
Abstract
Objective. To examine the postnatal predictors of survival and adverse outcome among Congenital Diaphragmatic Hernia (CDH) infants. Method. Six-year retrospective review of CDH infants born at tertiary neonatal unit. Results. Forty infants with CDH were included; 27 (67.5%) survived to discharge. Non-survivors had a higher best, mean, and highest oxygenation index (OI) (P < .001) on day 1 compared to survivors. Best (AUC = 0.917), mean (AUC = 0.945), and highest (AUC = 0.923) OI on day 1 were all predictive of mortality. The mean day-1 OI had a significant correlation with the duration of ventilation (DOV) (Spearman rho correlation coefficient (rS) = .549, P = .004), TTS (rS = .526, P = .007), and the length of hospital stay (LOS) (rS = .497, P = .012). The best and highest day-1 OI also correlated significantly with DOV, TTS, and LOS. Conclusion. First day OIs were excellent predictors of survival and have a significant correlation with the DOV, LOS, and TTS in infants with CDH.
Introduction
Congenital diaphragmatic hernia (CDH) is a common birth defect affecting 1:2500 to 4000 live births every year. 1 It continues to carry a high risk of mortality despite advances in antenatal diagnosis and fetal interventions designed to improve the degree of lung hypoplasia.2,3 Data from the CDH study group reported a 67% overall survival of CDH infants. 4 There are limited single data centers data on CDH survival outcomes in the Kingdom of Saudi Arabia.5-7
A variety of prenatal variables such as the presence of significant liver herniation8,9 and a lower lung-to-head ratio (LHR)8,10 have shown prognostic value. Postnatally, a variety of prediction scores have been developed, such as the score for neonatal acute physiology II (SNAP-II), the Wilford Hall/Santa Rosa predictive formula (WHSRpf), and the Congenital Diaphragmatic Hernia Study Group (CDHSG) equation.11-13 The size of the diaphragm defect has also been shown to have prognostic value. 14 More recently, the predictive value of oxygenation index (OI) has been reported in infants with CDH.15-19
The objective of this study was to examine the postnatal predictors of survival among CDH infants in a tertiary perinatal center in Saudi Arabia. We also examined the ability of the first day and pre-operative OIs in predicting the time to surgery (TTS) of the CDH, the durations of ventilation (DOV), and length of hospital stay (LOS) among CDH survivors.
Methods
This was a retrospective cohort of all cases of CDH born at single center Riyadh, Kingdom of Saudi Arabia over the 6-year period between October 1, 2016 and October 1, 2022. The study was approved by King Abdullah International Medical Research Centre (KAIMRC) ethics committee and waived the parental consent given the retrospective study design.
CDH cases were identified from the neonatal and feto-maternal databases at our institution. All cases with antenatal and postnatal diagnoses of CDH were included in the study, with no exclusions or selective terminations of CDH fetuses during the 6-year study period. It is important to note that no out-born infants with CDH were transferred to our center during the study period. Data extracted from the medical records included birth weight, gestational age at birth, gender, Apgar scores, mode of delivery, and maternal antenatal corticosteroids use. The side of the hernia and associated comorbidities were also determined. Antenatal ultrasound scans were used to determine the position of the liver where available. All fetuses with antenatal diagnosis of CDH underwent a detailed fetal echocardiogram to look for associated congenital heart disease (CHD).
Postnatally, CDH infants were managed according to the department guidelines, that is, infants were initially started on conventional ventilation with high frequency oscillatory ventilation (HFOV) as a rescue ventilation mode. Targets for pH, PCO2, preductal oxygen saturation, and PIP during conventional mechanical ventilation were based on the CDH EURO Consortium guidelines developed in 2010 and updated in 2015. 20 The ventilation strategy aimed to achieve preductal saturation between 85% and 95%, arterial PCO2 levels between 50 and 70 mmHg (permissive hypercapnia), pH > 7.2, and limiting peak pressure (PIP) to 25 cm H2O or less during conventional ventilation. 20 Inhaled nitric oxide (iNO) therapy was used if there was echocardiographic evidence of pulmonary hypertension.
All infants underwent a detailed echocardiogram within the first 24 to 48 hours to rule out CHD and to evaluate pulmonary hypertension. The echocardiographic features of pulmonary hypertension were a right ventricular systolic pressure ≥ 2/3 of the systemic systolic pressure as well as right ventricle (RV) dilatation/septal displacement or RV dysfunction ± left ventricle dysfunction. Inotropic support was commenced in infants with echocardiographic evidence of pulmonary hypertension. Surgical repair of the diaphragm defect was performed when the infant achieved cardiopulmonary stability. In our center, surgical repair of the defect was performed when infants’ clinical condition stabilized according to the following criteria: (1) blood pressure maintained at 40 to 50 mmHg with no more than 1 inotropic agent and (2) preductal oxygen saturation maintained between 85% and 95% on conventional mechanical ventilation with peak inspiratory pressure at 18 to 20 cm H2O and FiO2 less than or equal to 50%. Infants with CDH and associated critical congenital heart disease or major genetic abnormality were not offered surgical interventions, and palliative care pathways were deemed appropriate.
