
Abstract
Objectives. Preterm infants are at risk of hypothermia. This study described the available infant warming devices (IWDs) and explored the barriers and facilitators to their implementation in neonates in Malawi. Methods. A qualitative descriptive study was conducted among 19 health care workers in Malawi from January to March 2020. All interviews were digitally recorded, transcribed, and managed using NVivo and analyzed using a thematic approach. Results. The warming devices included radiant warmers, Blantyre hot-cots, wall-mounted heaters, portable warmers, and incubators. Inadequate equipment and infrastructure and gaps in staff knowledge and capacity were reported as the main challenges to optimal IWD implementation. Caregiver acceptance was described as the main facilitator. Strategies to optimize implementation of IWD included continuous practical training and adequate availability of equipment and spare parts. Conclusion. Implementation of warming devices for the management of neonatal hypothermia is effective when there are adequate human and material resources.
Background
Globally, preterm births (<37 weeks) occur in 11% of all newborns and are the leading cause of death in children under the age of 5.1-3 Approximately 1 million children die around the world each year due to prematurity complications, with a disproportionate burden in low- and middle-income countries (LMICs).3,4 The rate of preterm births in Malawi has remained alarmingly high, up to 19.3%. 5 Respiratory distress and neonatal sepsis are leading causes of death among preterm infants, though hypothermia is often a neglected contributory cause. 6 A study from Malawi found that the effectiveness of treating respiratory distress in preterm infants was limited due to pervasive hypothermia. 7 Preterm infants have an immature thermoregulatory system and are at risk of hypothermia. Preterm and low birthweight (LBW) infants have a large surface area to weight ratio, limited brown fat, and an inability to shiver, all of which increase the risk of body heat loss.8-11
Neonatal hypothermia is defined as an axillary temperature below 36.5°C and is associated with higher rates of morbidity and mortality.12-14 The World Health Organization (WHO) recommends thermal care for the management of hypothermia in an interlinked manner, which includes the following measures: ensuring that delivery occurs in a warm room: Immediate drying of the baby, skin-to-skin contact with the mother, immediate and frequent breast-feeding, delayed bathing and weighing of the baby to minimize exposure to cold temperatures, appropriate clothing and bedding to minimize heat loss, keeping mother and baby together to foster breastfeeding, warm transportation if a baby needs to be moved, warm resuscitation and training, and awareness-raising on thermal care.15,16 WHO further recommends that hospitals that treat sick and low-birth-weight babies should be equipped with other warming devices such as low-reading thermometers, heated mattresses, overhead heaters, and incubators. 15 Furthermore, it is recommended that caregivers and healthcare professionals ensure that a newborn is not experiencing hyperthermia as a result of wearing too much clothing or having bedding that is too warm for the surroundings because this may compromise the brain, cardiovascular, and respiratory systems, which can be fatal. 17 The WHO Immediate Kangaroo Mother Care Study (iKMC) proposes the implementation of immediate Kangaroo Mother Care (KMC) for LBW infants receiving clinical care because it significantly reduces the rate of neonatal death. 18 Previous studies in Sub-Saharan Africa have reported suboptimal adherence to the thermal care guidelines.19-21 Even when routine thermal guidelines are followed and with a high rate of knowledge on the relevance of keeping babies warm22,23 keeping preterm infants warm in the delivery room is still difficult. 24 Neonatal hypothermia is associated with a higher risk of mortality especially among neonates that are admitted to a neonatal unit with it. 13 The use of plastic coverings, heated mattresses, and skin-to-skin contact has been shown to keep infants warmer within normal body temperature ranges, with reduced hypothermia on admission to neonatal intensive care units (NICUs), especially for very preterm infants. 24 Currently, the WHO strongly recommends the use of radiant warmers or incubators for LBW infants unable to or in unstable health to use KMC. 25 While KMC is an important intervention for keeping small infants warm, alternative infant warming methods when KMC is not appropriate or feasible have been neglected. Though there is evidence demonstrating the benefits of infant warming devices (IWDs), implementation remains a challenge. In particular, the availability of IWDs and the factors that impact their implementation are not fully understood in resource-limited health settings in LMICs.26-28 The purpose of this paper is to describe the IWDs available and explore the barriers and facilitators to their implementation in Malawian hospitals. This information is important in a setting like Malawi, where neonatal hypothermia remains high, with rates of 77% among neonates admitted to tertiary facilities in the southern part of Malawi. 13 Neonatal hypothermia is among the main causes of mortality, despite the availability of infant warming devices.
