
Abstract
Introduction. Severe community acquired pneumonia (CAP) is a life-threatening condition, with high rates of morbidity and mortality. This study aimed to determine the recovery time from severe CAP and risk factors among pediatric patients. Methods. A retrospective follow-up study was conducted among 412 pediatric medical charts with severe CAP enrolled at Asella Referral and Teaching Hospital between January 01, 2021 and December 31, 2022. EpiData version 4.6.0.6 and STATA version 14.2 were used for data entry and statistical analysis, respectively. Bivariable and multivariable Cox proportional hazards regression analyzes were performed. Result. The median recovery time from severe CAP among pediatric patients was 5 days (IQR = 3-8 days). IDR of recovery from severe CAP was 13.089 per 100 [95%CI: 11.82, 14.49] pediatric days observations. The cumulative incidence of recovery from severe CAP was 89.56% [n = 369, 95%CI: 86.20, 92.18]. Age [AHR = 1.55, 95%CI: 1.12, 2.13, P = .007], vaccination status [AHR = 1.29, 95%CI: 1.03, 1.63, P = .027], presence of danger signs [AHR = 1.61, 95%CI: 1.26, 2.05, P = .000], presence of comorbidity [AHR = 1.67, 95%CI: 1.33, 2.10, P = .000], duration of seeking care [AHR = 1.71, 95%CI: 1.18, 2.47, P = .004], and oxygen therapy [AHR = 1.45, 95%CI:1.12, 1.87, P = .004] were statistically significant risk factors for recovery time from severe CAP. Conclusions. The median recovery time of patients with severe CAP is relatively high. Age, vaccination status, presence of danger signs, presence of comorbidities, duration of seeking care, and oxygen therapy were statistically significant risk factors of recovery time from severe CAP.
Keywords
Introduction
Pneumonia is a major killer of children in developing countries and leads to substantial globally.1,2 Pneumonia is one of the most critical diseases affecting children. 3 It is one of the leading causes of mortality among children under 5 years of age. In developing countries, the incidence is estimated to be 0.29 episodes per child-year, while 0.05 episodes per child-year in developed countries. Globally, approximately 156 million new episodes are estimated each year, of which 151 million are in developing countries. 4 According to the World Health Organization report of 2022, approximately 14% of all deaths in children under 5 years of age were due to pneumonia. In 2019, it killed approximately 740,180 children in 2019. 5
CAP is defined as the presence of signs and symptoms of pneumonia due to an infection acquired outside the hospital in a previously healthy child. 6 CAP leads to high mortality among individuals admitted to the public intensive care unit. 7 Approximately 22% of patients with CAP need admission to intensive care units. Approximately 44% to 83% of patients require mechanical ventilation, while 50% present with associated septic shock. 8 Globally, CAP is the leading cause of death among children under 5 years of age. It is a common infectious disease in children and is associated with high use of antibiotic and hospitalization, even in industrialized countries. 9 CAP is one of the major global health problems globally. 10
Severe CAP is the most lethal form of CAP and is characterized by admission to the intensive care unit and high morbidity and mortality. 11 Severe CAP is a life-threatening disease characterized by respiratory failure or unknown “symptoms of severe sepsis” or “septic shock.” Severe CAP accounts for approximately 10% of hospitalized patients with CAP. 12 Due to the severe complications of severe CAP, some children hospitalized for severe CAP require admission to the pediatric intensive care unit. 13 Severe CAP continues to contribute to pediatric morbidity, requires invasive investigations and treatment and prolongs hospitalization, even though severe CAP has become less frequent since the introduction of the widespread use of effective antibiotics early during infection and the probability of preventing CAP using vaccines. 14
Despite intensive studies, diagnosis, and treatment of pneumonia, the related burden is still ongoing. 3 Furthermore, pneumonia remains the leading cause of mortality in children under 5 years of age, despite the availability of vaccines and antibiotics. 15
Severe CAP remains a common cause of critical care admission and is associated with high mortality, despite improvements in supportive care. 16 Proper management of pneumonia requires careful understanding of its epidemiology, pathophysiology, and pharmacology. 17 Appropriate initial antibiotic selection is essential for patients with severe CAP outside the intensive care unit to improve their outcomes. 18 This is because early initiation of appropriate antibiotics is the key element in reducing adverse outcomes in individuals with SCAP. 19
The pooled prevalence of pneumonia in Ethiopia under 5 children was 20.68%. 20 Severe pneumonia among children under 5 years of age accounts for 16.09% of mortality in Ethiopia. 21 The magnitude of the poor outcomes of severe CAP such that “if treatment failure or antibiotic change or staying longer in the hospital or death occurred during follow-up days” was 28% in Ethiopia. 22
Despite the significant burden of severe CAP among pediatric patients, there are limitations to studies that have addressed the recovery time from severe CAP and risk factors in pediatrics in the study area and worldwide. However, understanding the recovery time from severe CAP and its predictors is vital information that needs to be incorporated into the management of severe CAP among pediatric patients. Therefore, the present study aimed to determine the recovery time from severe CAP and risk factors among pediatric patients admitted to the Asella Referral and Teaching Hospital, Oromia Regional State, Ethiopia.