The best (ie, lowest), mean, and highest oxygenation indices on day 1 were calculated from the corresponding arterial blood gases. “The OI is a critical parameter used in the management of respiratory failure in newborns, particularly for assessing the severity of hypoxemic respiratory failure and guiding therapeutic decisions, such as the initiation of mechanical ventilation or extracorporeal membrane oxygenation (ECMO).” The OI was calculated using the following formula: (OI = mean airway pressure (MAP) × fraction of inspired oxygen (FiO2) × 100/partial pressure of oxygen in arterial blood (PaO2). The OI was calculated with every arterial blood gas obtained in the first 24 hours. The blood gases for infants in this study were all obtained from the umbilical arterial line. Therefore, all of the oxygenation indices reported here are postductal.
In addition, the first and highest arterial (PaCO2), highest arterial (PaO2) on day 1, and first arterial blood gas pH were noted. Those who underwent surgery had their pre-operative OI determined. The Wilford Hall Santa Rosa Prediction Formula (WHSRpf) was calculated based on previously published formula. 21 The WHSRpf is the difference between the best (PaO2) and (PaCO2) in the first 24 hours of life.
The DOV and TTS were recorded for the survivors. The type of hernia repair and the LOS were also noted. The CDH treatment protocol in our institution did not include extracorporeal membrane oxygenation (ECMO) or Fetoscopic Endoluminal Tracheal Occlusion (FETO). ECMO is not currently available in our center for infants with neonatal respiratory failure.
Statistical Analysis
Quantitative variables were expressed as medians (IQR) and qualitative variables as numbers and percentages. Comparison between survivors and non-survivors were performed using a Mann-Whitney test for quantitative variables and a Chi-square test for qualitative variables.
Receiver operating characteristic (ROC) analysis with associated area under the curve (AUC) evaluated the ability of OIs, PCO2, PaO2, pH and the WHSRpf on day 1 in predicting mortality with selection of the most suitable cut-off point of each parameter. The ROC analysis allowed us to visualize the trade-off between sensitivity and specificity across various threshold values. We selected the cut-off points that provided the highest combined sensitivity and specificity values, indicating the best possible predictive accuracy for each parameter. 22 Additionally, infants were stratified based on the need for rescue HFOV and the need for patch repair of the diaphragm defect in those who had surgery. Correlation between OIs and the (DOV), (TTS), and (LOS) were assessed using the Spearman Rho correlation coefficients (rS). Analysis used the Statistical Package of Social Science Software program (SPSS), version 25.
Results
Over a 6-year period, with 54 000 live births, there were 40 cases of CDH identified. This results in a prevalence rate of approximately 74.07 cases per 100 000 live births; 27 infants (67.5%) survived to hospital discharge, and 13 (32.5%) died. Four infants had additional complex conditions: 2 had congenital heart disease and 2 had chromosomal abnormalities. After excluding these 4 cases from the total, the corrected survival rate for CDH in our center during the study period is 75%. Left-sided CDH were the majority of cases (77.5%), and 80% of the cases were diagnosed antenatally (Table 1). Of the cases that did not survive, 2 had associated complex congenital heart disease, another 2 had associated chromosomal abnormalities, and for the remaining cases, mortality was caused by lung hypoplasia with associated pulmonary hypertension. It is worth noting that there were 3 prematurely born infants in our cohort of 40 infants. All of the mortalities in our study occurred prior to surgery for the diaphragmatic hernia and there was no post-operative mortality in our cohort of 40 infants.
Demographic Data (Numbers and Percentages) and Median Interquartile Range (IQR).

There were no statistically significant differences between survivors and non-survivors in terms of gestational age [38 (37.6-39) weeks vs 38 (37-39) weeks; P = .977], birth weight [2770 (2400-3120) g vs 2610 (2200-3000) g; P = .441], gender (P = 1.00), mode of delivery (P = .331), and antenatal diagnosis (P = 1.00). Apgar scores at 1 minute [5 (4-8) vs 3 (2-4); P = .007] and 5 minutes [8 (7-9) vs 6 (5-7); P = 004] were significantly higher among survivors. Pre-operative pneumothorax (18.5% vs 23.1%; P = .736) and pneumoperitoneum (7.4% vs 7.7; P = 1.000) did not differ between survivors and non-survivors. PPHN on echocardiogram (100% vs 66.7%; P = .019) was significantly higher among non-survivors. Need for HFOV (100% vs 59.3%; P = .007) and iNO (100% vs 70.4%; P = .037) were significantly higher among non-survivors. Need for inotropic support did not differ between survivors and non-survivors (81.5% vs 100%; P = .154). The number of infants with a WHSRpf > 0 was significantly higher among survivors (92.6% vs 30.8%; P < .001) (Table 2).