Methods
Study Design
We conducted a qualitative descriptive study 29 at a secondary and tertiary level hospital in Malawi from January to March 2020 among healthcare workers (HCWs) to describe the availability and use of warming devices among neonates in their routine care environment. Following a phenomenological approach, this design allowed for broad insights into implementation grounded in HCW experiences. Our phenomenological approach considered those healthcare workers who had worked in the setting for more than 3 months and had experience using infant warming devices in the setting. This study was part of the larger project, “Integrating a neonatal healthcare package for Malawi” to understand implementation of evidence-based neonatal intervention, funded as part of the Innovating for Maternal and Child Health in Africa (IMCHA) initiative. KMC is reported in other components of the overall project,30,31 while the current study focuses on the technologies employed in the maternity wards in the hospitals to keep infants warm, particularly vulnerable small and sick infants. We have reported the study following the COREQ Checklist.
Study Setting
The study was conducted in 2 government-run hospitals located in southern Malawi. The tertiary central hospital is situated in an urban center while the secondary-level district hospital is in a rural location. The selection of these facilities was guided by the Malawi Ministry of Health because they represented various geographic health service zones and Malawi’s available health management structures, which are tertiary and secondary levels of health service provision in Malawi. At both facilities, basic services are offered without charge. 32 We intended to include 4 facilities in the study; however, due to the COVID-19 pandemic and after evaluating transcripts for content comprehensiveness, the research team determined that data saturation had been reached with the data collected from the district hospital and tertiary hospital. The neonatal unit at the tertiary hospital has a total admission capacity of 75 patients, including 40 NICU spaces and 35 beds in the kangaroo mother ward for mother-baby pairs. The neonatal unit at the district hospital has an admission capacity of 12 patients, including 4 KMC beds. When determined to be in stable condition (no signs of fever, hyperthermia, weight loss, sunken eyes, protruding fontanel, or failure to feed), preterm and low birth weight (<2500 g) newborns are admitted to KMC. 31 Medical equipment in the Malawi health system is centrally purchased with guidance from the Physical Assets Management (PAM) which is a unit under the Health Technical Support Services (HTSS) department in the Ministry of Health. The HTSS department governs the purchase and standardization of equipment that is purchased in Malawi’s health facilities, to ensure quality and functional equipment. 33 Additionally, equipment in the neonatal nurseries in Malawi is being supported through the Newborn Essential Solutions and Technologies (NEST) which is a program working in all facilities to supply neonatal equipment and training healthcare workers on neonatal health. 34
Sampling and Sample Size
We drew a purposive sample of 19 service providers and supervisors working in neonatal health and in the neonatal wards of the 2 facilities. These included nurses, clinicians, pediatricians, and district health management members overseeing service delivery, such as the director of health and social services, district medical officers, and district nursing officers. We estimated a sample of 5 to 10 healthcare workers per facility to acquire saturation based on the number of staff within neonatal units at each facility and deemed that the sample drawn would be adequate as suggested by Baker et al. 35
Recruitment of Study Participants and Data Collection
The study staff introduced the project to the clinical management teams in the 2 hospitals at the beginning of the project. No potential participants refused participation. Data were collected between January and March 2020 through in-depth interviews using an interview guide, including 16 in-person and 3 telephone interviews. Two nurses working in a neonatal unit tertiary facility participated in a pilot for the interview guide. The pilot data was not included in the analysis; instead, it was used to improve the wording of the questions. Before recruiting participants, the interview guide was translated into Chichewa, the primary local language of Malawi. Interviews ranged from 30 to 60 minutes. The 5 Malawian research staff, SS, BC, FC, LC, and EM (three certified nurse midwife technicians and 2 public health specialists; 4 female and 1 male) were trained before data collection. All researchers had no prior relationships with study participants, and none had worked in the study facilities. They introduced themselves as members of the IMCHA project from the College of Medicine at the University of Malawi and explained the study in detail before obtaining consent. Since data collectors included those with nursing backgrounds, the researchers reflected on their own experiences and knowledge of the use of IWDs to avoid bias during recruitment and data collection.
