
Abstract
Introduction. Respiratory distress (RD) contributes to common causes of neonatal mortality. Bubble continuous positive airway pressure (bCPAP) is a safe, low-cost therapy for RD; however, adoption of bCPAP programs remains challenging. Aim. To increase the percentage of neonates with RD treated with bCPAP from 2% to 25% by January 2019. Methods. In the newborn unit (NBU) at the Nakuru County and Referral Hospital in Kenya, a pre-initiative (pre) period (March 2016 to December 2017) and a post-initiative (post) period (January 2018 to December 2018) were defined. Tests of change included organization of infrastructure, staff trainings, development of a nurse educator role, and treatment protocols. Clinical and outcome data were abstracted from all available medical records. Results. A total of 405 infants were included in the pre group, with 2% bCPAP use. A total of 1157 infants were included in the post group, with 100 (17.6%) treated with bCPAP. bCPAP use increased during the post period. Rates of RD (49.9% pre, 49.0% post, P = .64) and mortality (30.9% pre, 29.1% post, P = .35) were similar. Neonates treated with bCPAP had lower mean birth weight and a higher risk of death (relative risk = 1.41, 95% confidence interval = 1.21-1.65) compared with those not treated with bCPAP. Conclusion. It was possible to build capacity for the use of bCPAP to treat neonates in this low-resource setting. Gaps in the delivery bCPAP remain, and the current capacity in the PGH NBU allows for application of bCPAP to smaller, likely, sicker neonates.
Keywords
Introduction
Neonatal mortality disproportionally occurs in resource-limited areas of the world. In Kenya, the neonatal mortality rate remains high at 22 per 1000 livebirths. 1 Respiratory distress contributes to all 3 of the most common causes of neonatal death worldwide: prematurity, birth asphyxia, and sepsis. 2 Limited health care system capacity to deliver care to neonates with respiratory distress in low-resource settings contributes to the high neonatal mortality rate in these areas. Feasible and sustainable care process models for the treatment of neonates with respiratory distress in low-resource hospital settings are needed. 3
Bubble continuous positive airway pressure (bCPAP) is considered standard of care for treatment of neonates with respiratory distress by many national and international health organizations including the World Health Organization (WHO) and the Ministry of Health in Kenya.4,5 bCPAP is an attractive treatment modality in low-resource settings, given that compared with mechanical ventilation, it is less expensive, requires less technical skill to operate, and has a lower risk of complications to the patient. Treatment with bCPAP reduces the need for mechanical ventilation, and there are a number commercial bCPAP devices designed to be cost-effective and easy to maintain.6-9
A pre-initiative review (March 2016 to December 2017) of 407 infants admitted to our hospital, the Nakuru County and Referral Hospital in Nakuru, Kenya, showed that 201 infants (49%) had respiratory distress at the time of admission. Of these, 160 infants (80%) were treated with oxygen via nasal cannula. Despite unit knowledge of and access to supplies to create bCPAP circuits using plastic water bottles and the availability of bCPAP machines at the end of the pre-initiative period, only 4 infants (2%) with respiratory distress were treated with bCPAP. The aim of our quality improvement (QI) initiative was to increase the percent of neonates with respiratory distress treated with bCPAP from 2% to 25% over a 12-month period (January 2018 to December 2019) in the newborn unit (NBU) of the Nakuru County and Referral Hospital in Nakuru, Kenya. Using existing hospital resources, we sought to develop a replicable operational framework to implement bCPAP as a treatment modality in a low-resource referral hospital.
Methods
The Setting
Nakuru County and Referral Hospital is the obstetric and neonatal referral center for high-risk deliveries that occur within the public health sector in Nakuru County, which has a population of 2.1 million. Around 1000 deliveries occur in the hospital each month, and roughly 10% of infants born require advanced pediatric care in the NBU. The NBU is the only public health facility offering advanced newborn care in Nakuru County, and the NBU has a daily patient census of approximately 50 throughout the year. The most common admission diagnoses to the NBU are low birth weight (<2500 g) and birth asphyxia. Two pediatricians share the rounding duties in the NBU. Medical officer interns from Egerton University, the affiliated public medical school in Nakuru, Kenya, rotate through the unit on a monthly basis and are present on the unit 24 hours a day. There are 14 nurses on staff, and one has formal training in general pediatrics. Nursing duties are divided into three 8-hour shifts with 2 nurses working during day shifts and 1 nurse working at night. Staff turnover is not frequent in the NBU; however, health care workers’ leaves of absence and strikes are common and cause labor shortages and unit closures.
