
Abstract
Background. Child abuse in Suriname has a prevalence between 58.2% and 68.8%. This prospective observational study evaluates the implementation of screening for child abuse at the Emergency Department (ED) of the Academic Hospital Paramaribo (AZP). Methods. Children (0-16 years) presenting with injury from 01-02-2018 until 31-08-2018 were eligible. Case-record-forms were completed. Multidisciplinary meetings were used to evaluate positive screened and admitted patients. Diagnostic accuracy was calculated and results were compared to retrospective data from 2016. Results. 3253 Children attended the ED. In 1190 (36.6%) children, the screening was completed. The screening was positive in 148 (12%); in 71 (6%) cases child abuse was confirmed. The sensitivity and specificity were 0.88 and 0.92 respectively, PPV 0.43, NPV 0.99. There was a significant increase of detected child abuse cases; 4.4% in 2016 versus 6% in 2018 (P = .04). Conclusion. Implementation of screening at the ED in the AZP increased detection of child abuse. To improve screening’s accuracy, more education for healthcare professionals is pivotal.
Introduction
The World Health Organization (WHO) estimates that 23% of all children worldwide are being exposed to physical abuse in the past year. 1 The prevalence of child abuse in low income countries such as Tanzania, Zimbabwe, Malawi ranges from 42% to 64% in girls and 53% to 76% in boys.1,2 Furthermore, high incidences of child abuse are reported in middle-income countries such as the Caribbean islands. A study in Aruba showed a prevalence of child abuse in 1 of 15 children (which is 66.1 per 1000 children). 3 Of these children, 25% was the victim of physical abuse and 20% of physical neglect. Although the incidence of child abuse in low- and middle-income countries is in general poorly available, a study published in 2015 estimated a prevalence of 58.2% to 68.8% of child maltreatment in Suriname. 4 These data indicate that child abuse is endemic in Suriname.
Physical, emotional, and sexual abuse of children is a major health problem with serious consequences for the victims and society. The emergency Department (ED) plays a crucial role in the detection of child abuse. Screening for child abuse at ED is known to increase the detection rate of potential child abuse, further a routinely performed physical examination is known to detect abuse cases which would have been missed by the screening.5,6 However, to date of this study, the existing screening tools were only validated in high-income countries. Further, there are many educational programs focusing on child abuse in high-income countries, in contrast to middle- and low-income countries. In these countries, the care system and education level of professionals regarding child abuse is underexposed. Suriname is a middle-income country at the South-American continent. There are 4 hospitals in the capital city (Paramaribo), of which only the Academic Hospital Paramaribo (AZP) has an ED. The majority of the population of Suriname lives in, close to the capital, and forms a close-knit community. Therefore, if the screening is effective in the emergency department of Suriname, the detection of child abuse may increase and interventions can be initiated and may be converted to other middle- and low-income countries.
The aim of our study was to evaluate the implementation of a systematic screening on child abuse and neglect at the emergency department of the Academic Hospital Paramaribo in Suriname.
In a prospective observational cohort study, we included all children who attended the emergency department of the Academic Hospital Paramaribo (AZP), Suriname, between February 2018 and August 2018.
Methods
Research Ethics Statement
The Ministry of Public Health and the Human Research Ethics Committee of Paramaribo, Suriname approved this study (REF: VG03-18). This study was a prospective observational cohort study that was performed from February 2018 for the duration of 6 months (until August 2018) at the emergency department of the Academic Hospital Paramaribo (AZP), Suriname. Prospectively collected data were compared to retrospectively collected data from February 2018 until August 2018.
Patient and Public Involvement
Study participants or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Objectives
The main aim of the study was to evaluate the effectiveness of a systematic screening on child abuse at the emergency department in combination with the implementation of a multi-disciplinary meeting in Paramaribo, Suriname. The effectiveness of the screening was defined as number of accurate child abuse referrals to the pediatrician and/or multidisciplinary meeting (MDM). Secondary outcomes were the incidence of child abuse among children with traumatic injuries and the mortality and hospitalization rate due to child abuse.
To assess the effectiveness, the prospective collected data were compared to retrospective collected data from the same period in the year before.
