
Abstract
Background. The Dutch guideline Eating Disorders defines admission criteria for children with anorexia nervosa (AN) in need for medical stabilization and advices close monitoring to detect refeeding syndrome (RFS) in an early stage. Methods. Admission criteria, recommendations at admission, and during first week of hospitalization were evaluated in accordance to the guideline. RFS was defined as decreased electrolyte concentrations and/or clinical features. Results. 22 patients were included with a total of 50 admissions. We observed that 62% of the admitted patients met one of the admission criteria, 190/300 (63%) recommended admission examinations were performed. During admission adherence decreased, in particular daily weighing and physical examination (12% and 6%, respectively). The guideline was not fully followed in any of the patients. None of the hospitalized patients met the RFS criteria. Conclusion. Guideline adherence was moderate and can be improved by a few adaptations, which may limit unnecessary laboratory testing.
Introduction
Anorexia nervosa (AN) is defined as a psychiatric disorder characterized by severe disturbances in eating behaviors and excessive concern with body weight and shape. 1 The main characteristics of the disease are presence of significant weight loss due to voluntary dietary restrictions associated with a fear of gaining weight and a refusal to maintain minimum body weight within indicated ranges. 1 Hospitalization for anorexia may be required in case of severe psychiatric condition and/or suicide risk or in case for medical stabilization of the physical consequences of AN due to starvation and compensatory behavior like purging and excessive exercise.
During hospitalization for medical stabilization, one of the physically most challenging phases is the refeeding period. Phosphate and thiamine are essential for glucose metabolism, and are rapidly used during this process.2,3 The shift to glucose metabolism during refeeding results in a high demand for the production of phosphorylated intermediates for glycolysis, the Krebs cycle, and the electron transport chain to form adenosine triphosphate and 2,3-diphosphoglycerate, resulting in a reduction in serum phosphate concentrations. This increased utilization of phosphate and subsequent reduction in serum concentrations can lead to arrhythmias, seizures, cardiac failure, respiratory failure, rhabdomyolysis, coma, and sudden death—collectively known as the refeeding syndrome (RFS), a physiological phenomenon that occurs while refeeding the undernourished patient, a process driven by insulin.4,5 Hypophosphatemia is the most consistently reported biochemical disturbance seen in the RFS.6,7 However, the syndrome is complex and may also feature abnormal sodium and fluid balance; changes in glucose, protein, and fat metabolism; thiamine deficiency; hypokalemia; and hypomagnesemia as a result from hormonal and metabolic changes. 8 The reported incidence of RFS varies from 0% to 48% with an average incidence of 14 %. 9
In 2017 the updated Dutch national guideline Eating Disorders was published. 10 In this guideline admission criteria for children with AN in need for medical stabilization are defined. During hospitalization weight restoration with a high calorie intake is initiated. The guideline advices close monitoring including frequent physical examination and laboratory testing during the first week of refeeding to detect RFS in an early stage. However, it is unknown if, and how often RFS occurs if this guideline is followed in non-academic general hospitals. Therefore, we determined the adherence to the guideline and the incidence of RFS in hospitalized adolescents in a non-academic teaching hospital.
Methods
Study Design and Participants
A single center, retrospective, cohort study was conducted. Patients meeting the DSM-5 criteria for AN, 1 with an age between 12 and 18 years old, and hospitalized, between January 2018 and December 2021 were included. The exclusion criteria were patients transferred from and to other hospitals.
Guideline
The guideline for Eating Disorders recommends that during initial presentation the patient history is documented, including minimum and maximum weight in recent years and the weight progression over time related to growth. 10 Height, weight, blood pressure, and pulse are recorded. Physical examination is performed with special attention to signs of malnutrition. Criteria for hospital admission are formulated, and these include arrhythmias, severe hypotension, orthostasis, dehydration, severe malnutrition, severe electrolyte disturbances, hypoglycemia, and hypothermia.
In order to prevent RFS, it’s recommended to start with a caloric intake of 40 to 60 kcal/kg of the current body weight. Monitoring for RFS consists of blood tests at admission, daily physical examination, including heart rate and blood pressure, and 3 times a week additional blood tests (creatinine, urea, phosphate, potassium, magnesium, glucose, capillary blood gas) and once per week a complete blood cell count and liver transaminases, and depending on symptoms more frequently.