The respiratory support mode most commonly administered in the NBU is oxygen via nasal cannula. Prior to November 2018 and the installation of piped oxygen, oxygen cylinders were used. During the pre-initiative period, international visitors provided education on the use of bCPAP circuits made from plastic water bottles. Instructions on assembly of these circuits were posted in the admission area, and these water bottles were available in the unit storage area. In October 2017, the NBU acquired 6 bCPAP devices. Two devices used in the NBU were purchased by the hospital, and 4 devices were purchased with WHO research funding not associated with this initiative. These devices are Pumani (Pumani bCPAP) and Diamedica (Diamedica Baby CPAP 20 LPM) models. Electricity to power bCPAP machines is reliably available in the NBU. Chest radiographs are not routinely obtained, and blood gas analysis is not available. There was 1 pulse oximeter in the NBU until November 2018, at which time 6 pulse oximeters became available. Antenatal steroids are administered to women in preterm labor or need for delivery with estimated gestation of less than 34 weeks or less. Surfactant is not administered due to lack of availability.
The Intervention
In the pre-initiative phase, we formed a multidisciplinary QI team of Kenyan stakeholders that included pediatricians, obstetricians, senior nurses, and hospital administrators. The team received training in QI methodology from international collaborators and was introduced to the QI toolkit available through the Institute for Healthcare Improvement, which includes rapid cycle feedback systems using the PDSA (Plan-Do-Study-Act) approach. 10 Jointly, members of the local and international QI team analyzed the existing care process for newborns with respiratory distress and performed a formal gap analysis with regard to NBU capacity to deliver bCPAP. During this process, a focus group was held including 4 senior members of the nursing staff and led by the Kenyan pediatrician and the visiting neonatologist. Following this focus group, a written survey regarding past experience and current attitudes toward CPAP was distributed to all physicians, nurses, and students who worked in the NBU. Throughout the intervention, the head nursing staff reported observed barriers to the QI team. The gap analysis identified the following key drivers of change: (1) improved NBU infrastructure, (2) increased staff knowledge and skill, and (3) standardization of the bCPAP care process (Figure 1). Administrative, educational, and clinical planning steps were taken at this stage to launch improvement interventions. Starting in January 2018, the QI team implemented a series of PDSA interventions with the aim to increase bCPAP utilization. PDSA cycles are grouped by primary driver, and are described below.
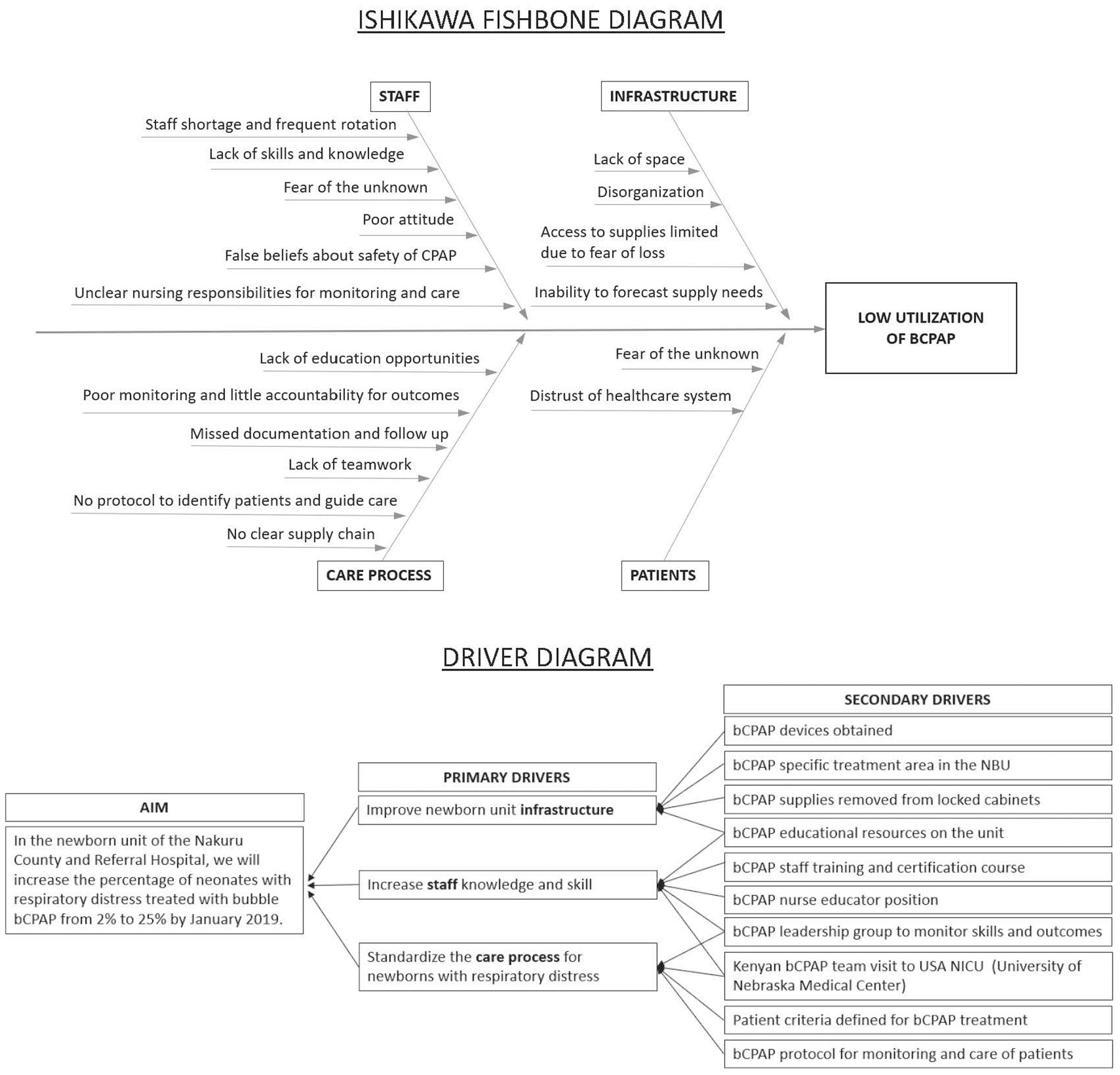
Ishikawa driver diagrams.