Methods
Study Area and Period
The present study was conducted at Asella Referral and Teaching Hospital, located in Asella Town. Asella town is located in the Arsi zone of the Oromia Regional State. It is located in central Ethiopia,126 km south of Addis Ababa. 23 The present study was conducted between March 12 and March 22, 2023.
Study Design
A retrospective follow-up study was conducted.
Source Population
The source population comprised all children admitted with severe CAP between January 01, 2021 and December 31, 2022.
Study Population
All children who were admitted to the hospital with severe CAP and their charts were available during the data collection period.
Eligibility Criteria
Inclusion criteria
All children ≤15 years of age admitted to the pediatric ward with severe CAP were included in the study.
Exclusion criteria
Children with incomplete medical records for date of admission and date of discharge were excluded from the present study.
Sample Size Determination
For the present study, a complete survey or census method was conducted. All children admitted with severe CAP between January 01, 2021 and December 31, 2022 were included in the present study. The final sample size was 448.
Sampling Technique and Procedure
The medical registration charts of all children admitted with severe CAP between January 01, 2021 and December 31, 2022 were checked. Subsequently, all necessary information was extracted from the medical charts of the children based on the data extraction format prepared for the present study.
Variables
Dependent variable
Recovery time from severe CAP
Independent variables
Operational definitions
Data Collection Tool, Procedure, and Quality Control
The data extraction format was adapted from a previous study. 24 The data extraction format was prepared in English. The format consists of 2 parts. Sociodemographic characteristics of the children and clinical related characteristics of children. Data were extracted by 2 nurses. Half-day training was provided to data extractors on the data extraction format and procedure. The completeness of the extracted data was checked daily during data extraction. They were supervised by a Master of Science degree-qualified instructor.
Statistical Analysis
EpiData version 4.6.0.6 was used for data entry. Statistical analyzes were performed using STATA Version 14.2. The time variable was determined by subtracting the beginning date from the end date, and the unit was “days.” The recovery time was determined using days as the time scale. The median recovery or survival times were determined and explained using the interquartile range (IQR). The rule of thumb applied to the variance inflation factor was used to determine the multicollinearity between the predictors; there was no sign of multicollinearity. Incidence density rate (IDR) and cumulative incidence were calculated in addition to the median recovery time. Kaplan-Meier survival estimation was performed to determine the probability of survival. Kaplan-Meier survival curve and log-rank tests were performed to test for equality of survival functions among the different categorical predictors. Schoenfeld residuals and scaled Schoenfeld residuals were used to check and test the Cox proportional hazards assumption, which is a goodness-of-fit test.
Predictors with a global test of P > .05, were considered to meet the Cox proportional hazard model assumption. The Cox-Snell residual was used to determine the overall fit of the model. Bivariable and multivariable Cox proportional hazards regression analyzes were performed. Bivariable Cox proportional hazard regression analysis and predictors with a P < 0.25 were considered for multivariable Cox proportional hazard regression analysis. The results were explained using the crude hazard ratio (CHR) and the adjusted hazard ratio (AHR) with 95% confidence intervals (CI). The statistical significance of the multivariable Cox proportional hazard regression analysis was declared at a P < .05. The results of the present study are presented using narration, tables, and figures.