Participants
Eligible for inclusion were all children (aged 0-16 years) who visited the emergency department with (suspected) traumatic injuries; including those caused by sexual abuse, psychological abuse or any other form of abuse. Patients were excluded when parents or children refused to participate in the study. All included patients gave written confirmed consent at the beginning of the ED visit. In case of patients aged 16 years or older, consent was received from the patients only, in case of patients aged between 12 and 16 years, consent was received from both patients and parents and in case of patients younger than 12 consent was received from parents only.
Definitions and Outcomes
The definition of child abuse used in this study is in line with the maltreatment definition of the World Health Organization (WHO). 7 Child abuse is an umbrella term that encompasses many forms of abuse, including inflicted trauma and neglect. Inflicted injuries are caused by force of impact through direct actions of someone other than the child (regardless of motive), for example, physical abuse, negligent injuries are caused by a failure to protect children from physical harm (either by a lack of supervision and/or an unsafe environment), accidental injuries were caused without any reasonable doubt about inflicted trauma or neglect. The screening was completed for children presenting with injuries to the ED, in order to detect inflicted injuries or injuries as a result of neglect. However, each child was evaluated for the presence of other forms of abuse.
Child abuse was confirmed by either agreement during the multi-disciplinary meeting, by confession of the caregiver or by legal authorities. The multi-disciplinary team consisted of a pediatrician, emergency department doctor, pediatric psychiatrist, legal authorities, and social work. In order to quantify our outcomes, we analyzed the number of accurate child abuse case referrals to the pediatrician, conclusions of the multi-disciplinary team meeting and (safety) measures taken after the meeting for these children (ie, social-work accompaniment, police investigation, sent home without measures etc.).
Study Procedures and Data Collection
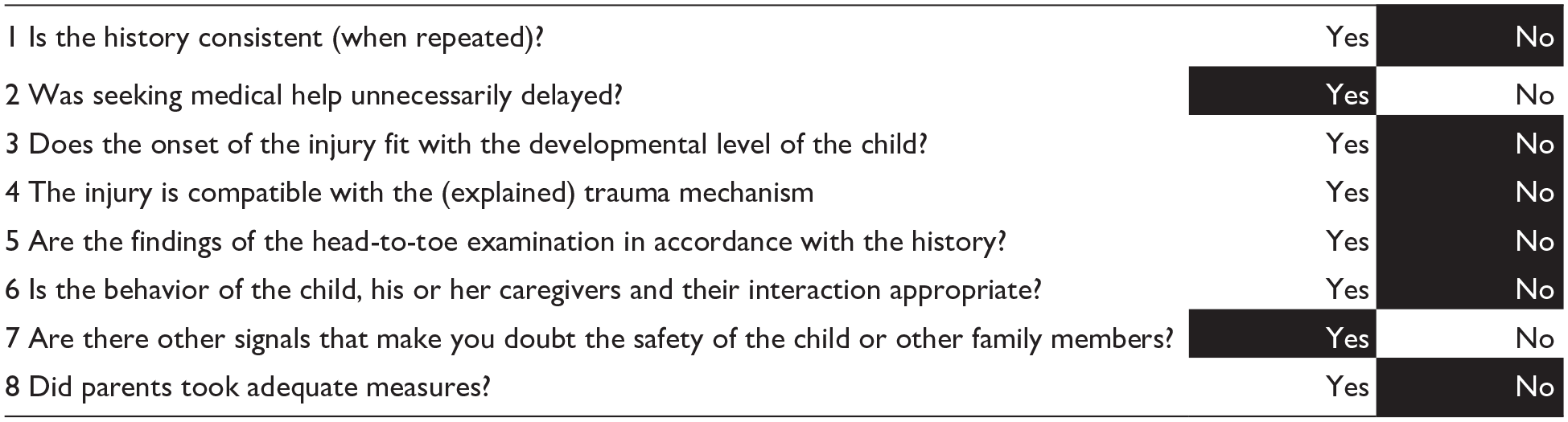
The screening, which is a version of the extensively studies SPUTOVAMO, was implemented as standard of care at the emergency department (ED). The screening was completed by the treating doctor at the ED (Table 1). The researcher such as collected other data: Demographic data, type of injuries, referral to the pediatrician and the conclusion of the multi-disciplinary team.