Improve NBU Infrastructure
The team designed a bCPAP treatment–specific area in the NBU (PDSA cycle 1). Three bed spaces closest to the nursing station were selected. This was important to nursing staff so that infants on bCPAP could be easily monitored. The area was equipped with supplies (bCPAP machines, nasal prongs of all sizes, tubing and connectors, a suction machine, orogastric tubes, nasal saline, oxygen cylinders, flow meters, hand bag and masks) needed to support a baby on bCPAP. Team members encouraged staff to keep these materials out of locked storage cabinets, as access to supplies was a barrier to initiating bCPAP identified by nursing staff. Reference materials and posters were available at the bedside to assist nurses in set up of the bCPAP machines. In November 2018, the NBU completed a facilities expansion at which point 8 bed spaces were designated as the bCPAP treatment area (PDSA cycle 4).
Increase NBU Staff Knowledge and Skills
A bCPAP training course for physicians and nurses was developed guided by competency goals outlined by the WHO and Kenyan health authorities (PDSA cycle 2). An initial training of nursing and physician staff was completed in February 2018 with follow-up refresher trainings offered in April 2018 and November 2018. The initial 1-day (8 hour) training course was led by the Kenyan pediatrician and the international neonatology team, and the refresher training in November 2018 was entirely directed by Kenyan team members. The training covered the clinical assessment of respiratory distress in the newborn as well as patient selection for bCPAP using the Silverman Anderson Respiratory Severity Score (RSS). The Silverman Anderson RSS was used as the staff had existing knowledge of the score, and it is included in the Kenyan Ministry of Health guidelines for CPAP use. 4 In addition, the course included education on the proper set up of the bCPAP machine, starting bCPAP settings, ongoing monitoring and care of patients on bCPAP, complications of bCPAP, and maintenance of bCPAP equipment. Particular attention was paid to the importance of prevention of nasal septal injury through selection of correct fitting nasal prongs and application of saline to the mucosa at each respiratory assessment. Photographs demonstrating examples of nasal septal injuries were shown. Teaching modalities included didactic, video, and hands-on group activities. bCPAP training videos developed by Rice 360 Institute for Global Technologies were used. 11 All participants were required to pass a practical examination to obtain certification to use bCPAP. Nursing participation in the course was supported by the hospital administration and was considered part of the nurses’ duty hours. No monetary compensation was provided to participants.
Based on a staff survey, the teaching modality most desired by nursing staff was bedside instruction. 12 To meet this request, a nurse educator position was created in the NBU (PDSA cycle 3). The nurse hired for this role was a member of the current NBU nursing staff who had demonstrated excellence in the use of bCPAP. She was individually trained by the Kenyan pediatrician and visiting neonatologist. Her duties included provision of support to nursing staff at the bedside, organization of bCPAP supplies, and maintenance of unit education materials. She reviewed the monitoring tool reports, and identified gaps in care delivery. Her salary was supported by funds from Rotary International.
Standardize the bCPAP Care Process
Patient criteria for bCPAP were defined, and a clinical treatment algorithm, including initiation of bCPAP, escalation and weaning of bCPAP support, patient monitoring, and supportive care for all patients receiving bCPAP, was developed and can be found in the supplemental material (PDSA cycle 2, available online). Inclusion and exclusion criteria for treatment with bCPAP were based on the Kenyan Ministry of Health guidelines. 9 To receive bCPAP care according to these criteria, infants must have: birth weight greater than 1000 g, 5-minute Apgar score ≥5, and a Silverman Anderson RSS >4 (indicating moderate or severe respiratory distress). Infants weighing <1000 g, with severe apnea, gasping respirations, or seizures were excluded from analysis. Both inborn and outborn infants with respiratory distress were eligible to receive treatment with bCPAP.
