
Abstract
Background. Neonatal hypothermia remains a challenge in resource-limited settings. Methods. We conducted a prospective mixed-methods cohort study in rural Rwandan health centers to assess the performance of an infant warmer we designed for low-resource settings. All hypothermic infants were eligible for enrollment. Outcomes. Safety: incidence of adverse reactions. Effectiveness: attainment of euthermia, rate of temperature rise. Feasibility: correct use of warmer, signs of wear. Interviews of caregivers and nurses. Findings. Of 102 encounters, there were no adverse reactions. Of 80 encounters for hypothermia when infants on warmer for ≥1 hour, 79 achieved euthermia; 73 in ≤2 hours. Of the 80 encounters, 64 had temperature rise ≥0.5°C/h. Of the 102 encounters, there were no instances of the warmer being prepared, used, or cleaned incorrectly. Five out of the 12 warmers exhibited wear. Interview participants were predominantly positive; some found time for readiness of warmer challenging. Interpretation. The warmer performed well. It is appropriate to study in larger scale.
Introduction
It is widely accepted that neonatal hypothermia remains an unsolved challenge that contributes to morbidity and mortality, especially in resource-limited settings.1-4 The prevalence of neonatal hypothermia ranges widely depending on the definition of hypothermia and the patient population assessed but was recently reported at 100% in a population of low-birth-weight (LBW) infants in 3 low-resource African settings.1,5 Those who are preterm, LBW, or ill are especially vulnerable to hypothermia. 6
Hypothermia can be prevented by providing a heat chain from the delivery room through interhospital/intrahospital transport to the neonatal ward. In high-income countries, this heat chain is highly reliant on radiant warmers and incubators.
In resource-limited settings where equipment, electricity, and training can be inconsistent at best, these electrical sources of external heat may be unavailable or misused resulting in high rates of hypothermia, as well as concerns regarding hyperthermia and infection control. The equipment is expensive, requires a consistent source of electricity, and the lifespan can be short without adequate infrastructure to address complex maintenance and repairs. While provision of a heat chain remains necessary, it requires adaptation based on available resources.
The World Health Organization’s global standard to provide external heat is continuous kangaroo mother care (KMC). KMC is a well-established, effective practice with many benefits beyond heat provision, including improved lactation and bonding.7-9 However, there are times when KMC does not provide enough heat, when it is not feasible due to illness of the mother or infant, or when the mother needs to take a break to pursue activities that are not compatible with KMC, such as bathing, cooking, or attending to other critical economic or social needs.10-18 In a trial of over 1500 mother/infant pairs, less than 25% practiced KMC for more than 7 h/day in the first 2 postpartum days, and from days 3 to 7 after birth, and the average was only 2.7 h/day. 19 Among the top 4 barriers to KMC cited by mothers in low- and middle-income countries were pain/fatigue.20-22
Other solutions currently available include hot water bottles, polyethylene wraps, bags, and mattresses filled with water, gels, or phase change materials (PCM). Each of these has major limitations related to safety, efficacy, and cost.23-26
Thus, there is an urgent need for an external heat source to complement KMC. A collaborative team including engineers from Lawrence Berkeley National Laboratory, subject matter experts from Boston Children’s Hospital, Rwandan clinicians from Partners In Health/Inshuti Mu Buzima, and leadership from the Rwandan Ministry of Health developed a warmer, designed specifically to address thermoregulation needs in the resource-limited setting. The infant warmer is a small mattress made of wax Phase Change Material (PCM) that turns from liquid to solid at skin temperature (37°C). 27 The PCM is melted by being placed in a thermos of boiled water for approximately 30 minutes. It is then slipped into an insulating sleeve where it stays at goal temperature (37°C) for approximately 6 hours. It is low cost, intuitive, reusable, and nonelectric. It can be used in the delivery room, neonatal ward, and on transport. The infant warmer can provide warmth when the patient is ill while still allowing easy accessibility for medical assessments and treatments. It is designed to be easily washable with standard hospital cleansers. Our goal, once the machine is manufactured, is that it lasts for 1000 uses and cost well under US$100.
The warmer performed well in a pilot study with 102 uses in 2 district hospitals in rural Rwanda. 27 Infants were eligible to use the warmer if they were hypothermic (temperature <36°C) or at risk of hypothermia (weight <2.5 kg) when KMC was not available. Hypothermia was prevented or corrected in 98% of uses. Mild hyperthermia was noted in 7% of uses. There were no other adverse events such as burns or rashes, and no instances in which the warmer was prepared, used, and cleaned incorrectly after only a brief training. Two out of 12 of the handmade prototype warmers demonstrated signs of wear and tear.