The screening test. Black boxes are considered “positive” if one or more are ticked and indicate possible child abuse. The screening is “negative” when none of the black boxes is ticked.

The standard care consisted of a total physical examination by the ED doctor, collection of medical history and completion of the screening. Please refer to Figure 1 for the study procedure after completing the screening.
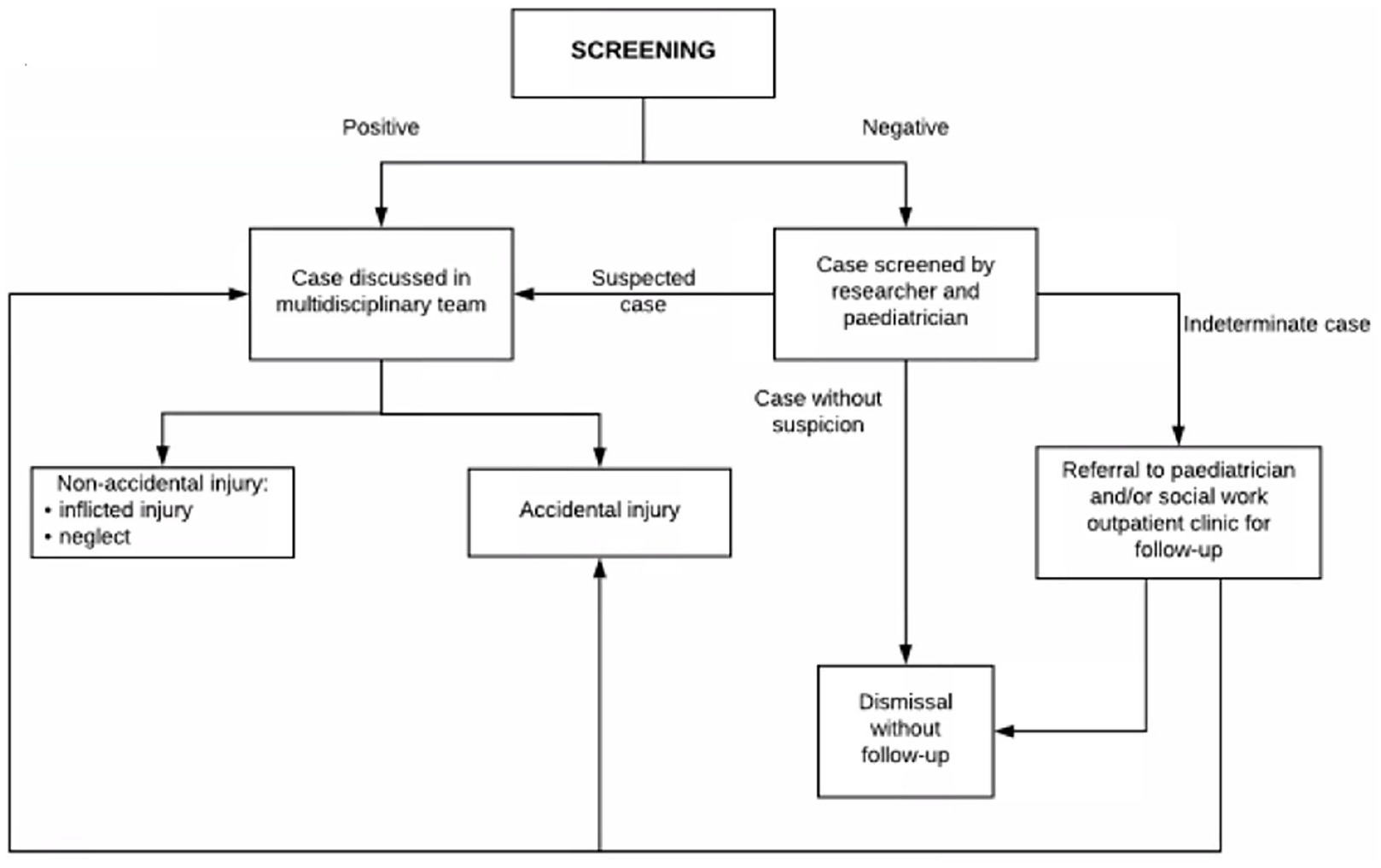
Study procedure flow diagram after completion of the screening.
