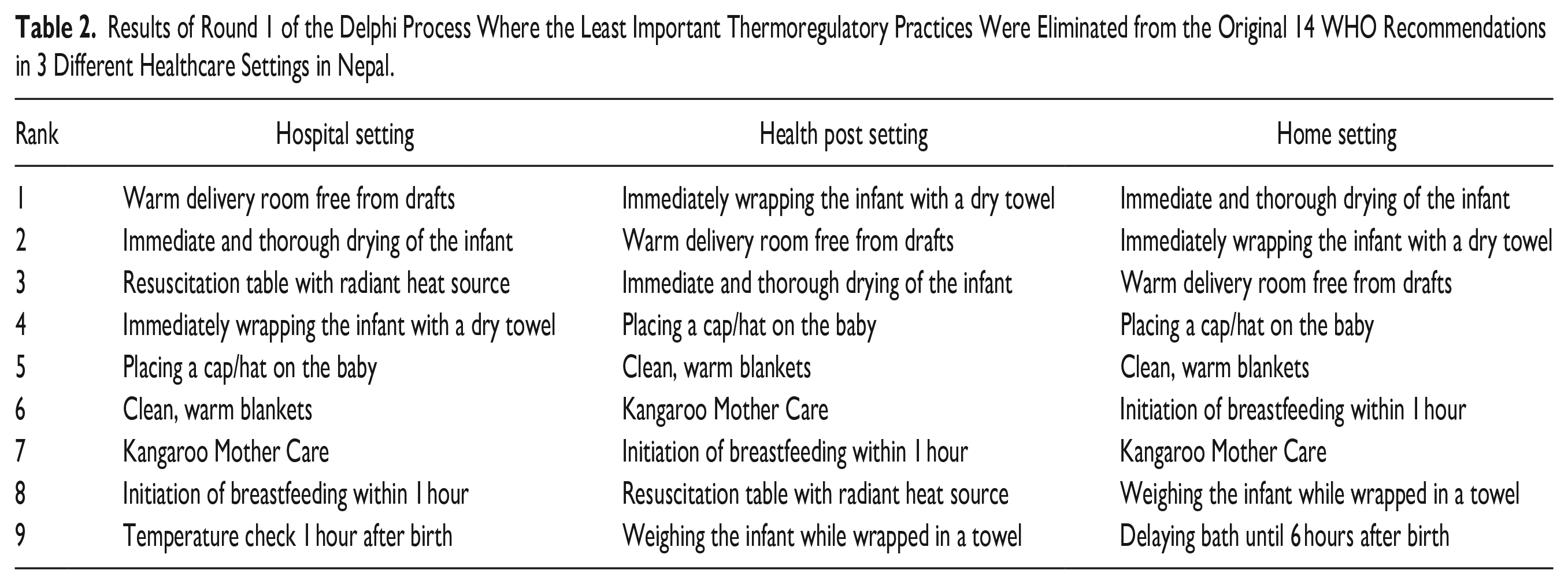
A total of 6 Nepali physicians participated in our focus group, with 5 physicians participating in the first-round survey and 4 physicians in the second-round survey. The intermediate results from the first round of the Delphi process are listed in Table 2, while the final rankings of thermoregulation practices are listed in Table 3. Agreement was reached in the final ranking except for the presence of a “resuscitation table with radiant heat source” in the hospital setting (SD = 3.1) and “Kangaroo Mother Care” in the homebirth setting (SD = 3.2). The predominant arguments from the survey comments were that practices that help prevent heat loss during resuscitation (the highest risk time for heat loss) were “most important,” as demonstrated by one respondent’s comment below: “It is very important to keep delivery room warm to prevent newborn from hypothermia. It’s the main time period where babies lose heat by different methods as well.”—Respondent 1
Results of Round 1 of the Delphi Process Where the Least Important Thermoregulatory Practices Were Eliminated from the Original 14 WHO Recommendations in 3 Different Healthcare Settings in Nepal.
Top 5 Key Practice Standards Identified by Local Lead Physicians for Thermal Management in Different Healthcare Settings in Nepal.

No agreement as defined by standard deviation ≤25% of the total ranking range.
Many practices listed as “least important” were noted not to be feasible due to implementation cost or practicality. Practices that did not directly treat hypothermia were viewed as important but less important than those that directly treated hypothermia. Major barriers identified by participants for each site are listed in Table 4. Summarized, anonymous comments are included as a Supplemental File to this manuscript.
Barriers for Individual Practice Implementation in Each Location Identified Through Free-Text Feedback on Surveys.

Discussion
Using the Delphi method, we identified the top 5 key practice standards as determined by Nepali pediatric physicians for thermoregulation of the newborn in Nepal for the hospital, health post, and homebirth settings. To our knowledge, this is the first consensus list of neonatal thermal regulation practices exclusively produced by physicians from Nepal. Despite the inherent variation of the 3 distinct birth settings with a wide range of available clinical expertise and resources, the top 5 standards remained similar across each setting. Based on the survey comments, the majority of the final standards are practices that prevent heat loss during the high-risk period immediately after birth. While it has been well established that the first hour of life is the highest risk time for developing hypothermia as a neonate, focusing exclusively on heat loss at delivery can expose infants to increased heat loss in the early post-natal period where infants are still at elevated risk for hypothermia. 26 This is especially true for premature infants, low birthweight infants, or infants born in delivery locations without environmental heat sources.
