
Abstract
Objectives. We investigated the challenges faced by mothers of preterm babies practicing KMC during the Covid-19 pandemic and documented the mothers’ suggestions of possible interventions. Methods. We conducted a cross-sectional descriptive study at the New Born Unit of Kenyatta National Hospital(KNH). We interviewed 82 mothers using a researcher-administered questionnaire with closed and open-ended questions. Qualitative data generated from open-ended questions was analyzed thematically. Results. KMC was majorly affected by; fear of the baby contracting COVID-19, fear of contracting COVID-19, and social distancing restrictions. The mothers’ suggested interventions included; the need for more KMC rooms, provision of appropriate clothing, strict application of COVID-19 prevention guidelines, and greater support of practice by the family. Conclusion. The mother’s pivotal role as a partner in decision-making in regard to the improvement of KMC during pandemics and possibly other settings was demonstrated. Targeted interventions should incorporate the suggestions from the mothers.
Background
Kangaroo Mother Care (KMC) is an effective intervention1 -3 that has been shown to improve health outcomes for premature and low birth weight infants, especially in low-resource settings. Effective KMC demands undivided support from family and healthcare systems. 4 The positive impact of KMC practice in Covid-19 has been demonstrated.5,6 However, the COVID-19 pandemic presented significant challenges in the practice of KMC in all settings including Kenya. By 21 September 2021, Kenya had reported 246 956 COVID-19 cases cumulatively with 5008 deaths depicting a case-fatality rate of 2.02%. The highest wave of Covid-19 cases in Kenya was reported in December 2021 with an average of 2400 cases a day. 7
Mothers in low-resource settings in Sub-Saharan Africa have faced several challenges in practicing KMC during the COVID-19 pandemic. These challenges include fear of exposure of babies to infection, lack of support from healthcare providers, inadequate facilities for KMC, and misinformation about COVID-19 among others.8,9 Additionally, inadequate supplies of essential items for KMC, such as kangaroo wraps and private spaces for breastfeeding, hindered the implementation of KMC in hospitals.
In Kenya, institutional studies found that KMC services were disrupted during the pandemic due to reduced staffing and limited availability of personal protective equipment. 10 In addition, fear of COVID-19 transmission led to decreased utilization of KMC services by mothers and families.
In their course of practice, the research team noted a significant decline in the number of postnatal mothers of premature infants practicing kangaroo mother care in the Newborn Unit of KNH. This was further supported by the facility’s postnatal care review records, which indicated that the number of postnatal mothers of preterms practicing continuous KMC at KNH had dropped by >70% since the start of the pandemic. 11 Few studies have explored the effect of Covid-19 among mothers practicing KMC particularly in low- and middle-income countries with reports of reduction in KMC practices in limited resource settings.10,12
Studies that aimed at improving the quality of KMC and overcoming barriers to KMC during the pandemic period found that homegrown solutions and strategies by mothers and healthcare workers could have more ownership and are likely to be more sustainable.13,14 Partners and family members often play a big role in decision-making regarding KMC. 8 Even though studies done at the community level among men, pregnant and lactating mothers as well as health care workers reported myths including ideation that Covid-19 did not exist and was a creation of the government 15 with another reporting low Covid-19 risk perception 16 the role of partner support on the influence of KMC at the institutional level cannot be overlooked.
The voice of the mothers in seeking possible solutions in these settings could be key to the success of KMC. By identifying the challenges faced by the mothers practicing KMC during Covid-19 as well as incorporating their suggestions in addressing the challenges, there can be continued support for the implementation of KMC and improve outcomes for vulnerable infants in low-resource settings during the COVID-19 pandemic and beyond.
Our study therefore aimed at gaining insights from mothers practicing KMC at KNH newborn unit in regards to their experiences and challenges they faced as well as documenting their suggested solutions.