Interviews were conducted in the participants’ language of preference. The interviews with HCWs were largely in English, the language commonly used in health sciences in Malawi, with some Chichewa words as needed. All interviews were audio recorded and were conducted in a private location at the facility and audio-recorded with permission. To minimize interference with the work schedules and responsibilities of healthcare workers, all interviews were conducted during off-duty hours. The participant and the researcher were the only people present during the interviews; there were no follow-up interviews. The interview process, flow, and participant behavior were all documented in the field notes that the researchers collected while conducting the interviews. 36
After an interim review that evaluated the saturation of concepts and established protocols to halt the spread of COVID-19, data collection was finished. We identified saturation of ideas when there was no new information found in the transcripts, and we followed up with 3 telephone interviews to confirm this. As a kind of member checking, the main points from each interview were summed up for the participants’ confirmation. 37
Data Management and Analysis
All data were stored on password-protected computers and cabinets at the university, with access limited to study researchers. Audio recordings were transcribed verbatim, Chichewa words were translated into English where necessary, and transcripts were managed using NVivo 12 software (QSR International, Melbourne, Australia). Each participant had a unique identifier to maintain confidentiality.
We analyzed the data thematically following a coding guide that was developed following a discussion of the pilot transcripts. 38 Our analysis included the pilot interview data because our goal was exploratory. SS coded all data under the supervision of MWK and ALNM and discussed by the team regularly. All themes were generated from the data and verified against the audio to ensure that they correctly reflect the data. Findings were member-checked with pediatric clinical experts in Malawi (KK, EMM, TH, QD) to ensure the relevance and accuracy of the themes within the local context.
Results
Characteristics of Health Care Workers
Nineteen interviews were conducted among healthcare workers; 10 were from the tertiary hospital. Of the 19, 8 were nurses, 4 were clinical officers, 2 were nurse officers in charge of the neonatal unit, 3 were district health management officials, and 2 were pediatric doctors, and both doctors were based at the tertiary level facility. The secondary-level facility had no pediatricians. The director of health and social services and the district nursing officer did not provide direct clinical care to neonates; they made decisions on the purchase and distribution of human and material resources to the neonatal units. All healthcare workers had no relationship with the industries that manufacture devices.
Available Devices and Level of Comfort in Usage