Antenatal and Postnatal Predictors of Survival.
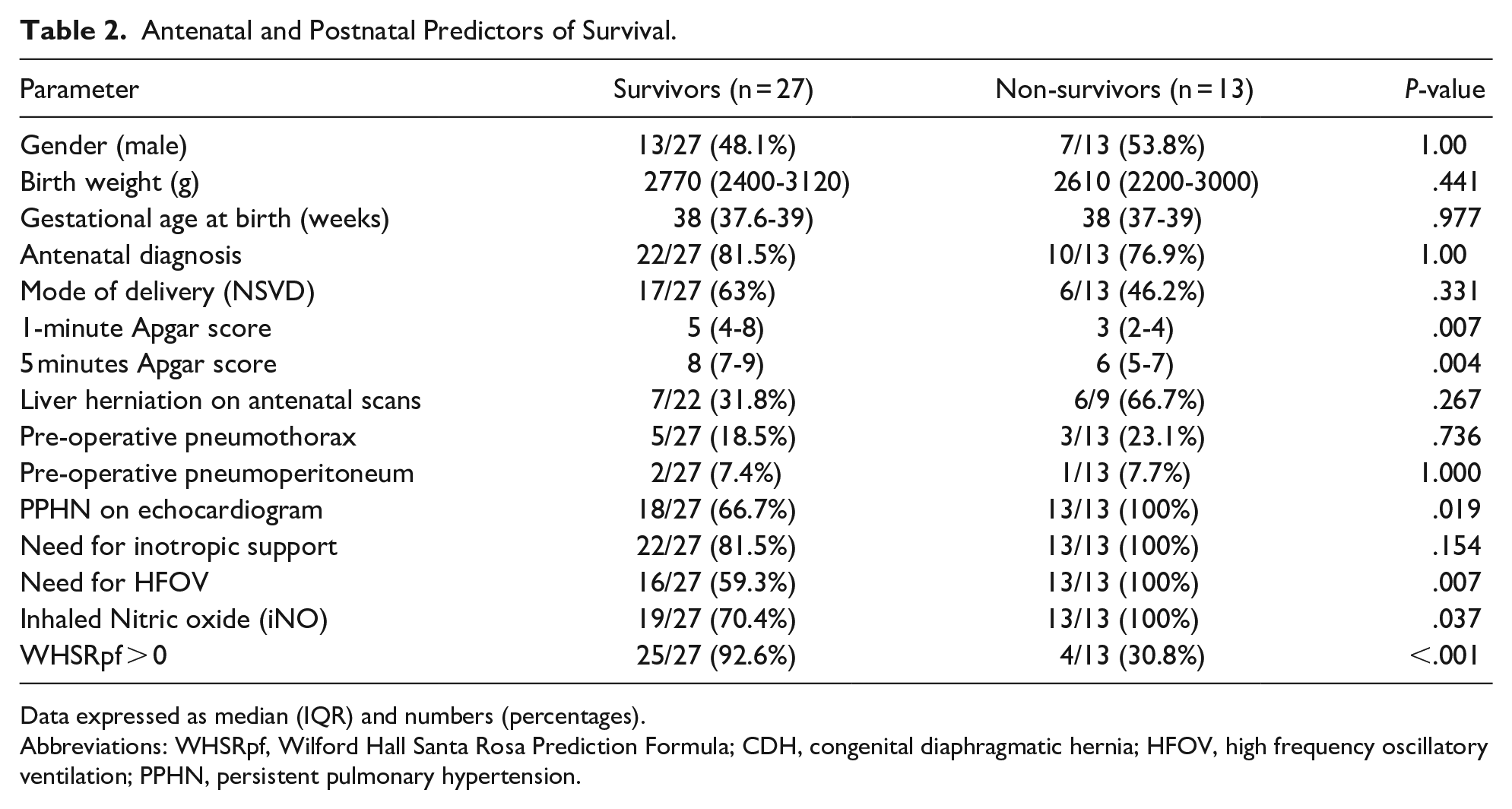
Data expressed as median (IQR) and numbers (percentages).
Abbreviations: WHSRpf, Wilford Hall Santa Rosa Prediction Formula; CDH, congenital diaphragmatic hernia; HFOV, high frequency oscillatory ventilation; PPHN, persistent pulmonary hypertension.