Methods
We conducted a cross-sectional mixed-method descriptive study among mothers of preterm babies at the newborn unit at KNH. Since Focus Group discussions could not be held due to Covid-19 challenges, data was collected using a researcher-administered questionnaire. The paper-based questionnaire contained both closed and open-ended questions. The questionnaire contained 3 sections; section A on demographic information of the mothers, Section B on factors affecting the mothers’ utilization of KMC during the Covid-19 pandemic, and section C captured the mothers’ suggestions to mitigate the reported challenges. The possible challenges identified by the mothers were categorized using a Likert scale, ranging from no extent 1 to a very great extent. 5 Section C contained open-ended questions that asked mothers to propose possible ways of dealing with the reported challenges. This generated the qualitative data used in this study. The responses from the mothers on possible interventions to foster KMC practice during the Covid-19 pandemic were captured verbatim and texts were recorded in the questionnaire. The study tools were translated into Swahili, the National language to ensure that all eligible mothers participated regardless of their literacy levels. We pretested the data collection tool among 10 mothers of preterm babies in the New Born Unit of the adjacent Mbagathi County referral hospital.
The study was done at the NBU of KNH. KNH is the largest National referral hospital in Kenya. It has a bed capacity of approximately 2500 with over 120% occupation on average. The hospital has 52 wards and several specialist clinics. Every month, the newborn unit(NBU) admits approximately 120 infants for KMC.
A consecutive sample size of 89 respondents was selected from a finite target population of 120 eligible mothers at NBU, KNH, assuming a 95% confidence interval and margin of error at 0.05.17 -19 Being A cross-sectional study with a finite population < 10 000 and with the prevalence of Kangaroo mother care is unavailable, therefore, an assumption of 50% prevalence for this study was adopted thus P = .5
We excluded teenage mothers, mothers who were too ill to respond to the questionnaire, and a few who could not converse in the Swahili language.
The respondents were given ample time to respond to the questions, as outlined in the study tools, without interfering with their responses. The responses were then read back to the mother and she was given an opportunity to recant any response or add any extra information. The session took an average of 30 to 40 minutes. The responses were documented in the questionnaire after which all questionnaires were scrutinized for completeness. The data collection exercise lasted 4 weeks from mid-October to mid-November 2021.
The research team familiarized themselves with the data collected every 2 days and spent time reviewing the data.
Data Analysis
We analyzed the texts embedded in the open-ended questions. The qualitative data generated were reported verbatim and texts were recorded into a Word document by research assistants. For quality control, the first and second authors reviewed the study tools for completeness and confirmed that the content of the manually filled qualitative data was a complete replica of the Word document. The first 2 authors took part in coding independently and where there was disparity a consensus was built. The coding was done manually so as to improve content coverage. 20 The qualitative data was analyzed thematically using content analysis and presented in prose form. 21 Thematic analysis was carried out by 3 independent transcribers and the converging themes from the 3 analysts were picked as the dominant ones that described the participants’ communication about the subject at hand.
Major and minor nodes were identified from the emerging themes with mothers differentiating them based on the perceived measure of effect on KMC practice. Where applicable, direct quotes from the respondents were captured. The quantitative data was analyzed using descriptive statistics and presented in percentages.
Results
A total of 82 mothers completed the questionnaire of the initial 89 who were recruited giving a response rate of 92%. Seven mothers dropped out of the study as they reported general exhaustion.
The demographic characterization showed that majority were aged between 18 and 39 years; had attained basic education level (Secondary − 48.8%; Tertiary − 39%); most were married (76.8%, n = 63); had between 1 and 3 children (90.2%, n = 74); were Christians (92.7%, n = 76); did not have any pre-existing illness during their pregnancy (76.8%, n = 63) and were currently practicing kangaroo mother care for their babies (75.6%, n = 62).
The respondents were asked to subjectively report the extent that the identified challenges affected their performance of KMC and were asked to suggest possible mitigation measures. The responses were summarized in Table 1 which shows the frequency distribution of the responses for each factor affecting the implementation of Kangaroo Mother Care (KMC) during the COVID-19 pandemic.
The Challenges Faced by the Mothers in Practicing KMC at KNH New Born Unit During Covid-19 Pandemic Period and the Perceived Impact.