A clinical monitoring tool for newborns receiving bCPAP, previously developed by Rice 360 Institute for Global Technologies, was added to the medical record. 13 The monitoring tool included patient demographics, date of initiation and cessation of bCPAP, and a table to chart all clinical assessments done by nursing staff. The respiratory examination of the infant was recorded at each assessment. In addition, the tool includes a column to note that saline drops were applied to nasal mucosa. The unit protocol for frequency of monitoring of infants on bCPAP was an assessment 1 hour following initiation of bCPAP or adjustment of settings, and every 6 hours once on stable bCPAP settings. Initial bCPAP settings were a water level of 6 cm and a fractional inspired oxygen percentage (FiO2) of 45%. Changes in the bCPAP support settings that were made in response to the respiratory examination were noted at each assessment.
Outcomes and Measures
The primary clinical outcome was the rate (%) of bCPAP application to neonates with respiratory distress at the time of admission (number of infants treated with bCPAP/number of infants with respiratory distress at admission). Respiratory distress at admission was defined by chart documentation of any of the following: tachypnea (respiratory rate [RR] over 60 breaths per minute), increased work of breathing (chest wall indrawing, retractions, or grunting) or hypoxia (oxygen saturation under 90%). Silverman Anderson RSS was not selected as a measure as it was found to be infrequently used at the bedside and was not documented in clinical charting for review.
Following cessation of therapy, the monitoring tool for each bCPAP case was reviewed for the following data points: day of life (DOL) of initiation of bCPAP, duration of treatment, time to reduction in RR to <60, and time to increase in oxygen saturation to >90. Improvement in respiratory status was defined as obtaining both a RR <60 and oxygen saturation >90 while receiving bCPAP. On review, we determined if each case had received monitoring by nursing staff according to the unit protocol (defined above). The number of respiratory assessments made by nursing staff and the number of these assessments occurring during day and night shifts were recorded.
Process measures tracked monthly during the implementation period included the percentage of nursing staff trained on bCPAP and the number of bCPAP treatment hours delivered. A total of 144 bCPAP hours were possible per day based on availability of 6 devices. In addition, each respiratory assessment recorded in the monitoring tool was reviewed by a member of the international team. This reviewer determined if a response was made in accordance with the bCPAP unit protocol; in other words, the reviewer determined if the bCPAP support was increased in response to an infant with persistent respiratory distress or decreased at the time when an infant met weaning criteria.
Nasal septal injury and mortality among individuals treated with bCPAP were balancing measures and were reviewed by the project team at the end of each PDSA cycle. It was not possible to monitor rates of pneumothoraces as chest X-rays were not routinely obtained.
Data Collection
We obtained demographic, clinical, and care process data through retrospective chart review on all patients admitted to the NBU. The pre-initiative period was March 2016 to December 2017. The implementation period began in January 2018. Starting in January 2018, all available medical records for infants admitted to the NBU were obtained and reviewed every 2 to 3 months. These intervals defined PDSA cycles, and coincided with site visits by members of the collaborating international team. Mortality data for pre-initiative and implementation time periods were collected prospectively from the unit mortality logbook.
Data Analysis
For comparison of patient characteristics and clinical outcomes, the χ2 test was used for categorical variables, and t test was used for continuous variables. The relative risk of death of infants with respiratory distress during implementation who were treated and not treated with bCPAP was compared. Cases with missing data were removed prior to any data analysis that included the missing variable. We used established QI methodology including run charts to monitor clinical outcomes and process measures over time. P charts were used to analyze percentage data, and statistical process control analysis was performed using QI Macros for Excel, version 2018, with the Institute for Healthcare Improvement rules.
Ethical Considerations
The institutional review board at the University of Utah and the ethics committee at Egerton University approved the implementation of this initiative as a QI project. This project received support from Rotary International Global Grant (#GG1862566).
Results
There were 405 infants included in the pre-initiative period and 1157 included in the implementation period (Table 1). The availability of medical charts for review increased in the implementation period. In some cases, medical records were either lost or not created. In the pre-initiative period, 405 charts were available for review of the 956 infants who were recorded in the NBU admission book. In the implementation period, 1157 charts were available for review of the 1327 infants who were recorded in the NBU admission book. Charts were not available for all cases of mortality in both the pre-initiative and implementation periods. There were gaps in the availability of both medical charts and mortality records in the pre-initiative period; some months had no data available.
Demographics of Infants Admitted to the NBU During the Pre-Initiative and Implementation Periods.