Result
Sociodemographic Characteristics of Children
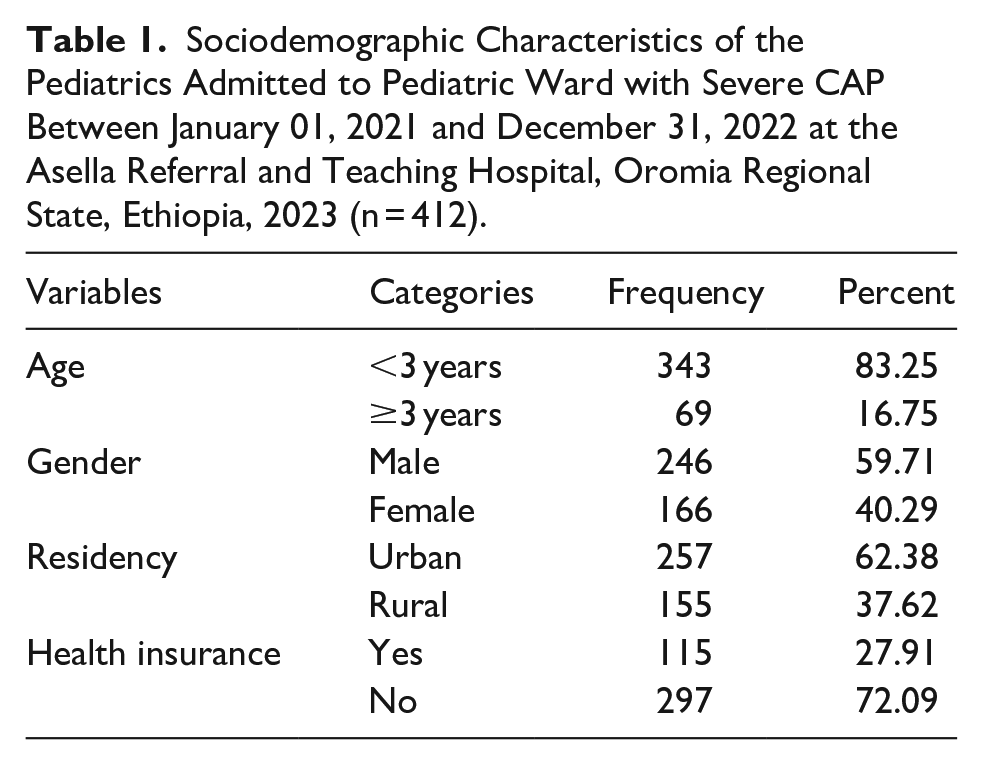
Of the 448 medical records of children, only 412 were included in the present study for analysis. The remaining patients were excluded from the analysis due to incomplete information. This resulted in a response rate of 91.96%. The majority 343(83.25%) of children included in the study were <3 years. Approximately 257(62.38%) of the children were urban residents (Table 1).
Sociodemographic Characteristics of the Pediatrics Admitted to Pediatric Ward with Severe CAP Between January 01, 2021 and December 31, 2022 at the Asella Referral and Teaching Hospital, Oromia Regional State, Ethiopia, 2023 (n = 412).