Other factors cited by the mothers as impeding their utilization of kangaroo mother care during the ongoing Covid-19 pandemic included lack of KMC-appropriate clothes for the baby such as wrappers, locally referred to as “lessos” (45.1%, n = 37); inadequate KMC rooms/spaces especially in light of the social distancing requirement for Covid-19 transmission prevention (65.9%, n = 54); limited time allocated for performing KMC (51.2%, n = 42); sitting chairs being uncomfortable (36.6%, n = 30); KMC rooms being located far from the nursery (14.6%, n = 12); security concerns at night (20.7%, n = 17); general body exhaustion among the mothers (34.1%, n = 28); infant being unwell (25.6%, n = 21) and lack of support from spouses/significant others with respect to the practice of KMC (72%, n = 59).
Thematic Analysis of Suggested Interventions to Foster the Mothers’ Practice of KMC During the Covid-19 Pandemic
The study sought to identify possible interventions to foster the postnatal mothers’ kangaroo mother care practice during the Covid-19 pandemic period and the mothers were requested to offer their suggestions on the same. From the responses to the open-ended questions, data saturation was achieved with the 26 interviews. The average response length was 22 words. Four major themes emanated from the mothers’ responses regarding possible interventions to enhance their practice of KMC during the ongoing Covid-19 pandemic. The 4 themes were; the need for more KMC rooms, the provision of KMC-appropriate clothing, the need for strict application of Covid-19 prevention guidelines, and the need for greater support of KMC practice from the family. Stratification of mothers was deemed unnecessary, as the responses exhibited a notable similarity across all respondents
A number of suggestions were captured verbatim from respondents and outlined as follows and further illustrated in Table 2;
Thematic Analysis of Suggested Interventions to Foster the Mothers’ Practice of KMC During the Covid-19 Pandemic at KNH.
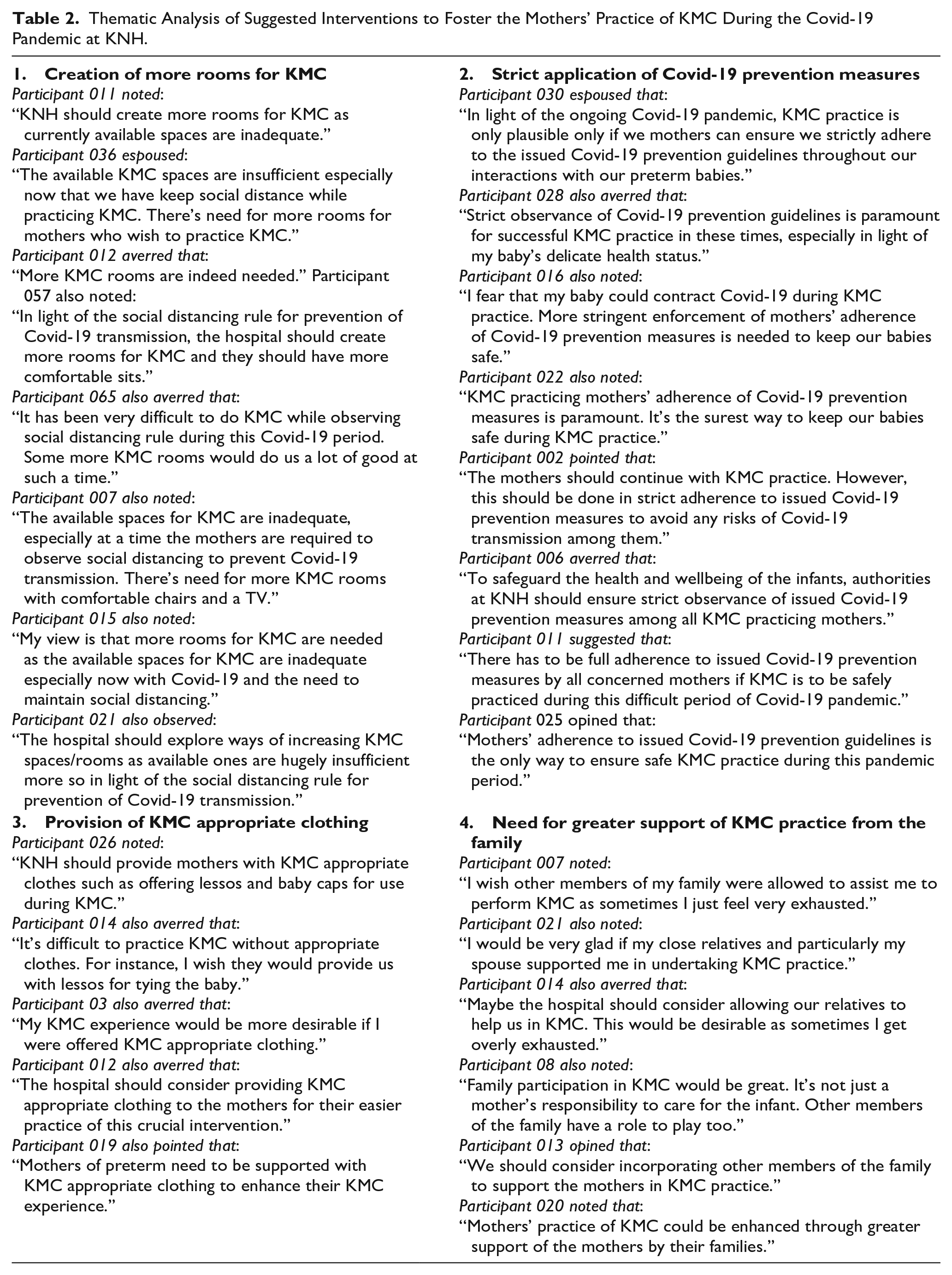
Theme 1: Creation of More Rooms for KMC
There was a shared view among most of the mothers that available KMC rooms at KNH were inadequate and hence most of the mothers were in agreement that there was a need for the creation of more KMC rooms to meet an already existing need. This is as captured in the following few verbatim excerpts;
“It has been very difficult to do KMC while observing social distancing-rule during this Covid-19 period. Some more KMC rooms would do us a lot of good at such a time.”
Theme 2: Provision of KMC-Appropriate Clothing