The district hospital had radiant warmers and wall heaters, while the tertiary hospital had radiant warmers, wall heaters, Blantyre Hot Cots, and portable warmers. The Blantyre Hot Cot is a local innovation featuring a wooden crib and 4 incandescent light bulbs to warm the air in the crib. Radiant warmers were preferred at the district hospital because of their ease of use. Healthcare workers outlined the advantages and disadvantages of each device as stipulated in Table 1.
Description of Infant Warming Devices.

Facilitators for the Use of Infant Warming Devices
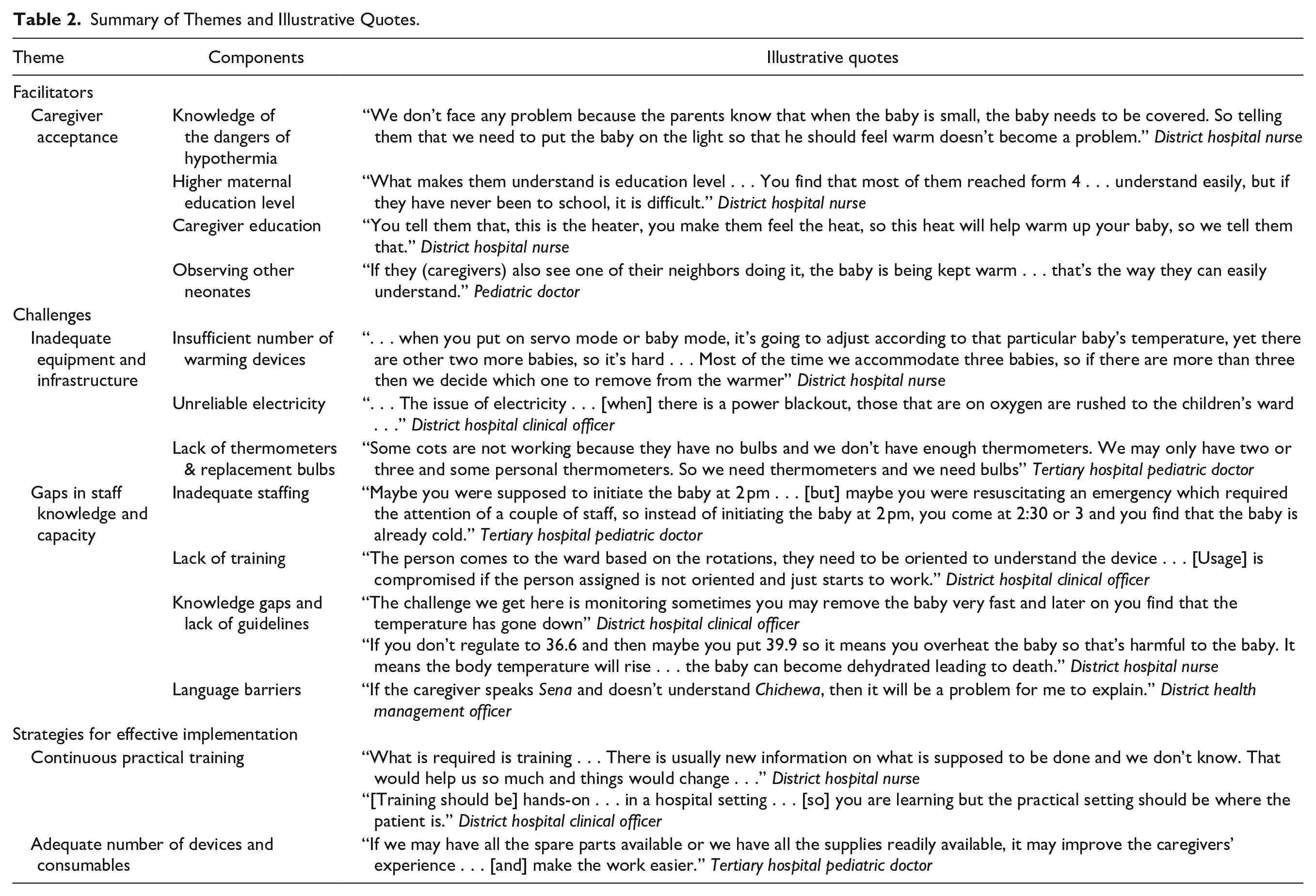
Overall, caregiver acceptance was identified as the key facilitator for IWD use at both the district and tertiary hospitals. Caregiver acceptance was supported by knowledge of the dangers of hypothermia, a higher maternal education level, adequate counseling with simple hands-on demonstrations, and when mothers observed other neonates with IWDs (Table 2). A common understanding among caregivers that infants, particularly small infants, need to be warm made the usage of IWDs easy to explain. Mothers with secondary school education in particular understood quickly. To support caregiver acceptance, HCWs allowed family members to test the devices by asking them to put their hands under the warmer to allay any misconceptions about potential harm. Health workers stressed the need to use hands-on demonstrations and simple language as opposed to using medical terms that left them confused. Caregivers tended to accept IWDs better once they observed other neonates receiving the same care.
Summary of Themes and Illustrative Quotes.
Challenges to the Use of Infant Warming Devices
Inadequate equipment and infrastructure were key challenges to the overall use of IWDs reported by HCWs (Table 2). Delays occurred due to a limited number of IWDs available or placement in another ward. In particular, the district hospital did not have a warmer in the ceasarian section operating room. Limited numbers of IWDs led to putting 2 or more neonates under 1 warmer, which meant that temperature sensors on the device would be inaccurate. This added extra workload as HCWs would then need to operate the device manually, which required careful and frequent monitoring. Unreliable electricity and the lack of thermometers and replacement bulbs were also reported as challenges.
Challenges were also reported related to staff knowledge and capacity. IWD initiation may be delayed when there are many infants in the unit requiring care or if there is another infant’s urgent attention, such as requiring resuscitation. HCWs also reported a lack of competency in operating the devices, stating that they are sometimes assigned to the neonatal unit without clear training on the devices. Limited knowledge of how to operate and regulate the devices led to concerns about overheating an infant and premature removal. There were unclear guidelines around removal from the IWD and transfer to the KMC ward, leading to debates among HCWs. Language barriers between HCWs and caregivers were also reported as a challenge.
Strategies for the Effective Use of Infant Warming Devices
Health workers recommended continuous training to introduce new knowledge and orient new staff members, with an emphasis on practical skills in the hospital setting (Table 2). Reliable access to devices, consumables, and spare parts would also help optimize the implementation of warming devices.