Clinical Related Characteristics of Pediatrics
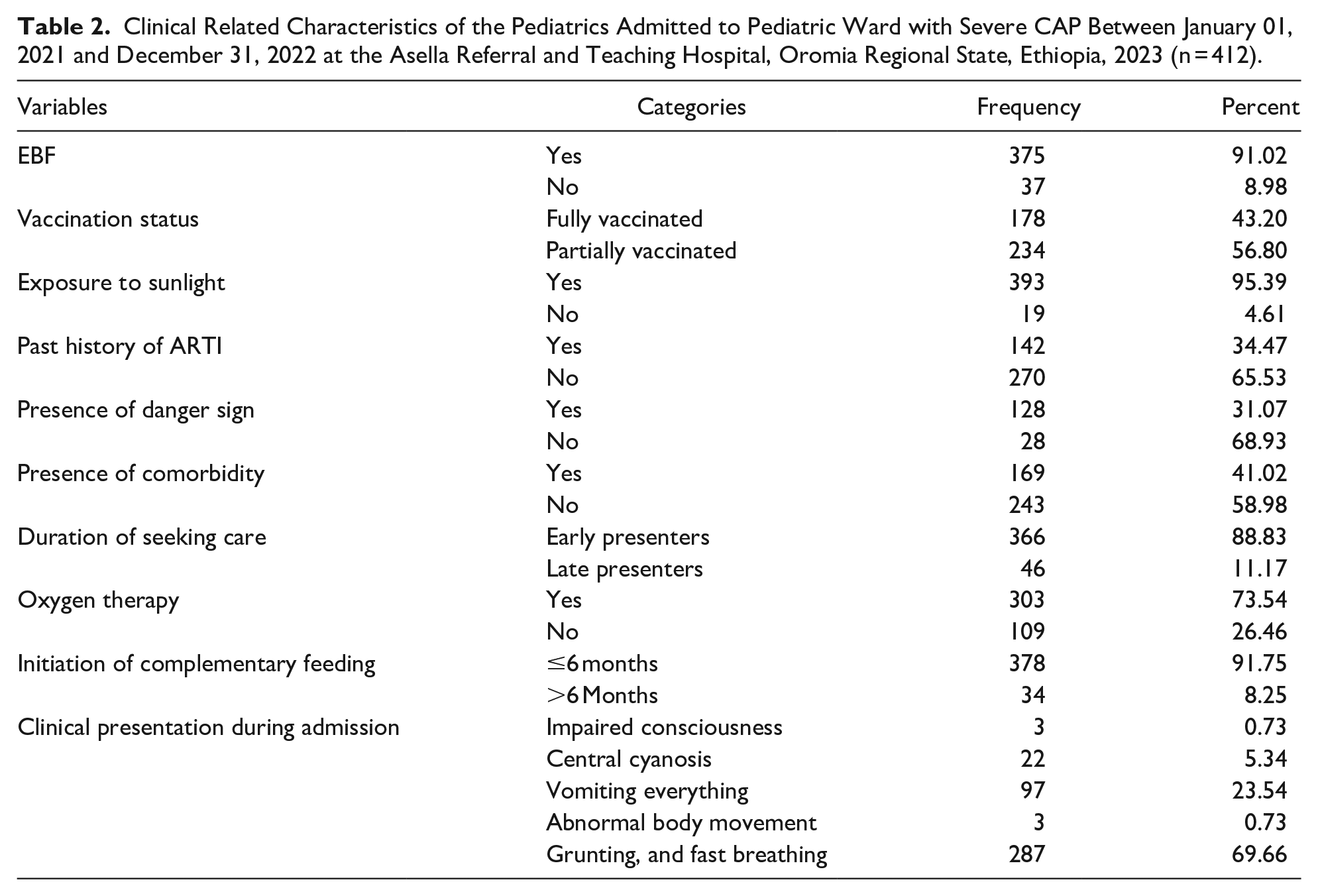
Of the children included in the present study, 178 (43.20%) were fully vaccinated. Approximately 142 (34.47%) of the children had a history of ARTI. The majority 128 (31.07%) of the admitted children had signs of danger during admission. About 169 (41.02%) of the children were diagnosed with comorbidities. The majority 366 (88.83) of the children were early presenters for seeking care (Table 2).
Clinical Related Characteristics of the Pediatrics Admitted to Pediatric Ward with Severe CAP Between January 01, 2021 and December 31, 2022 at the Asella Referral and Teaching Hospital, Oromia Regional State, Ethiopia, 2023 (n = 412).