In view of identified challenges relating to the inadequacy of appropriate KMC clothing among the mothers of pre-terms at KNH, the mothers shared the view that their KMC practice, during the ongoing Covid-19 pandemic, would be enhanced if they were provided with sufficient appropriate KMC clothing, as depicted in the following few verbatim excerpts;
“Kenyatta should provide mothers with KMC appropriate clothes such as offering lessons and baby caps for use during KMC.”
“It’s difficult to practice KMC without appropriate clothes. For instance, I wish they would provide us with lessos for tying the baby.”
It is to be noted that during the pandemic period, mothers were encouraged to use clothes provided by the hospital as these were considered to be safer in comparison to personal complementary clothing that mothers could previously be allowed to bring to the hospital.
Theme 3: Strict Application of Covid-19 Prevention Measures
In response to identified concerns shared by the mothers of the pre-terms regarding KMC practice during the ongoing Covid-19 pandemic, the mothers shared a common belief that strict adherence of prescribed Covid-19 transmission prevention guidelines was instrumental for their safe practice of KMC during the ongoing pandemic. It is noted that mothers felt that some of their colleagues were reluctant to follow the advice on physical distancing seriously. This is further illustrated in the following few verbatim excerpts; “Strict observance of Covid-19 prevention guidelines is paramount for successful KMC practice in these times, especially in light of my baby’s delicate health status.”
While a 38-year-old mother reiterated the concern and stated “I fear that my baby could contract Covid-19 during KMC practice. More stringent enforcement of mothers’ adherence of Covid-19 prevention measures is needed to keep our babies safe.”
Theme 4: Need for Greater Support for KMC Practice From the Family
We established that the mothers felt that their KMC practice would be enhanced by greater support for this important intervention from their families. In short, KMC practice should not be perceived as the mothers’ responsibility only but that even their immediate families had a role to play by offering support to the mothers. This is as depicted in the following few verbatim excerpts; “I wish other members of my family were allowed to assist me to perform KMC as sometimes I just feel very exhausted.”
While a 21-year-old mother noted; “Maybe the hospital should consider allowing our relatives to help us in KMC. This would be desirable as sometimes I get overly exhausted.”
It is to be noted that KNH had a “no-visitor” policy at the height of the pandemic, the period during which the study was carried out. Visitors could only be allowed in only when summoned by the hospital management and they majorly played the role of clearing the hospital bills and discharge of patients.