Some factors were viewed as “least important” in the survey results due to their impracticality in low-resource birth settings such as the home and some health posts. For example, it may not be feasible for a health post with limited access to electricity to have a resuscitation table with a radiant heat source, and even simpler options, such as low-reading thermometers, may also be unavailable in these locations. Even in hospitals with access to more sophisticated medical equipment, such as resuscitation tables, access to low-reading thermometers was ranked as one of the “least important” factors for managing thermoregulation. Survey comments from the thematic analysis explain that thermometers do not necessarily treat hypothermia and, therefore, are less important for thermoregulatory management. Studies have examined tactile evaluation of temperature in newborns in Nepal, reporting a sensitivity of 11% to 42% to detect cold stress (36°-37°C) and a sensitivity of 93% to 100% to detect hypothermia (<36°C), which suggests that there is room for improvement in the early detection of poor thermoregulation. 27
KMC is another widely studied and low-cost thermal management practice with robust data on its impact on hypothermia and survival, particularly in LMICs. The WHO and the United Nations Children’s Fund recommend facility-based KMC as a routine care method for clinically stable newborns weighing 2000 g or less at birth. 28 Despite this, our results demonstrated that KMC made the list of top 5 practice standards only for the homebirth setting (although the defined study agreement threshold was not reached), while being notably absent in the hospital and health post settings. Based on comments from the subjects, KMC was viewed as a supplementary practice that did not have as large an impact on hypothermia as the initial resuscitation and, therefore, was not prioritized. Interestingly, while there are studies in hospital settings in Nepal that show there is a benefit to KMC, these centers similarly struggle to implement this practice regularly in their units. 21 In a recently published study analyzing the determinants of KMC care in LMICs, the uptake of this practice had wide variability ranging between 11.0% and 83.5%. 29 In a systematic review outlining the barriers and enablers to KMC adoption, several themes emerged that included buy-in and bonding, social support, time, medical concerns, training, and cultural norms. 30 Further investigation is required to understand the context-specific reasoning behind excluding KMC care as a crucial step in neonatal care within institutional settings.
Additionally, delaying a bath until after 6 hours and using only warm water were both perceived as “less important” per the survey. From the published account of a nurse raised in a rural village in southern Nepal, the infant traditionally is bathed immediately after the umbilical cord is cut, and not all households have access to warm water. 31 This may explain why these were some of the first factors to be eliminated after the first survey round and could be a focus for further intervention.
While our study has demonstrated insight into the perceived importance of thermoregulatory practices of the newborn, it is important to acknowledge the limitations of our study design. First, we had a small subject group, with only 6 physicians participating in the study. This sample size was based on the number of experts available, not a sample size calculation. Though given the small starting subject pool, our survey response rate was robust at 75%. Secondly, we aimed to exclusively recruit physicians from the Kathmandu Valley in our subject group without including physicians outside of Kathmandu, midwives, or nurses. While this was done to focus the participant pool, this also created a non-representative sample of birth attendants in Nepal. For future studies, insight from those who attend homebirths and manage health posts (eg, midwives, nurses) would be useful for improved representation of Nepali birth attendants. Additionally, we did not use a previously validated survey for this study; rather, it was a survey designed and piloted by our research group. Finally, while this study concentrated on finding the most important factors to prevent hypothermia, there is the opportunity for a Nepali hospital to adopt the 14 identified thermoregulation practices from the WHO Recommendations on Newborn Health as part of their standard of care. Despite the limitations, this study provides critical information that can guide further development and implementation of national thermal care protocols across Nepali delivery settings.
Conclusion
Our study surveyed 6 leading neonatal physicians in Nepal to prioritize thermoregulatory practices to prevent neonatal hypothermia and a Delphi process was used to identify key practice standards for neonatal thermal management. We found that practices that protect infants from hypothermia in the initial resuscitation phase were prioritized over other well-studied practices (such as KMC) that protect the infant in the first few days of life. Additionally, the factors chosen were relatively similar across all birth settings. Moving forward, partnerships with midwives and nurses to understand current curricula and practices will need to be implemented. Future training, including increased emphasis on KMC and measuring the baby’s temperatures, will be required to further reduce hypothermia in Nepal.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241273300 – Supplemental material for Determining Consensus Alignment and Barriers of Neonatal Thermal Management in Nepal Using a Modified Delphi Process
Supplemental material, sj-docx-1-gph-10.1177_2333794X241273300 for Determining Consensus Alignment and Barriers of Neonatal Thermal Management in Nepal Using a Modified Delphi Process by Brandon Tomlin, Bibec Lamichhane, Ranjan Dhungana, Grace Richards, Peter Grubb, Anamika Mahato, Bernhard Fassl and Allison Judkins in Global Pediatric Health
Footnotes
Acknowledgements
We would like to acknowledge the Nepal National Innovation Center, whose support made it possible to host our focus group on hypothermia. We would also like to acknowledge the Nepali physicians who participated in this study.
Author Contributions
Authors BT, BL, RD, PG, BF, and AJ all contributed to the conceptualization and methodology of the study. Authors BT, BL, RD, AM, BF, and AJ contributed to the investigation of the study. Authors BT, GR, and PG contributed to the formal analysis. Authors BT, GR, BF, and AJ contributed to the initial writing of the original draft and all authors contributed to the review and editing of the manuscript. All authors agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This study was submitted to the University of Utah IRB (ref: IRB_00157939) and found to be exempt under Category 2 as the study only included an anonymous survey and interview procedures. All subjects gave their informed consent electronically to be anonymously included in the study via the survey process.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.