Phosphate supplementation is given on a temporary basis, especially in the case of low or rapidly falling phosphate due to refeeding or at the start of refeeding, preferably oral approximately 1 mmol/kg/day. Consideration may be given to supplementation of thiamine (vitamin B1). There is no consensus on the optimal thiamine dosage. If the patient shows signs of RFS, the energy and fluid intake is adjusted and symptoms should be treated appropriately.
Data Collection and Definitions
The total number of hospital admissions per patient was determined during the study period. Re-admissions within 5 days of the previous admission were excluded. Per admission demographic data, physical examination results and laboratory results were collected from the medical health charts.
Adherence to the guideline was divided in 3 parts. First, we determined if hospitalization was in line with the recommended admission criteria. Second, we determined if the 6 recommendations at admission (heart rate, blood pressure, weight, temperature, glucose, and electrolytes) were performed. Third, we determined if the 3 recommendations (blood tests 3 times a week, weight daily, physical examination daily) were performed during the first week of hospitalization. The adherence to the guideline was determined based on the total number of admissions.
RFS was defined as: (1) severely low electrolytes concentrations, including Potassium <2.5mmol/L, Phosphate <0.32mmol/L, Magnesium <0.5mmol/L; (2) peripheral edema or acute circulatory fluid overload; (3) organ dysfunction; (4) and not all features need to be present.6,7
To determine the incidence of RFS we searched for the number of cases of hypophosphatemia, hypokalemia, and hypomagnesemia at the day of admission, at 24 and 72 hours and after 7 days. If a patient was discharged before day 7, we checked if blood test were done 7 days after admission at the outpatient clinic department. Hypophosphatemia was defined based on the CALIPER database. We also examined medical records for clinical manifestations of RFS. The incidence of RFS was determined based on the total number of admissions.
Data Analysis
Statistical analyses were performed using SPSS Statistics, version 26 (IBM Corp.). A P-value of <.05 was considered as statistically significant.
Ethical statement: The study was approved by the Medical Ethical Review Committee of the Tergooi MC (V.34.61) and was not subjected to the Medical Research Involving Human Subject Act and written informed consent was waived by the Committee (letter 22.008 nWMO anorexia). The data was anonymized using Castor Electronic Data Management System and complied with the General Data Protection Regulation.