Survival Status of Pediatrics
The IDR of recovery from severe CAP was 13.089 per 100 [95%CI: 11.82, 14.49] pediatric day observations. The total person-time risk was 2819. The cumulative incidence of recovery from severe CAP was 89.56% [n = 369, 95%CI: 86.20, 92.18]. Of the 412 pediatric patients included, 43 (10.44%) subjects were censored. Of these, 31 (72.01%) were lost to follow-up, 4 (9.30%) were referred, 1 (2.33%) was transferred, and 7 (16.28) died before recovering from severe CAP.
Recovery Time From Severe CAP
The median time to recovery from severe CAP among pediatric patients admitted with severe CAP at Asella Referral and Teaching Hospital was 5 days (IQR = 3-8 days).
Recovery Time From Severe CAP Among Different Predictors
The log-rank test was performed to check for equality of survival time in the different groups. The log-rank test results for age were X2 = 4.87, df = 1, and P = .027. This indicates that there was a statistically significant difference in the survival time between children aged <3 years and those aged ≥3 years. The log-rank test results for residency were; X2 = 5.96, df = 1, and P = .014. This indicates that there was a statistically significant difference in survival time between urban and rural children.
The log-rank test results for EBF were X2 = 4.5, df = 1, and P = .033. This indicates that there was a statistically significant difference in the survival time between who were EBF and not. The log-rank test results for history of ARTI were; X2 = 9.14, df = 1, and P = .002. This indicated that there was a statistically significant difference in survival time between patients with a history of ARTI and those who did not.
The log-rank test results for history of danger signs were; X2 = 24.73, df = 1, and P = .000. This indicates that there was a statistically significant difference in the survival time between those who had danger signs on admission and those who did not. The log-rank test results for presence of comorbidities were; X2 = 40.92, df = 1, and P = .000. This indicated that there was a statistically significant difference in survival time between patients with comorbidities and those who did not.
The log-rank test results for duration of seeking care were; X2 = 23.14, df = 1, and P = .000. This indicates that there was a statistically significant difference in the survival time between the early and late presenters. The log-rank test results for oxygen therapy were; X2 = 32.20, df = 1, and P = .000. This indicated that there was a statistically significant difference in survival time between patients who received oxygen therapy and those who did not (Table 3).
Comparison of Survival Time by Different Predictors Among Pediatrics Admitted with Severe CAP Between January 01, 2021 and December 31, 2022 at the Asella Referral and Teaching Hospital, Oromia Regional State, Ethiopia, 2023 (n = 412).

The bold p-value indicates statistically significant level.
Overall Survival Function of Admitted Pediatrics
The Kaplan-Meier survival estimates showed that the estimated survival function for recovery from severe CAP in pediatric patients was 95.87% (95%CI: 93.45%, 97.41%), 17.55% (95%CI: 13.84, 21.63%), 5.95% (95%CI: 3.74, 8.88), 1.21% (00.35, 3.19), and 0.81% (95%CI: 0.17, 2.63) at the 1st, 10th, 20th, 40th, and 60th day follow-up periods, respectively. The majority (318) of the children recovered from severe CAP within the first 10 days. This was evidenced by the rapid decrease in the Kaplan-Meier curve in the first 10 days (Figure 1).

Kaplan Meier survivals function in pediatric admitted with severe CAP between January 01, 2021 and December 31, 2022 at the Asella Referral and Teaching Hospital, Oromia Regional State, Ethiopia, 2023 (n = 412).
Testing Overall Model Fit
The Nelson-Aalen estimator was used to determine the fitness of the model using Cox-Snell residuals. If the plot of the cumulative hazard versus (cs) approximates a straight line with slope 1, it is a sign of fitness of the model. The residuals should have a standard censored exponential distribution with hazard ratio to ensure that the Cox regression model fits the data. The hazard function closely followed the 45° line when the jagged line was compared to the reference line. Therefore, the Cox-Snell residuals satisfied the overall fitness (Figure 2).

Cox-Snell residual Nelson-Aalen cumulative hazard graph in pediatric admitted with severe CAP between January 01, 2021 and December 31, 2022 at the Asella Referral and Teaching Hospital, Oromia Regional State, Ethiopia, 2023 (n = 412).