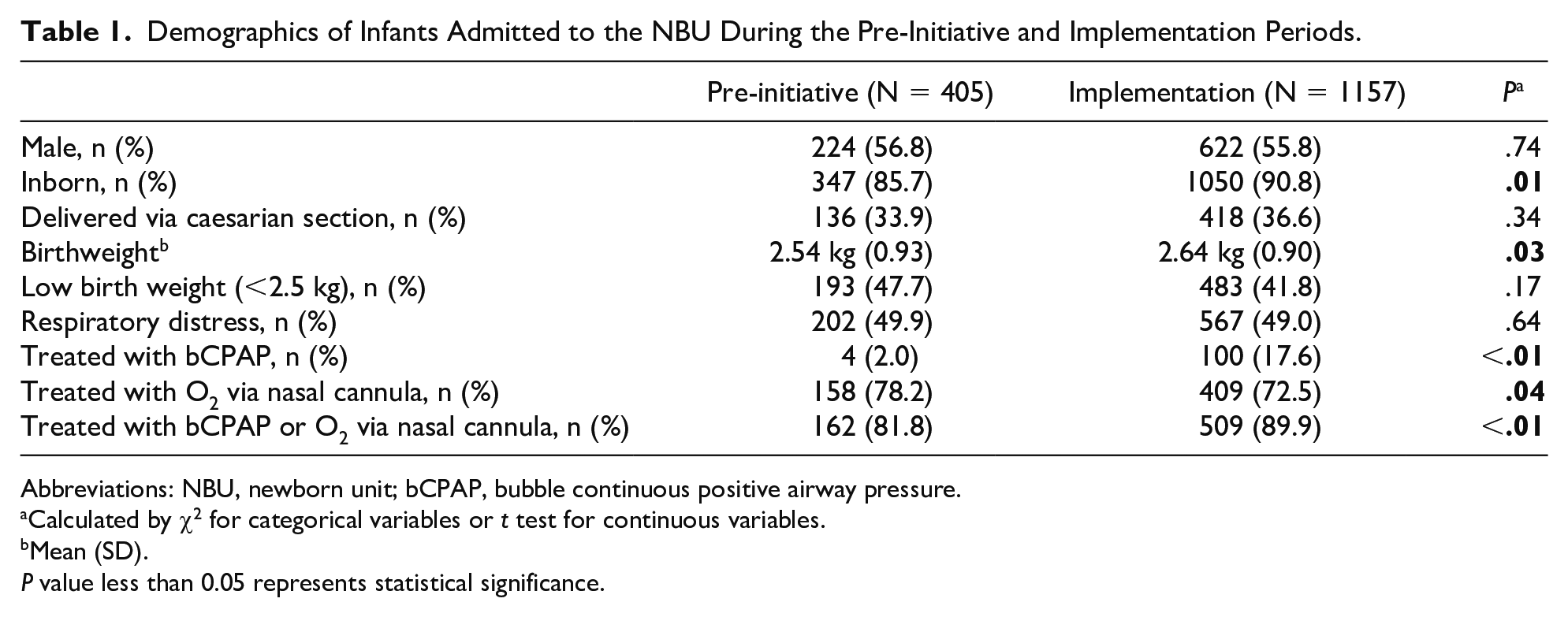
Abbreviations: NBU, newborn unit; bCPAP, bubble continuous positive airway pressure.
Calculated by χ2 for categorical variables or t test for continuous variables.
Mean (SD).
P value less than 0.05 represents statistical significance.
The rate of respiratory distress at the time of admission was similar to pre-initiative and implementation periods (Table 1). Of the cases with respiratory distress on admission, 4 (2%) pre-initiative and 100 (17.6%) during implementation were treated with bCPAP. bCPAP use increased in the implementation period (Figure 2). Infants with respiratory distress on admission were more likely to receive any treatment (oxygen via nasal cannula or bCPAP) during the implementation period (Table 1). Mortality for all infants admitted to the NBU was similar in the pre-initiative (296 deaths/956 admissions; 30.9%) and implementation periods (387 deaths/1327 admissions; 29.1%), P = .35. Mortality among the group treated with bCPAP during the implementation period decreased from a high of 56% in PDSA cycle 2 to a low of 22% in PDSA cycle 4 (Table 2).
Mortality of Infants Treated With bCPAP During Each PDSA Cycle During the Implementation Period.