Non-survivors had a higher best [26.2 (22.1-37.6) vs 4.7 (2.9-8.9); P < .001], mean [43 (31.9-61.2) vs 11.1 (5.9-21.4); P < .001], and highest [62 (32.2-80.4) vs 17.2(9.6-29.2); P < .001] OI on day 1 compared to survivors. ROC analyses showed that best (AUC = 0.917; P < .0001), mean (AUC = 0.945; P < .0001), and highest (AUC = 0.920; P < .001) OI on day 1 and were all highly predictive of mortality (Table 3) (Figure 1). Examination of the coordinates of the ROC curves showed that a best OI on day 1 > 13 predicted mortality with 92% sensitivity and 84% specificity, a mean OI on day 1 > 25 predicted mortality with 94% sensitivity and 84% specificity, and a highest OI on day 1 > 30 predicted mortality with 92% sensitivity and 80% specificity (Figure 1). The first arterial blood gas PCO2 [73 (49-91) vs 50 (44-61); P = .029] and the highest arterial PCO2 on day 1 [88 (58-119) vs 59 (50-68); P = .014] were significantly higher among non-survivors.
Oxygenation and Ventilation Predictors of Survival-Data Presented as Median Interquartile Range (IQR).

Abbreviations: OI, oxygenation index; WHSRpf, Wilford Hall Santa Rosa Prediction Formula; AUROC, area under receiver operator characteristic curve.

ROC curve for prediction of hospital mortality by mean, best (lowest), and highest oxygenation indices on day 1.
ROC analysis showed that the first arterial blood PCO2 (AUC = 0.715; P = .029) and the highest arterial PCO2 on day 1 (AUC = 0.742; P = .014) were predictive of the mortality. A first arterial blood gas PCO2 > 52 predicted mortality with 70% sensitivity and 48% specificity whereas a highest day 1 arterial PCO2 > 60 predicted mortality with 76% sensitivity and 56% specificity. The first arterial blood gas pH [7.25 (7.14-7.32) vs 7.06 (6.91-7.30); P = .033] and a highest day 1 PaO2 [115 (87-192) vs 60 (52.5-83.0; P = .006] were significantly higher among survivors. ROC analysis also showed that the highest day 1 PaO2 (AUC = 0.771; P = .006) and the first arterial blood gas pH (AUC = 0.711; P = .033) were both predictive of survival. A highest day 1 PaO2 < 83 predicted mortality with 78% sensitivity and 77% specificity whereas a first arterial pH < 7.12 predicted mortality with 71% sensitivity and 61% specificity. Furthermore, the (WHSRpf) was highly predictive of mortality (AUC = 0.838; P = .001). A WHSRpf score < 16 predicted mortality with 84% sensitivity and 85% specificity (Table 3).
There were 32 cases with antenatal diagnosis of CDH and a further 8 cases were the CDH was diagnosed postnatally. Gestational age was 37.8 weeks for antenatal versus 38.9 weeks for postnatal (P = .241), and birthweight was 2677 g versus 2721 g (P = .811). Survival rates were 68.8% for antenatal and 62.5% for postnatal (P = .736). OI measures, PCO2 levels, and WHSRpf scores were also similar across both groups with no statistically significant differences (Table 4).
Comparison of Clinical and Biochemical Measures of Stability Between Antenatally and Postnatally Diagnosed CDH.
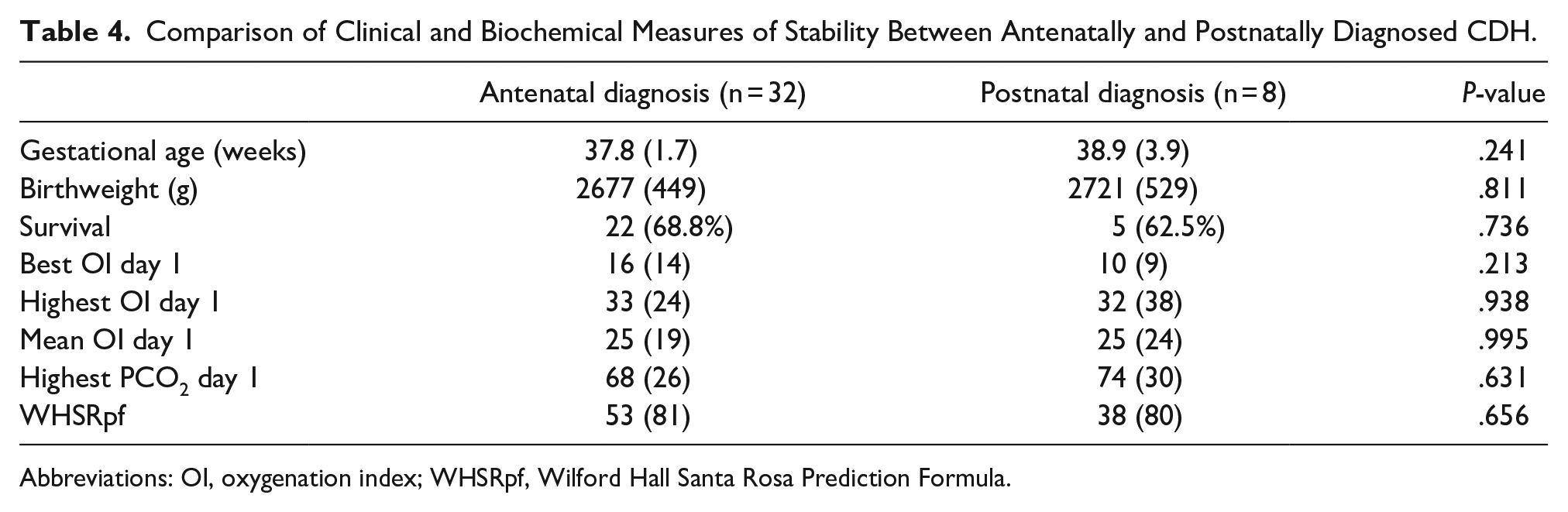
Abbreviations: OI, oxygenation index; WHSRpf, Wilford Hall Santa Rosa Prediction Formula.