Risk Factors of Recovery Time From Severe CAP
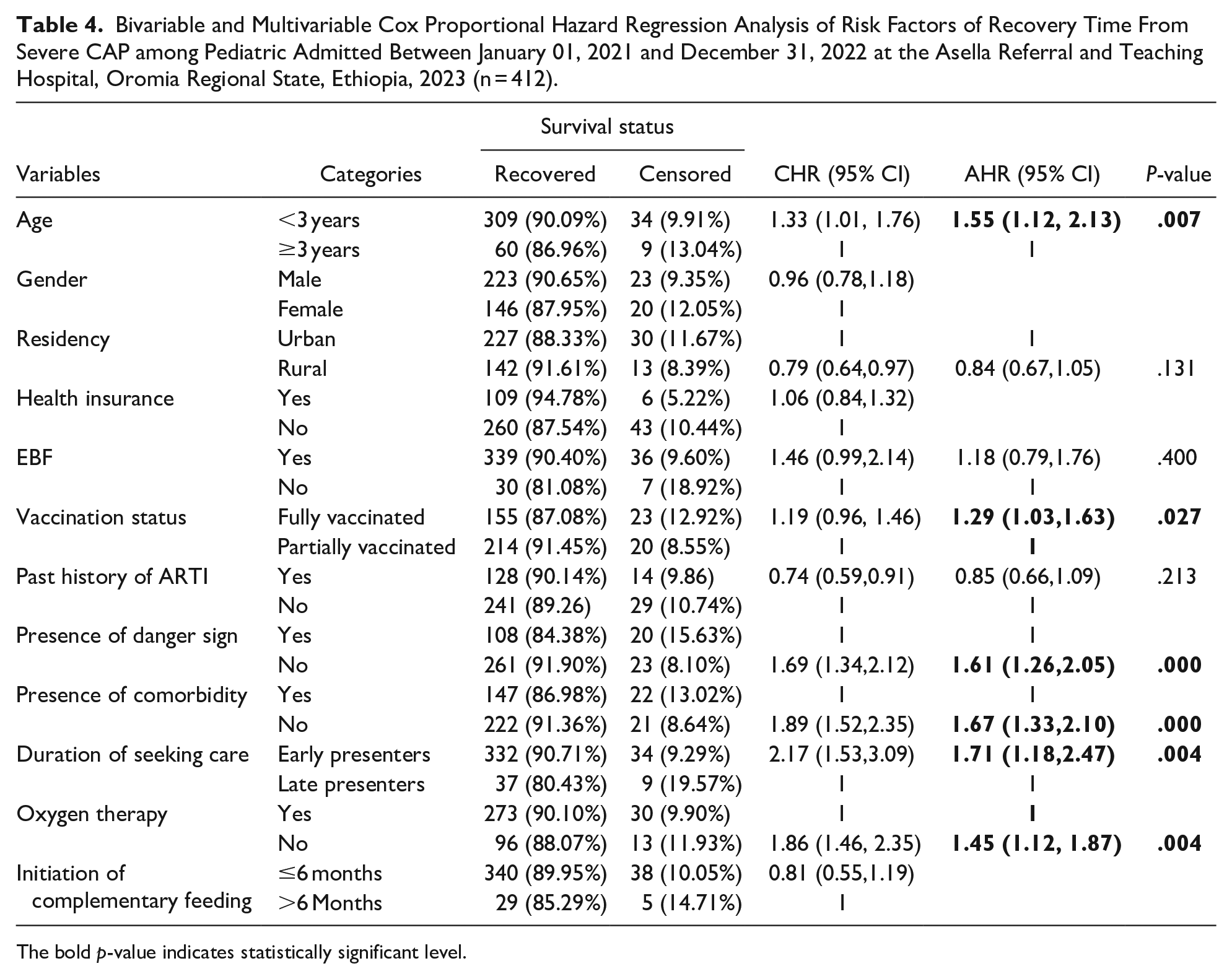
Age, sex, residence, health insurance, EBF, vaccination status, history of ARTI, presence of danger signs, presence of comorbidity, duration of seeking care, oxygen therapy, and initiation of complementary feeding were factors included in the bivariate Cox proportional hazard regression to check for their association with the recovery time from severe CAP among pediatric patients. However, considering the screening criteria P < 0.25 to include the predictor in the multivariable Cox proportional hazard regression, age, residency, EBF, vaccination status, history of ARTI, presence of danger signs, presence of comorbidity, duration of seeking care, and presence of oxygen were entered into the multivariable Cox proportional hazard regression. Finally, age, vaccination status, presence of danger signs, presence of comorbidity, duration of seeking care, and oxygen therapy were statistically significant risk factors for recovery time from severe CAP.