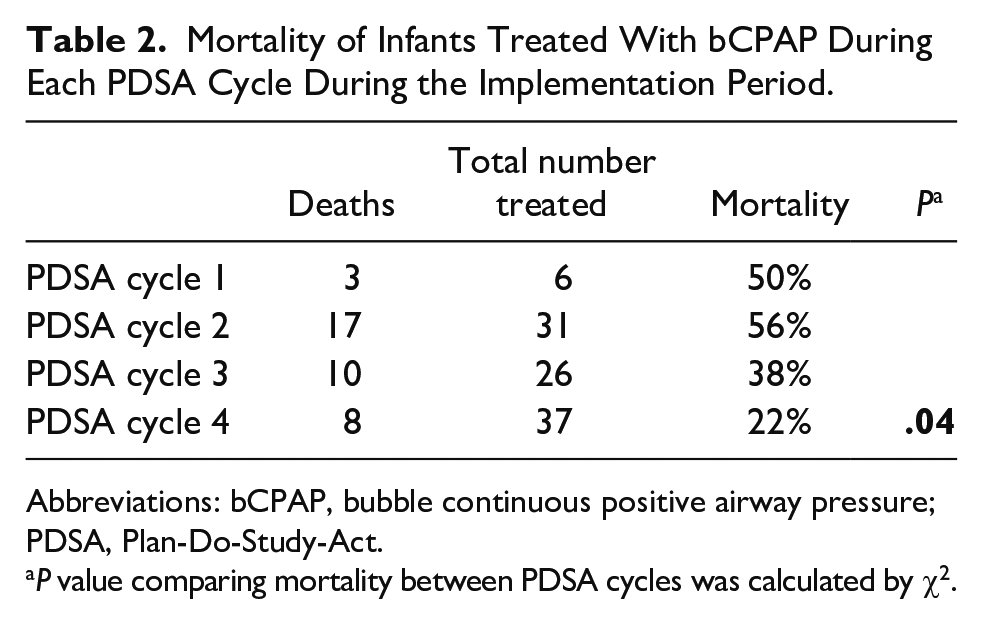
Abbreviations: bCPAP, bubble continuous positive airway pressure; PDSA, Plan-Do-Study-Act.
P value comparing mortality between PDSA cycles was calculated by χ2.

Monthly rate of bubble continuous positive airway pressure (bCPAP) use among newborns with respiratory distress admitted to the newborn unit (NBU). P chart with control limits at ±3 sigma lines. Shaded vertical bars represent time periods with labor interruption.
In the implementation period, neonates treated with bCPAP had lower mean birthweight (Table 3) and higher risk of death (relative risk = 1.41, 95% confidence interval = 1.21-1.65) compared with those not treated with bCPAP. The majority of treated patients were of low birthweight (Table 4). The dates of bCPAP treatment were recorded for 73 out of 100 cases. Of these, all infants were started on bCPAP within the first week of life with 41 (56%) placed on bCPAP on DOL 0. bCPAP was applied on DOL 1 in 26 (36%) cases. The remaining 6 (8%) cases were placed on bCPAP on DOL 2 to 6. The median duration of bCPAP treatment was 27 hours with a range of 1 to 181 hours. Seventy-five out of 100 infants treated with bCPAP in the implementation period had a clinical monitoring tool recorded. The clinical monitoring data available demonstrated that a RR of less than 60 was attained in 50 out of 75 (67%) cases at an average 18.5 hours (range = 0-98 hours, SD = 24.3) into bCPAP treatment. An oxygen saturation greater than 90 was achieved in 60 out of 75 (80%) cases at an average 7.8 hours (range = 0-46 hours, SD = 11.8) into bCPAP treatment. Forty-five out of 75 (60%) infants treated with bCPAP demonstrated an improvement in respiratory status. No nasal septal injuries in patients treated with bCPAP were observed.
Demographics and Mortality of Infants Admitted to the NBU With Respiratory Distress During the Implementation Period (January to December 2018).

Abbreviations: NBU, newborn unit; bCPAP, bubble continuous positive airway pressure.
Calculated by χ2 for categorical variables or t test for continuous variables.
Mean (SD).
P value less than 0.05 represents statistical significance.
Birthweight of Infants Treated With bCPAP During the Implementation Period (January to December 2018).

Abbreviation: bCPAP, bubble continuous positive airway pressure.
Initial staff training occurred in February 2018 during which 13 of the 14 qualified NBU nurses and both of the 2 pediatricians participated in a formal 1-day training. Twelve out of 13 (92%) nurses and 2 out of 2 (100%) NBU pediatricians passed (scored >84%) the post-training practical examination on their first attempt. Training of nursing staff was maintained at 100% for 6 out of 12 months of the implementation period. There was little staff turnover in the implementation period. New or missed staff were captured at follow-up trainings offered in April 2018 and November 2018. The trainings in February and April were led jointly by Kenyan and international team members. The training in November was led exclusively by the Kenyan team.
Thirty-eight out of 100 (38%) infants on bCPAP in the implementation period were monitored by a nurse according to the unit protocol. Nurses made 823 respiratory assessments of infants on bCPAP during the implementation period. A total of 569 (69%) assessments were made during day shifts (16 of the 24 daily work hours), and 263 (31%) were made during the night shift (8 of the 24 daily work hours). An adjustment was made to the bCPAP support according to protocol after 190 (23%) of the 823 respiratory assessments.
Six machines were maintained throughout the implementation period, and none had reported mechanical failures that limited availability. Only 2627 (5%) of the total 52 560 available bCPAP hours were used during the implementation period. All data are available on request from authors (
Discussion
Following the implementation of our QI initiative, there was a significant increase in the utilization of bCPAP to treat neonates with respiratory distress in the NBU of the Nakuru County and Referral Hospital in Nakuru, Kenya. The rate of bCPAP treatment increased by 9-fold through interventions aimed to improve existing infrastructure, increase staff knowledge and skill, and standardize the care process. Interventions associated with significant change in the SPC analysis were the staff trainings and the employment of the nurse educator (Figure 2). The capacity to deliver bCPAP was sensitive to the labor interruptions or workforce strikes (Figure 2).