Results
During the study period 22 patients were included with a total of 50 admissions. The mean days of admissions was 9.5 (range 1-32 days, SD 7.6) (Table 1). Of these 22 patients, 20 (90.9%) were female. Mean age was 15.1 year (range 12-17 years), weight 47.7 ± 8.5 kg and body mass index 16.7 ± 2.4 kg/m2. Seven (31.8%) adolescents were known with one or more psychiatric comorbidities, including autism, depression, attention deficit hyperactive disorder, posttraumatic stress disorder, anxiety and panic disorder, and personality disorder.
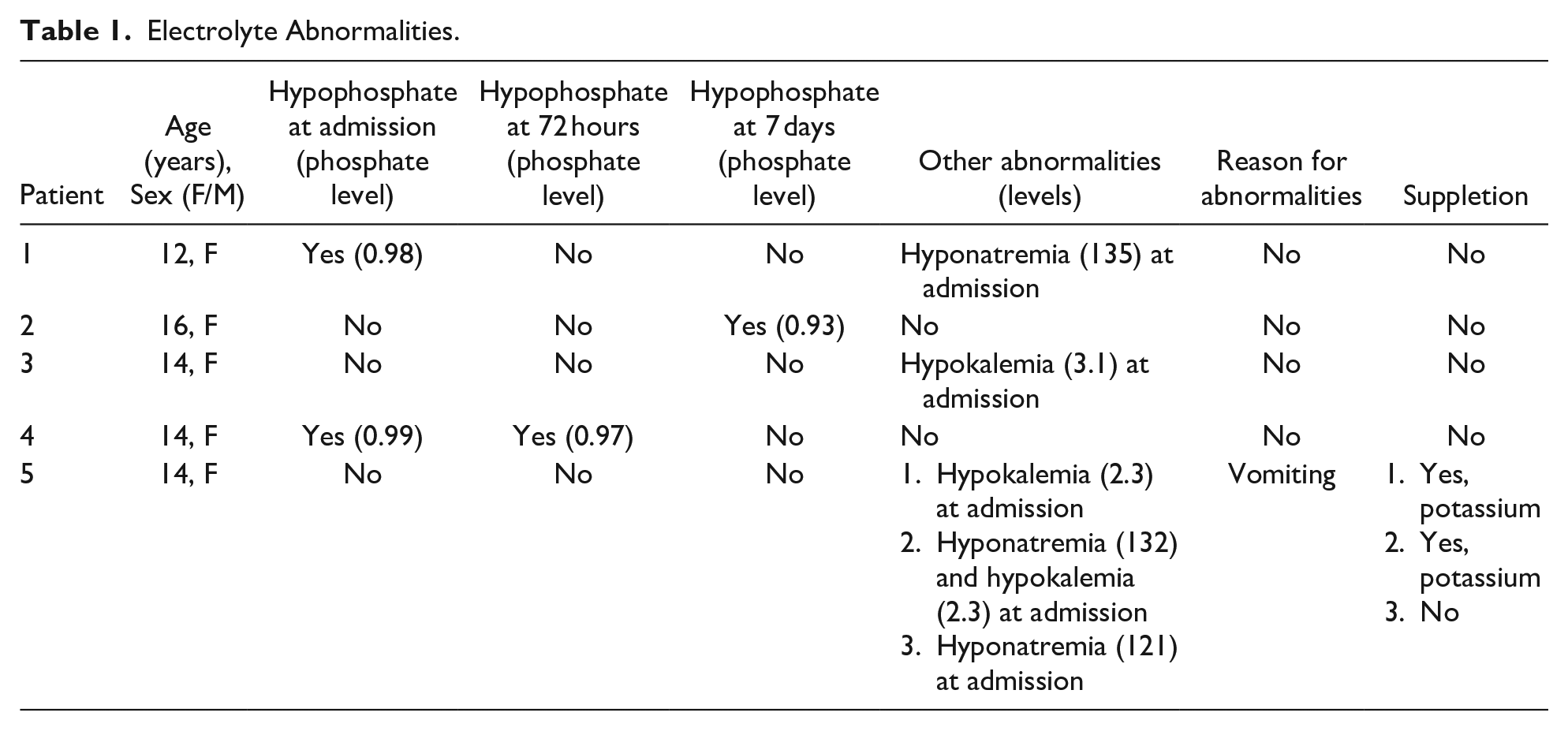
Electrolyte Abnormalities.
Adherence to Guideline
Reasons for admission: We observed that 38% of the admitted patients did not meet one of the admission criteria, of whom 9/50 (18%) were considered somatically threatened according to the treating physician but not further specified and in 10/50 (20%) reason for admission was not specified.
Recommendations at admission: The guideline recommends to perform 6 measurements at admission, hence for the 50 included admission a maximum of 300 recommendations. We found that 190 of the 300 (63%) admission recommendations were performed, namely in 42/50 (84%) for heart rate, 46/50 (92%) for glucose, 40 (80%) for electrolytes, 13 (26%) for blood pressure, 6 (12%) for temperature, and 43 (86%) for weight recording, respectively. In only 4 (8%) admission all recommendations were performed and documented. Temperature and blood pressure were often not performed.
Recommendations during first week of hospitalization: The adherence decreased during the admission. Blood test after 72 hours were most often done in accordance with protocol (66%), three times a week (38%) and after 7 days (22%), respectively. Daily weighing (12%) and daily physical examination (6%) were rarely performed. Consequently, in none of the patients the protocol was completely followed.
Incidence of Refeeding
A total of 8 mild electrolyte abnormalities were present: 6 at admission, one at 72 hours, and one at 7 days (Table 1). None of the electrolyte abnormalities fulfilled the RFS criteria according to the definitions. None of the patients received phosphate supplementation. There were no clinical symptoms of RFS reported.
Discussion
In this retrospective study, the adherence to the guideline in hospitalized AN patients, was moderate. Although one of the goals of the guideline is to detect RFS in an early stage, we did not identify patients meeting the criteria for RFS.