Based on this study, we conducted and report here the results of a second pilot study to assess the safety, effectiveness, and feasibility of the infant warmer in the health center setting where there is less consistent electricity, less support, and lower educational levels of the nurses. These infants are healthier than those in our previous study because sick babies born in health centers are transferred to a higher level of care, typically to a district hospital. We also included a qualitative interview of caregivers and nurses to assess acceptability of the warmer.
Methods
Study Design
We conducted a prospective mixed-methods cohort study in a purposeful sample at 6 health centers in rural Rwanda from February 2017 to May 2018. Health centers were selected to allow diversity in 2 aspects that could influence the results. First, ambient temperature: we selected half of the sites to be in a relatively warm region (Eastern province) and the other half in a relatively cold region (Northern province). Second, availability of electricity: within each district, we sampled sites both with and without electricity. Our quantitative goal was to assess the safety and effectiveness of the infant warmer based on clinical observation, and the feasibility of the warmer based on observer audits. Our qualitative goal was to understand the user experience with the warmer.
Quantitative Study
The study was conducted in 2 health centers in a relatively cool climate (median ambient air temperature 23.5°C (interquartile range [IQR] = 22.1-24.8) and 4 in a relatively warm climate (median air temperature 25.7°C [IQR = 24.8-26.45]). Of these 6 health centers, 5 have electricity; though an inconsistent supply, 3 have electric warmers.
The study nurse spent 2 hours training the clinical nursing staff at each health center in proper use of the infant warmer. She screened all infants on the postpartum unit for those who met study inclusion criteria without any exclusion criteria (Table 1). Infants were eligible for enrollment if they were hypothermic. Based on the Rwandan National Neonatal Protocols, hypothermia was defined as <36°C and euthermia as 36.5°C to 37.5°C. 28 Temperatures of 36.1°C to 36.4°C do not meet the definition of hypothermia but do not fall within the ideal euthermia range. The study nurse approached the parents of eligible infants for informed consent.
Inclusion, Exclusion, and Stop Criteria.
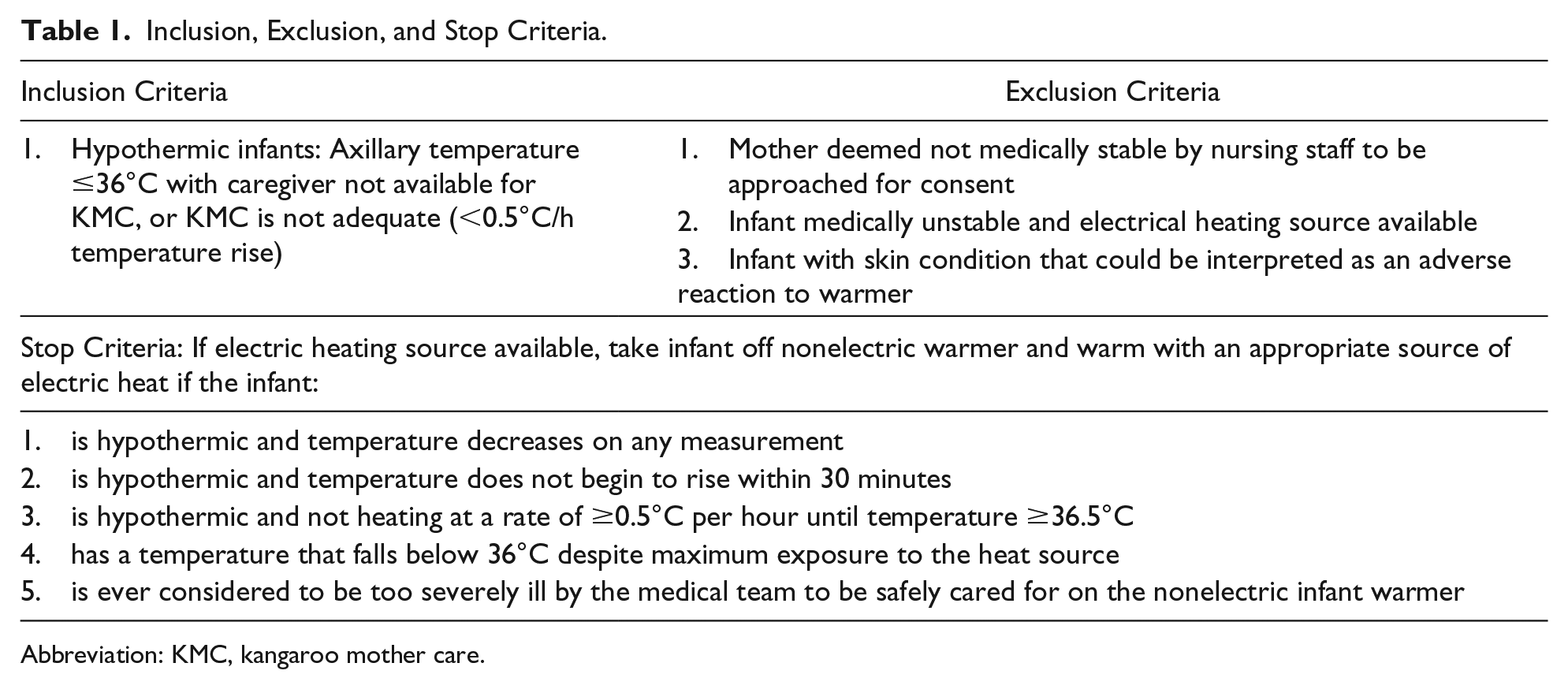
Abbreviation: KMC, kangaroo mother care.