Clinical bCPAP programs in low-resource settings have faced challenges.14-16 A country-wide survey in Kenya revealed that only 19 health centers were using bCPAP to treat newborns in 2017. 17 This report indicated that challenges at centers with bCPAP included lack of training of health care providers and poor maintenance of donated equipment. Although some CPAP machines on site were obtained through unrelated research funding, the local hospital had made an investment in its own CPAP machines. Our initiative did not require external investment or donated bCPAP machines. Equipment maintenance was a priority for the local hospital administration, which led to less equipment failures. Both the Pumani and Diamedica bCPAP models were designed specifically for use in low-resource settings, and as such contribute the sustainability of our bCPAP program. CPAP accessories such as nasal prongs and tubing were relatively expensive, and patient safety and sustainability of the CPAP program will rely on the site’s ability to properly clean and reuse these parts.
Another strength of our initiative was the local, multidisciplinary QI team. bCPAP would not have been adopted without consistent engagement of the local project leadership and frontline staff. The availability of bCPAP machines alone did not lead to high bCPAP use, and only a very small percentage of potential bCPAP hours were used each month. The pace of increase of bCPAP delivery was driven by the local capacity and not by the expectations of the international collaborators. This collaborative environment may have allowed for transfer of knowledge and growth of staff skill. Also of particular value to our team was the involvement of Egerton University, a Kenyan academic partner. Team members from Egerton had an existing background in education and familiarity with research, which were vital to our implementation. This local academic partnership facilitated implementation and is a valuable resource to maintain the ongoing staff training and outcome monitoring.
Although there is global interest in expanding capacity to use bCPAP to treat newborns in low-resource settings, studies reporting detailed implementation strategies are few. 18 Wilson et al 19 published the only available comprehensive bCPAP training package intended for use in low- and middle-income countries to train both neonatal and pediatric care providers. This program uses the training-of-trainers (TOT) methodology and includes low-cost educational materials similar to those used in our training package. They report that their program has trained 104 instructors in 4 countries (Cambodia, Kenya, Rwanda, and Honduras), but details regarding the impact of training on the delivery of bCPAP to neonates and children and the impact on clinical outcomes are yet to be published. They do emphasize the importance of strong buy-in of local partners for the adoption of this new technology, which was comparable to our experience with bCPAP implementation.
McAdams et al 20 reported the implementation of a bCPAP treatment program in a neonatal intensive care unit in a referral hospital similar to ours in central Uganda. As in our training, this program used the Silverman Anderson RSS to assess the degree of respiratory distress. In contrast to our experience with the RSS, they report that the RSS was accurate, easily adopted, and that provider skill with the score was maintained over the 6-month study period. During the study period, 21 infants were treated with bCPAP using a water bottle device. This was a feasibility study and as such was not designed to measure outcomes, but it is noteworthy that 9 out of 21 (43%) treated patients died prior to discharge. They reported 3 cases of nasal septal irritation while on bCPAP, but no major complications were observed. They conclude, as we do, that bCPAP is safe and feasible in a low-resource setting.
Effectiveness of bCPAP in low-resource settings to reduce mortality has not been proven conclusively. Multiple retrospective analyses following implementation of bCPAP in low-resource settings suggest that bCPAP does improve mortality from respiratory distress, but no randomized trials compare bCPAP with local standard of care, typically oxygen via nasal cannula.21-23 Furthermore, it is widely accepted that bCPAP is an effective therapy in high-income countries, and the need for as well as the ethics of these randomized controlled trials in low-resource settings is debated.24,25 Kawaza et al 26 reported a quasi-randomized study in which bCPAP delivered with the Pumani device was compared with oxygen via nasal cannula. Infants in this study received bCPAP based on the availability of the device at the time of identification of severe respiratory distress. If bCPAP was not available, oxygen via nasal cannula was applied. Survival rate for neonates treated with bCPAP was 44 out of 62 (71%) compared with 11 out of 25 (44%) in controls. There were no complications of bCPAP reported. This work supports the safety and effectiveness of bCPAP to reduce mortality in a low-resource setting.