Discussion
The warming devices available in Malawian hospitals included radiant warmers, Blantyre hot cots, wall-mounted heaters, portable warmers, and incubators. Blantyre hot cots and portable warmers were not implemented at the district hospital. The radiant warmers were favored among all the warming devices. Inadequate equipment and infrastructure and gaps in staff knowledge and capacity were reported as the main challenges to optimal IWD implementation. Caregiver acceptance was described as the main facilitator. Strategies that were recommended to optimize implementation of IWD included continuous practical training and adequate availability of equipment and spare parts. Our findings on the preference for automated warming devices that are servo-controlled are consistent with findings from previous studies.24,28 However, automated warming devices cannot be effectively used when there is overcrowding and unreliable electricity. Automated devices are preferred over manual ones because of their ability to minimize accidental overheating. 24 The limited preference for Blantyre hot cots could stem from the need for manual temperature monitoring and adjustment of the bulbs in the cots, 39 and the limited preference for wall heaters could be due to neonates experiencing hypothermia even in warm rooms. 24 An earlier study also reported that radiant warmers were preferred because of their ease of use, though they remain expensive for facilities to purchase. 28 Although automated devices remain appealing in the Malawian health system, which is constrained by a shortage of healthcare workers, 40 they are challenged by feasibility barriers like overcrowding, erratic electricity, and access to supplies. The inadequacy of the devices and supplies, particularly at secondary-level facilities, is consistent with previous reviews from LMICs and the sub-Saharan African region26,28 and was also observed in our earlier facility assessments of neonatal care services in Malawi. 41 As Malawi strengthens neonatal care, it is imperative to ensure that facilities have adequate and contextually appropriate human and material resources. 26 The lack of confidence in using IWDs found in our study is consistent with previous studies that have shown that gaps in training over thermal regulation devices compromise the use of the devices.26,27 The Care of the Infant and Newborn (COIN) manual for Malawi is a comprehensive document that has the potential to resolve gaps in knowledge among HCWs. 39 This training is offered both in pre-and in-service training for healthcare workers, thereby creating platforms for strengthening skills. 39 The situation in Malawi is also likely to improve with the investment in newborn technologies initiated by the Newborn Essential Solutions and Technologies (NEST) program which includes building dedicated neonatal units in district hospitals equipped with resources for thermal management. 34 However, to sustain the level of investment made by NEST, there is a need to revise health services financing for the reliable purchase of consumables and maintenance 42 as well as adequate staffing and training needs.
Our study highlights some HCW-related barriers that have previously been reported in the management of most neonatal technologies.11,32,43-45 The inadequate competence levels of healthcare workers in operating neonatal technologies have been reported earlier.11,32,44 The heavy workload of health care workers compromises care, a finding consistent with previous reviews that reported that workload and inadequate pre-service training in neonatal care impede optimal delivery.46,47 Similar to findings on breastfeeding support, it’s possible that the widespread belief among HCWs and caregivers that neonates, especially small and sick infants, need to be kept warm contributed to the lack of attention thus these infants were less of a priority than those requiring urgent care. However, our study finds training and supervision are required, especially with the preference for automated technologies. Training and implementation of guidelines would also be beneficial for the appropriate timing of removal from IWDs and the delivery of KMC.
With the findings of the recent WHO iKMC study that immediate KMC of LBW infants receiving clinical care significantly reduces the rate of neonatal death, 18 guidelines will be updated, and training will be important to clarify when to use an IWD or KMC. Training staff will be essential so they can also adequately explain the use of IWD and/or KMC to caregivers. In contrast to either one or the other, the use of IWDs and KMCs can be complementary. Provisioning IWDs in the KMC ward could improve the quality of life for mothers providing KMC so they could rest, prepare, and have meals, and go to the washroom. 48 Though counter-intuitive, the provisioning of IWDs in the KMC ward could potentially encourage mothers to stay longer at the facility until their infants are of adequate weight instead of self-discharging early to go home, where there is more support available from family members. IWDs will continue to play an important role in care to support the effective implementation of KMC and iKMC with a focus on family-centered care that highlights the needs of infants and the well-being and capacities of their caregivers.
Strengths and Limitations
Strengths of this study include research in both a secondary and tertiary level health facility to broaden the transferability of findings, collaborative analysis between Malawian and Canadian qualitative experts, member checking the findings with clinical experts in Malawi, and reviewing themes against the audio files to support credibility. Halting data collection early due to the COVID-19 pandemic is the main limitation of our study. However, we believe that including 1 tertiary and 1 secondary level facility in the study highlights the implementation challenges and enablers in the 2 levels of care. Future studies should focus on caregivers to achieve a comprehensive description. It is challenging to assess the total amount of equipment used by each staff member or patient because we did not record all the devices that were available for use in our study. To convey the sufficiency and use of the devices, we also did not put a number on the number of preterm and low birthweight babies. In the future, research endeavors may employ quantitative methodologies to evaluate the equipment’s usability and effectiveness, thereby offering a comprehensive perspective on the technology.