Retrospective data was collected in order to compare study results to the previous situation without any screening on child abuse at the ED. Abused patients were identified via ICD-10 codes and collected in a database by social work. In their database they differentiated between physical child abuse (deemed assault) and other forms of child abuse (deemed child abuse) for which reason we have reported both likewise in the manuscript. All ED admissions were collected, including demographics, information on injuries and the mechanism of injury (abuse or accidental injury). This data were collected from February 2018 until August 2018.
Data Analyses
All analyses were performed with the Statistical Package for Social Sciences (SPSS version 25). Quantitative variables were summarized as mean and standard deviation (SD); categorical variables were expressed as counts and percentages. The sensitivity, specificity and positive- and negative predictive value of the screening test was calculated using a 2 × 2 table. Retrospective data was collected in Excel and converted to SPSS for analysis. A P-value less than .05 was considered statistically significant and 95% confidence intervals were calculated.
Results
During the study period 3253 children attended the emergency department (ED), excluded were children with an unclear outcome (no conclusion on child abuse was possible) and children without screening (n = 2063). Included for analyses were children with a completed screening, which were 1190 (36.6%) admissions. The mean age of the children was 6.1 years (SD ± 4.47) and there were 682 (57%) boys. During the study period, none of the children and/or parents refused to participate in this study. In total 71 (6%) child abuse cases were identified.
Retrospective Data
To compare results, we collected retrospective data of all children who attended the ED between March 2016 and August 2016. In total 2322 children attended the ED. There were 1370 (59%) boys and the mean age was 9.7 years (SD ± 5.24). Child abuse was diagnosed in 102 (4.4%) children and any form of physical child abuse (assault) in 160 (6.9%).
Compared to the retrospective data there was a significant increase in detection of child abuse cases during our study period (P = .04).
Screening Test
The screening was completed in 1190 (36.6%) children and positive in 148 (12%). The screening was completed in 29% during office hours (7am-3pm), in 47% in the evening (3pm-10pm) and in 24% during night hours (10pm-7am). Demographic characteristics of abused and non-abused (accident) children are provided in Table 2.
Demographic and clinical information of the child abuse group and no child abuse group.

Accuracy of the Screening
The sensitivity of the screening was 0.88 and specificity 0.92. The positive likelihood ratio was 11 and negative likelihood ratio was 0.13, the positive predictive value (PPV) was 0.43 and negative predictive value (NPV) 0.99. The calculation was based on Table 3.
The 2 × 2 table was used to calculate the accuracy of screening.

Accuracy of Screening Questions
The sensitivity, specificity, likelihood ratios (LR), PPV, and NPV are calculated for all questions of the screening. Please refer to Table 4 in Supplemental File 1 for details on these data. Question 7, asking whether the physician had any concerns about the safety of the child and/or other family members and question 1, asking whether the history was consistent and question 3 about the compatibility of the injury with the developmental level of the child, have the highest calculated PPV 0.86, 0.64, and 0.60 respectively. Question 6 was the question with the lowest PPV (0.32).
Compared to the retrospective data (4.4% child abuse cases), the implemented screening detected 6% cases of child abuse during the study period.
Discussion
In this prospective observational cohort study, we showed that an implementation of a systematic screening on child abuse at the emergency department of the Academic Hospital of Paramaribo (AZP), Suriname, raised the detection of child abuse cases. We were able to notice the improvement in the detection due to our comparison between our prospective data and previous retrospective data of the same ED. We used an existing screening method, which was developed in high-income countries. It showed that the detection of child abuse cases in this middle-income country was raised as well.
Especially in a middle-income country like Suriname it is of utmost importance to conduct a study on the detection of child abuse. We are aware that the local situation in low- and middle-income countries is not comparable to high-income countries such as European countries. The main difference is that in Suriname (and many low- and middle-income countries) there is no follow-up system such as Child Protective Services (CPS, or “Veilig Thuis” in Dutch). The added value of a systematic screening in high income countries has been investigated in several studies with moderate results.5,6,8,9 However, studies in low and middle-income countries are lacking, which results in a knowledge gap highlighting the need for studies in this setting.