Discussion
In this study, we aimed at establishing the challenges faced by mothers in regard to practice of KMC at KNH and captured the suggestions of mothers on how the challenges could be addressed. The major challenges highlighted by mothers include; fear of the baby and mothers contracting Covid-19, social distancing restrictions, and financial barriers related to families’ economic shocks due to Covid-19 related loss of livelihood. Other challenges that were linked to the Covid-19 pandemic included; restriction of physical movement, low awareness about Covid-19 and mixed messages on transmission. These challenges were unique to the Covid-19 pandemic.
The understanding of Covid-19 spread caused a lot of fear and families desired to minimize any unnecessary exposure to the newborn babies. They opted to keep away resulting to mothers remaining lonely in the facilities with less support from the health care providers due to small numbers per shift. Previously existing challenges such as lack of support from family, personal stress, and lack of support from healthcare workers were highlighted. The hospital policy of no visitors exacerbated the feeling of lack of support from significant others. Additionally, reported factors like conflicting instructions against KMC from healthcare workers, low healthcare staff availability, and overwhelmed congested health facilities were reported as bottlenecks exacerbated by Covid-19. The factors identified were consistent with the challenges faced by health systems globally during the pandemic, including restrictions on physical movement, communication challenges, and shortage of healthcare workers. 22 We noted that approximately 8.6% reported that instruction against KMC by Health care workers had a great extent to very great extent influence on the practice of KMC. This is an indication of the possibility of a percentage of HCWs having contrary beliefs regarding KMC during the Covid-19 pandemic. This phenomenon could need further exploration as 10 instructions against KMC from healthcare workers may have led to reduced individual support offered to mothers thus affecting the quality of KMC provided to their infants during the pandemic.
The study also identified other unique factors that impeded the utilization of KMC during the COVID-19 pandemic specifically at KNH, including, uncomfortable sitting chairs, which may have contributed to general body exhaustion as well as security concerns at night since mothers resided in a hostel one floor below the NBU. The movement from the hostel to the NBU especially at night may be a daunting task. Although the hospital endeavors to provide night guards, mothers generally prefer walking in groups for security reasons. The findings of our study support previous research that has highlighted the importance of addressing structural barriers and environmental factors in promoting the adoption and sustainability of KMC in low-resource settings.7,23,24 The findings from our study highlighted potential solutions suggested by the mothers with the hope of overcoming such identified challenges. One of the major themes that emerged from reported solutions was the need for more KMC rooms. This is consistent with findings from other studies done in low-resource settings such as Malawi, where inadequate space for KMC was reported as a major challenge by mothers.25,26 The KMC rooms should be well equipped with facilities such as private spaces for breastfeeding, handwashing facilities, and PPE for healthcare workers.3,27 Improving the infrastructure and KMC facilities in hospitals is also crucial to support KMC implementation in low-resource settings. Creating more KMC rooms could improve the quality of KMC for infants and ensure that they can practice KMC in a safe and comfortable environment. KNH could consider implementing suggestions from the mothers as a recent study done in Zambia revealed that improvement in the setting of a number of KMC rooms improved infant outcomes. 28
Another theme that emerged was the need for appropriate KMC clothing. This observation is also consistent with other studies that have highlighted the importance of providing appropriate clothing for mothers practicing KMC 23 as well as a comfortable environment. 28 Inadequate clothing can make it difficult for mothers to practice KMC effectively and comfortably, which can negatively impact the health of the preterm baby.