Twenty-nine infants needed rescue HFOV. There were statistically significant differences between those who needed rescue HFOV and those who did not in the mean (P = .001), best (P = .043), and highest (P ≤ .001) day-1 OI. The mean (AUC = 0.875, P = .001), best (AUC = 0.752, P = .043), and highest (AUC = 0.92, P < .001) day-1 OI were all predictive of the need for rescue HFOV (Table 5).
OI of CDH Infants Based on the Need for Rescue HFOV.

Data presented as median (IQR).
Abbreviations: OI, oxygenation index; HFOV, high frequency oscillatory ventilation; AUROC, area under receiver operator characteristic curve.
Twenty-seven infants underwent surgical repair of the diaphragm defect of whom 14 infants needed patch repair of the defect. There were no statistically significant differences in the mean (P = .166), best (P = .202), and highest (P = .222) day-1 OI between those who had patch repair of the diaphragm defect and those who had primary repair (Table 6).
Oxygenation Indices of CDH Infants Based the Type of Surgical Repair.
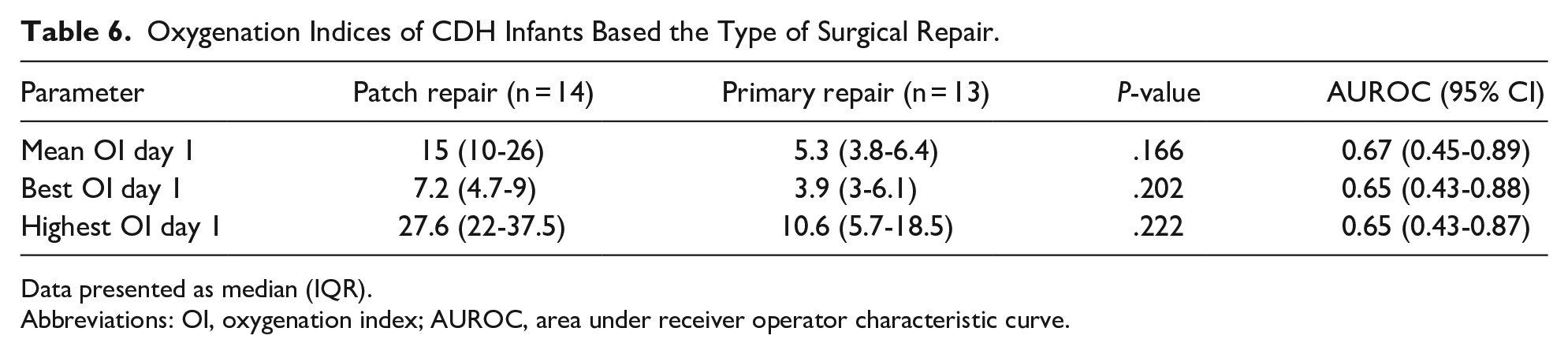
Data presented as median (IQR).
Abbreviations: OI, oxygenation index; AUROC, area under receiver operator characteristic curve.