Mortality among neonates overall in the NBU did not change following implementation of our initiative. During the implementation period, the relative risk of death in the population exposed to bCPAP was higher than those not treated. We suspect that this reflects selection bias, as evidenced by the lower birth weight of infants selected for bCPAP in the implementation period. At the current capacity smaller, sicker infants are more likely to be selected to receive bCPAP. We were not able to report the severity of respiratory distress of included versus excluded patients due to inconsistency of chart documentation. Thus, it is not possible to test our hypothesis of selection bias. We were also not able to compare mortality of infants with respiratory distress during the pre-initiative time period with that of the implementation period due to missing mortality data in the pre-initiative chart review. This along with other missing clinical data is a weakness of our study. We also cannot exclude the possibility that bCPAP complications such as pneumothorax or secondary pneumonia contributed to the increase mortality in exposed infants, as these data are also not available. Still, we are reassured that mortality among the group with respiratory distress treated with bCPAP during implementation did decline over time suggesting that effective bCPAP was delivered safely as the new technology was adopted and its use improved.
After implementation, we find that a number of gaps remain in the bCPAP care process. Baseline assessment of staff knowledge in the NBU demonstrated that physician and nursing staff were able to identify cases of respiratory distress, and all of the infants placed on bCPAP during implementation had documented respiratory distress signs. 12 However, staff did not always translate their respiratory assessment skills into meaningful bCPAP support adjustments. Review of the monitoring tools revealed that many infants on bCPAP remained tachypneic and hypoxic while receiving clinical assessments that were not followed by an increase in bCPAP support. In addition, infants with respiratory distress at the time of their admission (typically DOL 0) were often started late on bCPAP. These gaps raise a concern that the training interventions did not adequately teach staff to provide effective bCPAP treatment. Another weakness of our study is the lack of longitudinal objective assessments of provider skill following the initial practical examination.
Gaps that remain in the system to deliver bCPAP following our implementation inform the way forward for the bCPAP program. We did not meet the targeted goal to treat 25% of neonates admitted with respiratory distress. We intend to continue similar PDSA cycles aimed at increasing capacity and use of bCPAP machines. Our initiative is well poised to sustain the project beyond implementation given that the local team is now in full control of data collection and review on a monthly basis. Local hospital administration continues to support the bCPAP program through provision of supplies and maintenance of equipment. Furthermore, local QI team members, in particular those from Egerton University, continue to educate new staff independently of foreign influence. We feel that this independence is particularly important for long-term sustainability of any global QI program.
International stakeholders will remain invested in the site now with a particular interest in improving the ability of health care providers to adjust bCPAP settings in response to serial respiratory assessments. Further work is needed to develop training and assessment tools to meet this need. Our intention is to provide additional training in the NBU with a hands-on clinical educational module that could spans multiple weeks. The nurse educator will be vital to this education intervention as would methodical documentation and review of providers skills on an ongoing basis. We will use the PDSA cycle approach to evaluate providers’ response to respiratory assessment to examine the effectiveness of our education intervention.
Our study describes a multidisciplinary QI-based approach to build sustainable capacity for the use of bCPAP in a low-resource setting. The implementation of this hospital-based bCPAP treatment program for neonates with respiratory distress revealed challenges that others undertaking similar initiatives may also encounter. The use of well-described QI techniques enhanced our ability to implement our program. Our experience demonstrates that a sustained effort by a local, multidisciplinary team is required to increase the use of bCPAP. Furthermore, the effectiveness of bCPAP delivery in low-resource settings must be examined closely as implementation does not ensure optimization. We believe that the model for implementation presented here can be replicated in similar settings worldwide to improve outcomes of neonatal respiratory distress and potentially decrease the burden of neonatal mortality that lies heavily in the developing world.
Supplemental Material
Supplemental_Page_1 – Supplemental material for Implementation of a Bubble CPAP Treatment Program for Sick Newborns in Nakuru, Kenya: A Quality Improvement Initiative
Supplemental material, Supplemental_Page_1 for Implementation of a Bubble CPAP Treatment Program for Sick Newborns in Nakuru, Kenya: A Quality Improvement Initiative by Nora Switchenko, Elizabeth Kibaru, Pamela Tsimbiri, Peter Grubb, Ann Anderson Berry and Bernhard Fassl in Global Pediatric Health
Supplemental Material
Supplemental_Page_2 – Supplemental material for Implementation of a Bubble CPAP Treatment Program for Sick Newborns in Nakuru, Kenya: A Quality Improvement Initiative
Supplemental material, Supplemental_Page_2 for Implementation of a Bubble CPAP Treatment Program for Sick Newborns in Nakuru, Kenya: A Quality Improvement Initiative by Nora Switchenko, Elizabeth Kibaru, Pamela Tsimbiri, Peter Grubb, Ann Anderson Berry and Bernhard Fassl in Global Pediatric Health
Footnotes
Acknowledgements
We would like to thank all of the nursing staff in the NBU at Nakuru County and Referral Hospital, in particular Helen Nafula and Mary Slessor, for their contributions to the bCPAP program.
Author Contributions
NS and EK were involved in the project design and implementation, data tracking, analysis, and manuscript preparation. PT, AAB, PG, and BF assisted with data analysis and manuscript revision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project received support from Rotary International Global Grant (#GG1862566).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.