The infant was then placed on the prepared warmer. Data were collected by the study nurse. Each time infants met the inclusion criteria, they were eligible to use the warmer. Therefore, a few infants participated in the study more than once; each time is referred to as an “encounter.” If the infant’s starting temperature was <35°C, the infant was placed on an electric warmer, if available, until the temperature reached 36°C, at which point the infant was placed on the nonelectric infant warmer in combination with KMC (Figure 1). If the mother was not available for KMC, the infant was placed directly on the warmer as a stand-alone heat source (Figure 1). After being placed in contact with the warmer, with or without KMC, the infant and warmer were then swaddled together in a blanket. The use of a hat with the warmer was encouraged. Infants only wore additional clothing by parental request, as it reduces heat transfer.

Infant warmer.
Temperature measurements of the infant, warmer, and ambient air were taken every 15 minutes for the first hour, then hourly, and as clinically indicated until the study ended. An infant who met “stop” criteria (Table 1) was removed from the warmer and offered an electric heat source, if available. Otherwise, the study was complete after 6 hours of warmer use, or when the warmer temperature fell below the effective temperature (<35°C) as indicated by the temperature indicator, or when the mother requested to discontinue use of the warmer, typically once the infant was euthermic and the mother wished to resume KMC.
A small group of infants were enrolled who needed neonatal resuscitation. To enroll these infants, the study nurse requested informed consent from laboring mothers and prepared the warmers. A newborn requiring resuscitation was placed on the warmer for the duration of the resuscitation, and then returned to the mother.
The study nurse observed the preparation, use, and cleaning of the warmer with each encounter, and recorded instances in which these steps were not properly executed. If she observed deviation from the proper protocol, she was instructed to intervene and collect data regarding the potential misuse of the warmer.
Qualitative Study
A qualitative arm of the study was carried out in order to better understand the user experience with the infant warmer. A phenomenological approach was used in order to gain an understanding of caregivers’ and nurses’ experiences working with the warmer. We intended at each health center to interview 10 to 15 caregivers and 1 to 3 nurses until we reached saturation.
Semistructured in-depth qualitative interviews were conducted with caregivers and nurses. Participation in the interview was not required for the infant to be enrolled to use the infant warmer. All interviews were conducted in a private space at the local health center where the person worked. Interviews were carried out in the local language, Kinyarwanda, audio recorded, transcribed, and then translated into English by a professional Rwandan translator. An independent translator back-translated 10% of the interviews into Kinyarwanda, and compared them with the original transcripts for validation. Analysis began with completion of the first interview. Contents were assessed to assure sufficiency of questions used.
A caregiver met inclusion criteria if present during the use of the warmer. The only exclusion criterion was unwillingness to consent. Centers with the largest number of encounters with the warmer were given the largest number of interviews.
Protocol Changes
We intended to enroll patients during transport from health centers to district hospitals, but due to feasibility issues related to space for the study nurse during transportation and limited study staff, after the first transport case, this inclusion criterion was eliminated.
Ethical Approval and Informed Consent
The study was approved by the Boston Children’s Hospital Institutional Review Board (IRB-P00016205), the Rwanda National Ethics Committee (Reference # 0076/RNEC/2018), Rwanda National Health Research Committee (Reference # 514), and the Rwanda Ministry of Health. The study was also registered at ClinicalTrials.gov (Registration #: NCT03031431).