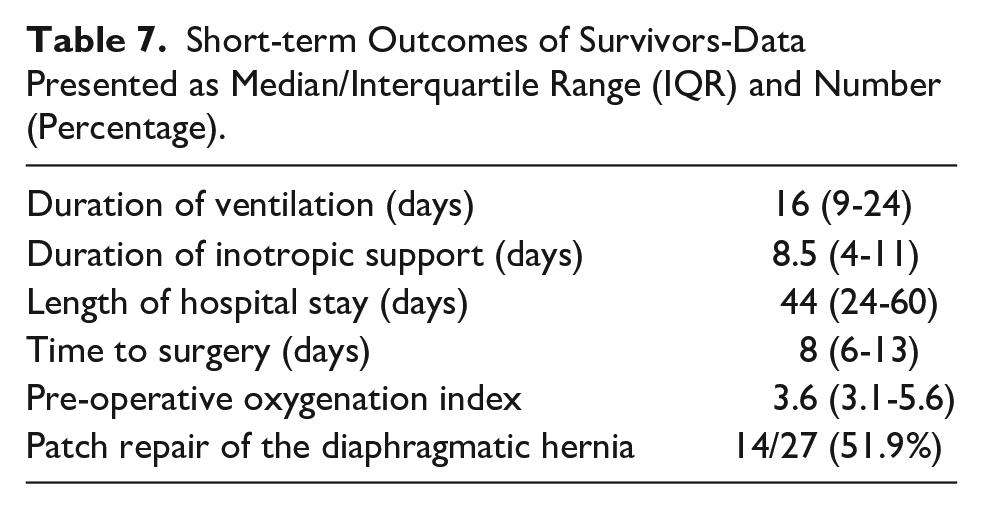
Twenty-seven (67.5%) infants had surgical repair of the CDH at a median (IQR) age of 8 (6-13) days and prosthetic patch was used in 14 (51.9%). Their median (IQR) DOV was 16 (9-24) days, and the median (IQR) LOS was 44 (24-60) days (Table 7).
Short-term Outcomes of Survivors-Data Presented as Median/Interquartile Range (IQR) and Number (Percentage).
There was a significant correlation between the preoperative OI and the TTS (rS = .462; P = .017) as well as the LOS (rS = .458; P = .019). Furthermore, the mean day-1 OI had a significant correlation with the DOV (rS = .549; P = .004), TTS (rS = .526; P = .007), and the LOS (rS = .510; P = .010). Similarly, the best day-1 OI had a significant correlation with the DOV (rS = .580; P = .002), the TTS (rS = .509; P = .009), and the LOS (rS = .490; P = .013). Finally, the highest OI on day 1 had a significant correlation with the DOV (rS = .585; P = .002) and the TTS (rS = .440; P = .028) (Table 8).
Correlations of the Oxygenation Indices (best, Mean, Max Day 1 and Pre op) With DOV, TTS, and LOS.
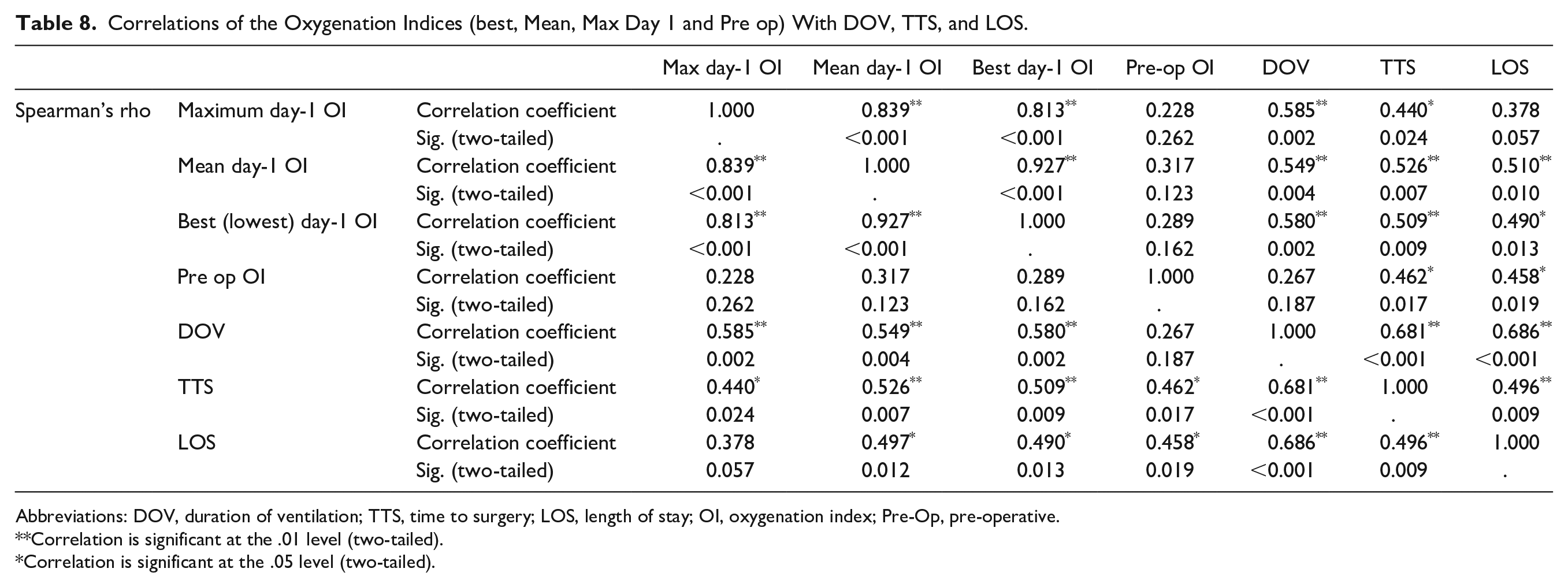
Abbreviations: DOV, duration of ventilation; TTS, time to surgery; LOS, length of stay; OI, oxygenation index; Pre-Op, pre-operative.