Strict adherence to Covid-19 prevention measures was also identified as a key factor for safe KMC practice during the pandemic. While there may have been few healthcare providers to oversee strict adherence to the Covid-19 protocol, some mothers may have not been keen on following the same, contributing to concern from fellow mothers. This finding is supported by other studies that have highlighted the importance of Covid-19 prevention measures in KMC practice 14 Adherence to these measures could help to prevent the spread of Covid-19 and ensure that mothers and preterm babies remain safe. Appointing enthusiastic mothers as KMC leaders in such settings has been shown to be effective in motivating and monitoring other mothers. 14
Our study implores that greater support from family members is needed for successful KMC practice. This finding is consistent with other studies that have identified family support as a key factor in the successful implementation of KMC 29 but contradicted a previous study that was done in the same institution prior to Covid-19 in which mothers reported support from family members. 24 Family support can help to reduce the burden on mothers and ensure that they have the necessary support to practice KMC effectively during Covid-19.To ensure the effectiveness of this support, it is essential to debunk myths surrounding Covid-19, such as the unfounded belief that it is a creation of the government and the misconception that it is not a reality among men, pregnant women, and lactating mothers. 15 It is worthwhile noting the shift of concerns of the mothers from a prior study where mothers recommended for provision of entertainment, review meal time and having a healthcare workers in the KMC room as interventions to improve practice of KMC prior to Covid-19. 24
Study Limitation
Generalization of these findings should be taken cautiously as the study was undertaken in a single-site referral health facility. Qualitative data collection is subjective and at the same time manual coding of qualitative data may have introduced the underlying researcher’s personal influence on interpretation of data. Human error in the documentation of qualitative data by research assistants was also a possibility Anxiety among mothers may have influenced their responses. There was no intergroup analysis in this study, an area that needs further exploration
Conclusion
This study sheds light on the dilemmas arising from the fear of Covid-19 exposure for all involved in preterm infant care, emphasizing heightened anxiety among mothers in newborn units due to uncertainties and lack of preparedness during the pandemic’s peak. These mothers lacked typical family support and limited direct contact with healthcare workers to reduce infection risks for both themselves and the infants. Consequently, they grappled with uncertainties about caring for their preterm infants while navigating the necessity of social distancing to minimize Covid-19 exposure. The disruptive nature of Covid-19 was underscored, emphasizing the critical need for preparedness in managing future infectious epidemics within similar healthcare settings.
Furthermore, the study highlights the key challenges faced by mothers practicing Kangaroo Mother Care (KMC) during the ongoing Covid-19 pandemic, offering potential solutions to overcome these hurdles. It emphasizes the importance of prioritizing the creation of adequate KMC rooms, providing appropriate KMC clothing, strictly adhering to Covid-19 prevention measures, and garnering greater support from significant others to ensure effective KMC practice in low-resource settings. This reiterates the call for institutional frameworks and strengthened health systems in KMC in East Africa. 27 By addressing these challenges, hospitals can ensure that mothers in low-resource settings access quality KMC services during the Covid-19 pandemic and related emergencies. The study’s findings can inform interventions and preparedness strategies needed to uphold the practice of KMC during pandemics and other emergencies.
Importantly, this study highlights the mother’s pivotal role as a decision-making partner in improving KMC during pandemics and possibly other settings. Further research is needed to establish the practical implementation of the recommended interventions.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X231213472 – Supplemental material for Challenges Faced by Mothers Practicing Kangaroo Mother Care (KMC) in a Resource-Limited Setting During the COVID-19 Pandemic: Insights From the Voices of Mothers of Preterm Babies and Their Suggested Solutions
Supplemental material, sj-docx-1-gph-10.1177_2333794X231213472 for Challenges Faced by Mothers Practicing Kangaroo Mother Care (KMC) in a Resource-Limited Setting During the COVID-19 Pandemic: Insights From the Voices of Mothers of Preterm Babies and Their Suggested Solutions by Beatrice Afande Mukhola, Lucy W. Kivuti-Bitok and Angeline Chepchirchir in Global Pediatric Health
Footnotes
Acknowledgements
We thank all the mothers who took the time to share their experiences.
Author Contributions
BAM: Contributed to conception and design; Contributed to analysis; Drafted the manuscript;critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. LWK-B: Contributed to conception and design;Contributed to analysis; Drafted the manuscript;critically revised the manuscript;Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. AC: Contributed to conception and design; Contributed to analysis; Drafted the manuscript;critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical clearance was obtained from the Kenyatta National Hospital/University of Nairobi ethics and review committee(P372/05/2021) while permission was granted by the KNH administration who issued a study registration certificate. Written Informed consent was obtained from the mothers. We included mothers whose preterm babies had been admitted to the Newborn Unit for over 48 hours. This time frame allowed mothers to be a bit settled and had an opportunity to visit the NBU. Mothers were allowed to drop off at any point of the study without repercussions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.