The hazard ratio of recovery from severe CAP in pediatric patients aged <3 years was 1.55 hazard [AHR = 1.55, 95%CI: 1.12, 2.13, P = .007] more likely than in children ≥3 years. The hazard ratio of recovery from severe CAP in pediatric patients who were fully vaccinated was 1.29 hazard [AHR = 1.29, 95%CI: 1.03, 1.63, P = .027] more likely than that in pediatric patients who were partially vaccinated.
The hazard ratio of recovery from severe CAP in pediatric patients who had no danger signs on admission was 1.61 hazard [AHR = 1.61, 95%CI: 1.26, 2.05, P = .000] more likely than pediatric patients who had danger signs on admission. The hazard ratio of recovery from severe CAP in pediatric patients who had no comorbidity was 1.67 hazard [AHR = 1.67, 95%CI: 1.33, 2.10, P = .000] more likely than who had comorbidity.
Additionally, the hazard ratio of recovery from severe CAP in pediatric patients who were early presenters for seeking care was 1.71 hazard [AHR = 1.71, 95%CI: 1.18, 2.47, P = .004] more likely than that of late presenters. The hazard ratio of recovery from severe CAP in pediatric patients who received oxygen therapy was 1.45 hazard [AHR = 1.45, 95%CI: 1.12, 1.87, P = .004] more likely than in those who did not (Table 4).
Bivariable and Multivariable Cox Proportional Hazard Regression Analysis of Risk Factors of Recovery Time From Severe CAP among Pediatric Admitted Between January 01, 2021 and December 31, 2022 at the Asella Referral and Teaching Hospital, Oromia Regional State, Ethiopia, 2023 (n = 412).
The bold p-value indicates statistically significant level.
Discussion
Approximately 10% of patients with CAP who come to the hospital require admission to critical care. Severe CAP remains a common cause of hospital admission. Severe CAP is also the most common cause of septic shock. It is associated with high rates of mortality and substantial morbidity. 16 Therefore, the present study aimed to determine the recovery time from severe CAP and risk factors among pediatric admitted to the Asella Referral and Teaching Hospital, Oromia Regional State, Ethiopia.
The present study showed that the median recovery time from severe CAP among pediatric patients admitted with severe CAP at the Asella Referral and Teaching Hospital was 5 days (IQR = 3-8 days). The finding of the present study was higher than the study conducted in Debre Markos (4 days). 24 The finding of the present study were also higher than those of a study conducted in Nepal (2 days). 26 This variation could be due to differences in sociodemographic characteristics, and this study addressed “severe pneumonia” rather than severe CAP.
The present study showed that the IDR of recovery from severe CAP among pediatric patients was 13.089 per 100 [95%CI: 11.82, 14.49] pediatric day observations. This finding was lower than the study conducted in Debre Markos (16.25 per 100). 24 The present study showed that the cumulative incidence of recovery from severe CAP among pediatric patients was 89.56% [95%CI: 86.20, 92.18]. This finding is consistent with that of a study conducted in Debre Markos (88.9%). 24
The hazard ratio of recovery from severe CAP in pediatric patients aged <3 years was 1.55 hazard [AHR = 1.55, 95%CI: 1.12, 2.13, P = .007] more likely than in children ≥3 years. This finding was supported by the study conducted in Debre Markos. 24 The hazard ratio of recovery from severe CAP in pediatric patients who were fully vaccinated was 1.29 hazard [AHR = 1.29, 95%CI: 1.03, 1.63, P = .027] more likely than pediatric patients who were partially vaccinated. This finding was supported by the study conducted in Debre Markos. 24 This is because vaccines encourage the immune system to fight infections more efficiently by stimulating immune responses to specific diseases. If the virus or bacteria invades the body in the future, the immune system will already know how to fight it. 27
The hazard ratio of recovery from severe CAP in pediatric patients who had no danger signs on admission was 1.61 hazard [AHR = 1.61, 95%CI: 1.26, 2.05, P = .000] more likely than pediatric patients who had danger signs on admission. This finding was supported by a study conducted in Debre Markos. 24 In fact, since the danger sign is the severity of child’s health status, there will be a high physiological disturbance in the child. Thus, children require a long time to recover from their disease. The hazard ratio of recovery from severe CAP in pediatric patients who had no comorbidity was 1.67 hazard [AHR = 1.67, 95%CI: 1.33, 2.10, P = .000] more likely than those with comorbidity. This finding is supported by a study conducted in Gambia. 28 This could be because comorbidities would decrease the time to recovery from severe CAP by weakening the immune system of children.