Correlation is significant at the .01 level (two-tailed).
Correlation is significant at the .05 level (two-tailed).
Discussion
The study demonstrated a survival rate of 67.5% among CDH infants managed without ECMO at our institution. We included all fetuses with in-utero and postnatal CDH diagnosis born at our institution over the 6-year study period with no exclusions or selective terminations during the study period. Previous single-center studies from the Kingdom of Saudi Arabia showed variable survival rates in CDH infants ranging from 71.4% 5 to 57%. 6 A recent single-center study on (CDH) survival rates in the Kingdom of Saudi Arabia over a 21-year period reported a survival rate of 48%, which is notably lower compared to other CDH survival rates reported in the Kingdom. However, the extended study duration likely encompassed significant changes in CDH management practices, which could have influenced the CDH survival outcome reported in that study. 7 Our survival rate is comparable to that reported from the CDH Study Group (67%). 4 A multicentre European study involving 975 infants born between 2004 and 2013 reported an overall CDH survival of 71.9%, a 68.7% survival for the group of CDH infants who underwent ECMO, and a lower survival at 52.4% for a subgroup of CDH infants who had (FETO). 23
In our series, 32 infants (80%) were antenatally diagnosed, and the rates of antenatal diagnosis did not differ between survivors and non-survivors. Antenatal diagnosis offers the advantages of a planned delivery at a tertiary center with availability of expertise dealing with CDH cases. Nevertheless, antenatal diagnosis might imply a longer duration of abdominal visceral herniation into the thoracic cage, thus resulting in an increased degree of lung hypoplasia. 24 Therefore, some studies have reported a significantly higher mortality in antenatally-diagnosed patients versus those diagnosed postnatally.24,25 Postnatally-diagnosed infants with CDH in our study were managed with the same protocol as prenatally-diagnosed cases. There may have been some variation in the initial stabilization in the postnatally-diagnosed cases. However, postnatally-diagnosed CDH infants were managed with the same protocol as prenatally-diagnosed cases from the time of admission to intensive care. There were no out born infants with CDH in our study.
We have shown that the Apgar scores at 1 minute and 5 minutes after birth were significantly lower among CDH non-survivors. This is consistent with other previous studies showing a lower 5-minute Apgar score among CDH non-survivors.13,26 Indeed, the Apgar score is an indicator of early cardiopulmonary adaptation and response to resuscitation. Nevertheless, others have found no differences in the Apgar scores between CDH survivors and non-survivors. 27 Both the need for iNO therapy and HFOV were significantly higher among CDH non-survivors in our cohort. This is similar to the findings from the largest observational study on the resuscitation of CDH infants that showed a higher use of HFOV and iNO therapy among CDH non-survivors. 27
We also found that the echocardiographic findings of PPHN were significantly more concerning among CDH non-survivors. Indeed, pulmonary hypertension is a major determinant of postnatal survival in infants with a CDH. The pulmonary hypertension treatment in our patients varied considerably and included a combination of different vasopressors, milrinone, and iNO therapy. Indeed, optimal treatment for pulmonary hypertension in infants with CDH is still unclear. We await the results of ongoing randomized control trials looking at the best initial therapy for pulmonary hypertension in infants with CDH.28,29 The first and highest PCO2 recorded on day 1 (<60 mmHg) were within the range that would be acceptable for a permissive hypercapnia strategy. Nevertheless, rates of preoperative pneumothorax in our study were relatively high, but this unlikely to be related to the ventilatory strategy used in infants included in the study and is likely a reflection of the severity of the lung disease secondary to the diaphragmatic hernia. All CDH infants included in this study had a functioning nasogastric tube. The occurrence of pneumoperitoneum in our study occurred in association with pneumothorax. Therefore, it is likely that the air leak started in the chest and extended to the peritoneum through the diaphragm defect.
This study showed that the best (lowest), mean, and highest oxygenation indices on day 1 were all excellent predictors of survival: The mean day-1 OI marginally outperformed the other 2 indices with higher sensitivity and specificity. The mean day-1 OI is likely to be more reflective of the overall first day cardiopulmonary stability versus the lowest and highest day OI because these indices may vary in response to alternations in the clinical condition and the ventilatory support changes. Indeed, the excellent survival predictive ability of the best day-1 OI has been described in the literature.16-18,30 We also demonstrated that the WHSRpf (highest PaO2—highest PaCO2) 21 is predictive of CDH survival. Nevertheless, the predictive ability of the formula is lower than that of day-1 OI as seen in AUC analysis. We have also shown that the first arterial PCO2, the highest arterial PCO2, the PaO2 on day 1, as well as the first arterial blood gas pH were all predictive of survival—albeit with lower predictive ability versus the OIs and the WHSRpf. Others have shown that the maximum PCO2 in the first 24 hours after birth is a useful predictor of survival in CDH infants. 15 We also demonstrated that the first-day OI are predictive of the need for need for rescue HFOV among CDH infants but not of the need for patch repair of the diaphragm defect.