The moderate guideline adherence in our study is in line to adherence to other Dutch pediatric care guidelines, including those for early onset neonatal sepsis, traumatic brain injury, fever without apparent source, and functional abdominal pain.11-15 Reasons for moderate adherence to guidelines can be explained in terms of both the users and the guideline. In this study we observed that adherence to admission criteria were low, which may indicate that clinician’s decided to hospitalize these adolescents for other reasons than strictly medical stabilization. Particular around the COVID pandemic admission rates increased significantly. For example, a highly significant increase of 40% in admission rates has been described in Germany for female children’s and adolescents’ between the pre-COVID-19 and peri-COVID-19 periods in 2019 and 2021, respectively. 16 A number of these adolescents were not always in need for medical stabilization as shown that weight of the patients at admission was higher during the COVID-19 period and fewer patients had clinical signs typical of AN upon physical examination. 17 Furthermore, adherence to perform blood tests over time decreased as well, which may be attributed that the patients did not develop signs of RFS, and that clinician’s considered these recommendations to strict.
A second finding of our study was that we did not identify any case RFS case. Various reasons may contribute to this finding. The RFS incidence may be under estimated due to a number of reasons. First, 38% of the patients that were admitted to the hospital did not meet one of the admission criteria. These patients were admitted based on the clinical judgement of the treating pediatricians or based on other non-physical reasons like social circumstances. Although variation in admission criteria have been reported, it remains questionable whether these patients were in need for refeeding and were at risk for RFS. 10 Second, the adherence to the guideline was poor and decreased during hospitalization. One can discuss that, we may have missed mild clinical signs of RFS as physical exams were not performed daily and missed hypophosphatemia as blood test were not performed as recommended. On the other hand, RFS occurs mainly in the first 1 to 5 days of hospitalization, so it is not surprising that guideline compliance decreased during hospitalization, especially when there were no signs of RFS during the first week of admission. Third, less likely, it could be that some patients were discharged while still being catabolic. Fourth, to determine the incidence of RFS in the hospitalized patients we applied the most commonly used and accepted definition based on a combination of severe electrolyte disturbances and/or clinical features.6,7 These criteria may be too strict for this population. The incidence could have been higher if other RFS definitions were used. Definitions of RFS are highly heterogeneous among studies, with some studies only relying on electrolyte disturbances with different cut-offs, and others also integrating clinical parameters. This also explains the large variation in reported RFS incidence rates of 0% to 48%. 9
The current study provides baseline data to identify areas for improvement in our care of adolescents requiring inpatient medical stabilization for AN. Specific areas for improvement include to decrease the number of laboratory testing during hospitalization. First, if an adolescent is hospitalized for other reasons than medical stabilization, routine laboratory testing during the time of admission can be withheld. Second, for those adolescents hospitalized for medical stabilization, given the low incidence of RFS, we suggest that if laboratory results are normal after 72 hours, no further blood test are needed in a patient who is clearly refed. It is, however, recommended that physical examination and weight measurement, for example 3 times a week during hospitalization, is mandatory. In case of weight loss or signs of persistent catabolic state blood test can be repeated on individual basis instead of routine testing. Before start of refeeding it is also mandatory that the risk for RFS at start of refeeding is estimated based on objective parameters. We think adherence to the guideline can be increased by making these adaptations to the guideline for this population.
We acknowledge that this study has some limitations, including a relatively small sample size. We did not perform a sample size calculation for detecting RFS. Although, we do not think that a larger sample size changes the outcome of our results, it could help to underscore our conclusions. In addition, due to the retrospective nature of this study, we had to rely on the accurate recordkeeping by the medical staff, which may give a bias. Finally, we did not evaluate the reasons why the guideline was not followed. The strengths of this study that it is performed in a non-academic large teaching hospital and our results may be used to make adaptations to the guideline for this specific population to decrease unnecessary laboratory testing.
Conclusion
We found a moderate guideline adherence in hospitalized adolescents with AN in need for medical stabilization in a general hospital. Reasons for this moderate adherence include that the current guideline recommends often laboratory testing to detect RFS despite that the incidence of RFS in this population is very low. We provided suggestions to decrease the number of laboratory testing, which may help to increase adherence to the guideline.
Footnotes
Author Contributions
All authors contributed to the study conception and design. Data collection and analysis were performed by IB. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The study was approved by the Medical Ethical Review Committee of the Tergooi MC (V.34.61) and was not subjected to the Medical Research Involving Human Subject Act. The data was anonymized using Castor Electronic Data Management System and complied with the General Data Protection Regulation.
Informed Consent
Not applicable