We are convinced that there is much to be gained when it comes to the detection of child abuse in low- and middle-income countries. 10 Mostly because of the high prevalence of injuries due to neglect or violence against children and a subordinate role for education about child abuse but in particular because people in low- and middle-income countries usually live in a close (small) community. Because of this close-knit community, it is challenging to initiate a screening and education program focusing on child abuse. 3
Our study results show that the screening in Suriname has raised the detection of child abuse. Moreover, compared to high income countries, the results of the screening in terms of sensitivity, specificity, positive- and negative predictive value were higher in Suriname.5,6,11 A reason for this finding can be that the pretest probability in Suriname is higher compared to for example the Netherlands, where the prevalence of child abuse in the conducted studies was lower. Another reasonable explanation is that the screening raised awareness among the doctors at the ED to pay attention to possible child abuse cases. This phenomenon was seen at the implementation of the systematic screening in the Netherlands as well. 12 Although it was not mandatory to complete the screening, it was completed in about 37% of admissions. This may have led to bias if the screening was completed when children where already suspected of child abuse by doters. On the other hand, we also noticed that dedicated doctors completed the screening more frequently compared to other doctors in both cases with or without suspicion. For doctors in low- and middle-income countries, it is harder to detect child abuse cases because of less attention in educational programs on child abuse, leading to a gap in knowledge and cultural differences. A systematic screening can be of help to overcome these issues both by providing a mnemonic during work as well as be a starting point for education on the subject. For example, during the study implementation, the researcher taught the healthcare professionals about child abuse. After the presentation 1 of the medical interns said that she did not know what child, abuse was and, in retrospect, found out that she had been abused in the past. At last, we believe that the differences may be caused by the fact that the screening in the Netherlands focusses on all types of child abuse, while the screening implemented in Suriname focused on physical child abuse and physical neglect. The high-income countries desire to detect all forms of child abuse at the emergency department, which is not feasible. 13 The ED staff gave feedback to the researchers that more education was desired, since they want to improve the detection of child abuse, however they did not feel competent because they did not know what to look for.
In addition, we showed the results per questions of the screening tool and concluded that these results differ from the results in high-income countries. Several studies in the Netherlands were conducted to assess the accuracy of screening.6,11,14 The highest PPV was 0.41 (95% CI: 0.29-0.55) for the question asking whether the location of the injury is usual (part of the SPUTOVAMO), 6 followed by the question “Does the onset of the injury fit with the developmental level of the child?” (part of the ESCAPE) 11 with a PPV of 0.21 (95% CI 0.13-0.32). Both questions were incorporated in the screening we used in Suriname.
Although the question which concerns the behavior of the child and their parents resulted in the lowest PPV in Suriname, this question has a lower PPV in the Netherlands (PPV 0.13 95% CI 0.07-0.22), which is not the lowest scoring question in the Dutch study. 11 Probably the interpretation of this question dependents on local cultural behavior or possibly the Suriname culture influences the assessment of behavior between a child and his/her caregivers. On the other hand, a possible explanation can be that doctors have difficulties in interpreting this question because of a lack of knowledge about “normal” interaction between parents and children. As previously said, the lack of education on child abuse and alarming symptoms can be a cause of a different interpretation of the screening questions. Furthermore, it was to be expected that there is a difference in outcome of the questions between Suriname and high-income countries such as the Netherlands.
Strengths
This study is carried out in a middle-income country, which is an important first step for the improvement and development of the care on child abuse in these countries. It provides important insights and knowledge about the situation in middle-income countries and exposes different challenges compared to high income countries, such as a knowledge gap about child abuse because this is less discussed in trainings. Although all the screening methods are designed in high-income countries, child abuse is prevalent in low- and middle-income countries as well. Therefore, it is pivotal to focus on these countries in order to improve the situation. Despite that there was a previous knowledge gap concerning child abuse and although no previous training on the use of the screening tool was provide, still the detection tool at the ED seemed to be filled in successfully, increasing the detection of child abuse at the ED. This suggests that the screening instrument is an easy-to-use method to increase the detection of child abuse at the emergency department in low- and middle-income countries. With this study, we showed the effects and pitfalls of the implementation of the screening on child abuse at the emergency department of a middle-income country.