Conclusion
Implementation of warming devices is effective in reducing rates of hypothermia when there are adequate human and material resources. Supporting caregivers and health workers with training in the implementation of various devices facilitates their use. Future research should focus on assessing caregivers’ experiences with warming devices and how caregivers interact with their neonates when receiving thermal care.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241248982 – Supplemental material for Factors Influencing the Implementation of Infant Warming Devices Among Healthcare Workers in Malawian Hospitals
Supplemental material, sj-docx-1-gph-10.1177_2333794X241248982 for Factors Influencing the Implementation of Infant Warming Devices Among Healthcare Workers in Malawian Hospitals by Alinane Linda Nyondo-Mipando, Mai-Lei Woo Kinshella, Sangwani Salimu, Brandina Chiwaya, Felix Chikoti, Lusungu Chirambo, Ephrida Mwaungulu, Mwai Banda, Tamanda Hiwa, Marianne Vidler, Elizabeth M. Molyneux, Queen Dube, Joseph Mfutso-Bengo, David M. Goldfarb and Kondwani Kawaza in Global Pediatric Health
Supplemental Material
sj-pdf-1-gph-10.1177_2333794X241248982 – Supplemental material for Factors Influencing the Implementation of Infant Warming Devices Among Healthcare Workers in Malawian Hospitals
Supplemental material, sj-pdf-1-gph-10.1177_2333794X241248982 for Factors Influencing the Implementation of Infant Warming Devices Among Healthcare Workers in Malawian Hospitals by Alinane Linda Nyondo-Mipando, Mai-Lei Woo Kinshella, Sangwani Salimu, Brandina Chiwaya, Felix Chikoti, Lusungu Chirambo, Ephrida Mwaungulu, Mwai Banda, Tamanda Hiwa, Marianne Vidler, Elizabeth M. Molyneux, Queen Dube, Joseph Mfutso-Bengo, David M. Goldfarb and Kondwani Kawaza in Global Pediatric Health
Footnotes
Acknowledgements
This manuscript is part of the “Integrating a neonatal healthcare package for Malawi” project within the Innovating for Maternal and Child Health in Africa (IMCHA) initiative. The authors are grateful to the IMCHA team for their support, the study participants for their voluntary participation, and the Directors of the various institutions included in the study for allowing us to conduct the study in their facilities.
Abbreviations
COIN—Care of the Infant and Newborn; COVID-19—Corona Virus Disease 2019; HCWs—Healthcare Workers; HTSS—Health Technical Support Services; iKMC—Immediate Kangaroo Mother Care; IMCHA—Innovating for Maternal and Child Health in Africa; IWDs—Infant Warming Devices; KMC—Kangaroo Mother Care; LBW—Low birthweight; LMICs—Low and Middle-Income Countries; NEST—Newborn Essential Solutions and Technologies; NICUs—Neonatal Intensive Care Units; PAM—Physical Assets Management; WHO—World Health Organization.
Author Contributions
ALNM led the qualitative component of the project and developed the methodology and supervised the investigation, data analysis, and drafted the original paper with support from MWK, SS, BC, FC, LC, EM, TH, and JMB contributed to the investigation and data analysis and MB was the project administrator. SS coordinated data collection activities and contributed to the investigation and analysis. MV and EMM reviewed all versions of the paper and contributed to the interpretation and structure of the paper. QD, DMG, and KK contributed to the conceptualization of the research project and its funding acquisition and reviewed all versions. All authors have read and approved the manuscript. ALN-M: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. M-LWK: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. SS: contributed to acquisition and analysis; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. BC: contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. FC: contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. LC: contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. EM: contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. MB: contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. TH: contributed to design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. MV: contributed to conception and design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. EMM: contributed to conception and design; contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. QD: contributed to conception and design; contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. JM-B: contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. DMG: contributed to conception and design; contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. KK: contributed to conception and design; contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are not publicly available due to participant privacy but are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was carried out with the aid of an IMCHA grant (108030) funded by Global Affairs Canada, the Canadian Institutes of Health Research, and Canada’s International Development Research Centre. The funders had no role in the study design, data collection, analysis, decision to publish, or preparation of the manuscript.
Ethical Approval and Consent to Participate
Ethics approvals were obtained from the University of Malawi College of Medicine (P.08/15/1783) and the University of British Columbia (H15-01463-A003). All hospitals provided institutional support for the study to be conducted in their facilities. All participants provided written informed consent before study participation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.