The hazard ratio of recovery from severe CAP in pediatric patients who were early presenters for seeking care was 1.71 hazard [AHR = 1.71, 95%CI: 1.18, 2.47, P = .004] more likely than that of late presenters. This finding was supported by a study conducted in Debre Markos. 24 This might be because delays in receiving adequate care for children with pneumonia can be life threatening. 29 This is because a longer delay in seeking care leads to a longer deterioration of the body. Therefore, the body requires more time to recover from such deterioration. The hazard ratio of recovery from severe CAP in pediatric patients who received oxygen therapy was 1.45 hazard [AHR = 1.45, 95%CI: 1.12, 1.87, P = .004] more likely than in those who did not. Oxygen is one of the most basic medical therapies for acute respiratory diseases, and has been an established part of medical practice for over 100 years. 30 Oxygen therapy, which involves the administration of supplemental oxygen, is one of the most effective treatments for pneumonia. Oxygen plays a crucial role in the healing process because it helps boost oxygen levels in the body, supporting the immune system in fighting infections. 31
Limitations of the Study
This study is a retrospective follow-up study that should be interpreted considering the following limitations. Since the study design was a retrospective follow-up study based on data extraction from patient medical records, predictors such as hospital-related factors, environmental-related factors, family wealth index, and other parental variables were not incorporated.
Conclusion
The median recovery time from severe CAP among pediatric patients admitted with severe CAP was relatively high. The IDR of recovery from severe CAP was 13.089 per 100 [95%CI: 11.82, 14.49] pediatric days observations. The cumulative incidence of recovery from severe CAP was 89.56% [95%CI: 86.20, 92.18]. Age, vaccination status, presence of danger signs, presence of comorbidities, duration of seeking care, and oxygen therapy were statistically significant risk factors of recovery time from severe CAP among pediatrics.
All concerned bodies, such as the healthcare providers, local and national policy makers and implementers, stakeholders, and pediatricians, need to focus on strategies to reduce the recovery time from severe CAP among pediatric patients. The identified risk factors for recovery time from severe CAP must be incorporated into the management of this disease in pediatrics. Prospective studies are recommended to incorporate hospital-related factors, environmental-related factors, family wealth index, and other parental variables.
Footnotes
Acknowledgements
The author would like to thank the Asella Referral and Teaching Hospital, Arsi University, and the data collectors.
Author Contributions
The author has made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work. Finally, he has read and approved the final manuscript.
Availability of Data and Materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the ethical review and research committee of the Nursing Department, College of Health Sciences, Arsi University, after a thorough assessment of the study for its scientific contribution and ethical issues. A letter of permission was received and sent to Asella Referral and Teaching Hospital and permission was obtained from the concerned body before the commencement of this study. The requirement for informed consent was waived because of the nature of the study design; retrospective study design and as the study depended on secondary data collected from patients’ medical charts. No individual consent is required as the study depends on secondary data; data were collected from the patients’ medical charts by using a data extraction format. Furthermore, all methods were performed in accordance with the ethical standards as laid down in the Declaration of Helsinki and its later amendments or comparable ethical standards.
Consent for Publication
Not applicable.