We have shown that the pre-operative OI had a significant correlation with the TTS of the hernia as well as LOS. Tan et al 30 also showed that pre-operative OI did show significant correlations with TTS, LOS, and DOV. 30 In addition to the predictive ability of the first day oxygenation indices for CDH survival and need for rescue HFOV, we also showed that they have a significant correlation with the TTS, DOV, and LOS. To the best of our knowledge, the correlation of the first-day OI with DOV, LOS, and TTS have not yet been described. This finding therefore adds to the usefulness of first day OIs as a predictor of both CDH survival and adverse outcomes among survivors. A preprint of the study was previously published in research square (https://doi.org/10.21203/rs.3.rs-2322559/v1). 29
This study has both strengths and limitations. We report data on consecutive infants with CDH with no exclusions. We also obtained a full set of oxygenation indices from our electronic patients records that combine the ventilatory settings and the corresponding blood gases results used to calculate the OI values. Limitations include a lack of data for the LHR and CDHSG defect size. Unfortunately, LHR was not recorded systematically at our center until 2022. Nevertheless, we have 2 stratification strategies including the use of rescue HFOV in all CDH infants in the study as well as the need for patch repair of the diaphragm defect in those who had surgery. Our study did not employ a pre-determined sample size calculation, as it was retrospective in nature, including all infants diagnosed with Congenital Diaphragmatic Hernia (CDH) born within the specified 6-year study period. This approach ensured comprehensive data capture but may limit the generalizability of our findings. The inability to calculate and justify a sample size based on statistical power considerations before the study commenced is a limitation, as it might affect the representativeness and the extrapolation of the results to other populations. Future prospective studies could benefit from predetermined sample size calculations to enhance the statistical power and applicability of the findings.
Conclusion
We have shown that our CDH survival rates without ECMO and antenatal interventions are excellent and are comparable to data from international studies. We also demonstrated that the first-day OI including the best (lowest), mean, and highest OI were excellent predictors of survival in CDH infants. Finally, we showed that the first-day OIs—together with the preoperative OI—have significant correlation with other adverse outcomes including the DOV, LOS, and TTS among CDH survivors. Our study stands out because it specifically examines oxygenation indices (OIs) and related parameters in a Saudi Arabian context, contributing localized insights to the existing global literature on CDH. We have provided cut-off values for different oxygenation indices in the first 24 hours (mean, best, and highest) to predict survival and other adverse outcomes such as the need for rescue high-frequency oscillatory ventilation (HFOV) and patch repair of the diaphragm, which serves as a surrogate marker for the size of the diaphragmatic defect. We found that the optimal OI cut-off for predicting survival in our cohort aligns closely with findings from international studies. This provides a relevant benchmark for other centers in Saudi Arabia and similar regions to follow, allowing for standardized assessment and management of CDH based on local clinical data.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241263760 – Supplemental material for Congenital Diaphragmatic Hernia, Predictors of Survival and Adverse Outcomes
Supplemental material, sj-docx-1-gph-10.1177_2333794X241263760 for Congenital Diaphragmatic Hernia, Predictors of Survival and Adverse Outcomes by Kamal Ali, Nemer Aljuaid, Saleh S. Algarni, Abadi Ghazwani, Saad Alshreedah, Nawaf Alghamdi, Mohamad Alreefi, Abdurhman Alsaif, Naif Alotaibi, Wejdan Alzahrani and Saif Alsaif in Global Pediatric Health
Footnotes
Acknowledgements
Authors’ Note
Kamal Ali also affiliated to King Saud bin Abdulaziz University for Health Sciences, Riyadh, Kingdom of Saudi Arabia.
Author Contributions
Kamal Ali, Nemer Aljuaid, Saleh S Alqarni and Saif Alsaif designed the study and analyzed the data. Nawaf Alghamdi, Mohammad Alreefi, Abadi Ghazwani, Abdurhman Alsaif, Naif Alotaibi, Wejdan Alzahrani and Saad Alshreedah collected the data. All of the authors made a significant contribution to writing of the manuscript.
Availability of Data
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: King Abdullah International Medical Research Centre (KAIMRC) approved the project with IRB number: NRC21R/229/06. Funding for this publication is provided by King Abdullah International Medical Research Center (KAIMRC).
Ethical Standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Details of Ethical Approval
King Abdullah International Medical Research Centre (KAIMRC) ethics committee approved the project with IRB number: NRC21R/229/06. Requirement for informed consent was waived by King Abdullah International Medical Research Center (KAIMRC) ethics committee due to the retrospective nature of the study.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.