Limitations
A limitation of the study is that there is a selection bias of included patients. This was not because of patient’s refusal to participate in the study, we had no refusals. However, we noticed that the selection bias occurred due to the dedication of the doctor on call. Some doctors were very dedicated and motivated to participate in the study, because of which many patients were included during their shift. While patients were missed during the call of other doctors. Although we noticed a slight improvement overtime, the difference between doctors remained. Another cause of selection bias is that the screening was more often completed during day hours versus night hours. For the implementation of a screening at the ED, it is pivotal to commit all the personnel in order to make it valuable. Interviews with all ED staff is advised prior to the implementation of such a procedure, in order to accomplish a good working collaboration and dedication of all staff. At last, the case identification of child abuse in our study was different compared to the retrospective data. This may be of influence of the results and comparability between the 2 groups. We may have overestimated the prevalence of child abuse in the retrospective data, because we were only able to use ICD-10 codes to identify these patients. Only the prospective collected data was discussed in a multidisciplinary meeting. It is known that the reference standard, especially since there is a lack of gold standard to diagnose child abuse, determines the outcome. 13 Lastly, we did not calculate the necessary sample size prior to conducting this study.
Future Perspectives
We would like to point out some important priorities for the improvement of the detection of child abuse at the ED in low- and middle-income countries. First of all, the education of healthcare professionals needs to focus more on child abuse, red flags of child abuse and how to act when you suspect child abuse. This will make the healthcare professionals presumably more confident and aware. 12 Secondly, it is pivotal to have a dedicated multi-disciplinary team that can be consulted by healthcare professionals at the ED. An important person in this team should be a specialized “child abuse professional,” who works at the ED and can monitor the admitted children, can be consulted by ED nurses and doctors at the ED and who can help to screen for child abuse. Last important issue is to have an organized safety net for children who have been abused. A national CPS organization is pivotal for the safety of the children and monitoring of their safety after hospital discharge. Interesting to investigate in the future is to interview the healthcare professionals and ask them about their experiences regarding working with the screening. Important to know is whether they understood how to complete the screening, how did they experience the implementation process and is there a sufficient follow-up system available? This information can be used for the implementation of the screening in other middle-income countries.
Conclusion
The implementation of a systematic screening at the emergency department of the Academic Hospital Paramaribo of Suriname yielded an improvement in the detection of child abuse cases. Even though the screening showed different outcomes compared to the implementation in high income countries, it was valuable in a middle-income country as well. Some screening parts had a higher sensitivity and specificity in Suriname compared to European countries. Future policy should focus on education on child abuse, provide continuous consultation of a multidisciplinary team who can assess suspected child abuse cases and the improvement of a safety net after hospital discharge. Especially interesting for middle- and low-income countries is that the detection of child abuse increases significantly, by using an “easy-to-use” screening instrument.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241245274 – Supplemental material for Screening for Child Abuse in the Emergency Department of Academic Hospital Paramaribo in Suriname
Supplemental material, sj-docx-1-gph-10.1177_2333794X241245274 for Screening for Child Abuse in the Emergency Department of Academic Hospital Paramaribo in Suriname by Eeftinck Schattenkerk, LD, Loos MHJ, Schouten MCM, Cheuk-Alam I, Bakx R and Lissone NPA in Global Pediatric Health
Footnotes
Acknowledgements
Doctor M.C. Rodriquez, doctor R. Wolf, the Louise Vehmeijer foundation.
Author’s contribution
Dr. Loos conceptualized and designed the study and data collection instruments, carried out analyses, drafted the initial manuscript and reviewed and revised the manuscript.
Dr. Eeftinck Schattenkerk implemented the screening at the AZP, collected data, carried out analyses and reviewed and revised the manuscript.
Dr. Cheuk-Alam collected data and reviewed the manuscript for important intellectual content.
Dr. Bakx conceptualized and designed the study, and critically reviewed the manuscript for important intellectual content.
Dr. Lissone and Dr. Schouten coordinated and supervised data collection at the AZP, and critically reviewed the manuscript for important intellectual content.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All phases of this study were supported by the “Louise Vehmeijer” foundation, Stadionweg 9, 1077 RV Amsterdam, the Netherlands. Funding reference number 2016-007V.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.