Outcomes
Quantitative outcomes included the following:
Safety. Incidence of hyperthermia (>37.5°C), skin rash, burn, or other adverse reactions
Effectiveness. For all hypothermic (<36°C) infants attained temperature ≥36.5°C attained a temperature ≥36.5°C in ≤2 hours rate of temperature rise ≥0.5°C/h
Feasibility.
Usability: observation of correct preparation, use, and cleaning of warmer Functionality: duration of warmer at goal temperature, external signs of wear and tear of warmer with repeated uses
Statistical Analysis
To assess the influence of continuous covariates on the outcomes, we performed logistic regression with adjustment for clustering of multiple encounters per participant. To assess the influence of binary covariates, we used Fisher’s exact test. Quantitative data were analyzed using Stata v.15.1 (Stata Corp, College Station, TX). Numbers and percentages were reported for categorical variables, and median, interquartile range, minimum, and maximum for continuous variables. The median body temperature achieved on the warmer, ambient air, and infant warmer temperature was calculated as a summary of the encounter medians. The time to euthermia is the time when the body temperature of a hypothermic infant was first reported to be ≥36.5°C.
De-identified interview results were coded using Dedoose software version 8.1.8 (Los Angeles, CA). Duplicate coding was used to assure objectivity. Semi-open coding and 3 levels of thematic analysis were utilized. Initial themes were identified and further explored in order to identify reoccurring themes and broad patterns of personal experience (Online Appendix 1). From this, we were able to reduce the textural and structural meanings of the described experiences to key descriptions. Selected direct quotes to illustrate summary findings can be found in Online Appendix 2.
Role of the Funding Source
The study was funded by the Arthur Rosenfeld fund at Harvard Medical School. This funding had no influence on data collection, analysis and interpretation, manuscript preparation, or decision to submit the article for publication.
Results
We enrolled 97 patients for a total of 102 encounters. Three patients used the warmer twice, and 1 used the warmer 3 times. Twenty-one encounters occurred at the colder sites, and 81 at the warmer sites. Eighty-one encounters were initiated for hypothermia, and 21 for resuscitation. Of the 81 initiated for hypothermia, almost half involved infants of term gestation (Table 2). A high proportion of infants had an unknown gestational age, reflecting low rates of fetal dating in rural Rwanda. The majority of encounters were on the day of birth; all were in the first week of life (Table 2).
Clinical and Demographic Characteristics of Infants Participating in the Infant Warmer Study Phase II (N = 97).

Warm sites.
Cold sites.
In 1 of the 81 encounters initiated for hypothermia, the infant was removed from the warmer after only 15 minutes by maternal request. In the other 80 encounters, the infant remained on the warmer until reaching 36.5°C or for 6 hours, whichever came first.
Because of the lack of electric warmers, only 6 of the 17 encounters in which infants had a starting temperature <35.0°C received electric heat according to the goal study design. KMC was combined with the warmer in 12 (15%) of the encounters at the start of warmer use, and this fell to zero by 3 hours as patients became euthermic. In all 80 encounters, infants used a blanket, 23 (29%) used a hat, 1 wore additional clothes for 2 hours in the middle of the study, and none used diapers.
Unlike our previous study in the district hospital setting when we also enrolled patients who were at risk for hypothermia on the basis of being LBW, due to the lower risk deliveries in the health center setting, no patients were enrolled on the basis of this “at-risk” inclusion criterion.
For the 21 neonatal resuscitation encounters, infants were removed from the warmer once the resuscitation was complete; only 4 remained on the warmer for >30 minutes and none were on for more than an hour. One resuscitation patient was also transported on the warmer; this infant was on the warmer for a total of 1 hour.
While all encounters (for hypothermia and resuscitation) were included in the safety and feasibility analyses, the effectiveness analysis excludes encounters in which the patient was on the warmer for ≤1 hour (all resuscitation encounters and 1 hypothermia encounter of only 15 minutes). Of note, the 4 resuscitation patients who were on the warmer for ≥30 minutes did achieve the goal rate of rise of ≥0.5°C/h.
A total of 39 caregivers (30 from warm and 9 from cold climates) and 12 nurses (10 from warm and 2 from cold climates) were interviewed. There were enough interviews to achieve saturation.
Safety
Of the 102 encounters, there were zero instances of hyperthermia (temperature >37.5°C), burns, rashes, or other adverse events. Overall, both caregivers and nurses found the infant warmer to be safe (Quotes [Q] Q1, Q2, and Q3 in Online Appendix 2). Neither group reported observing any adverse effects. Nurses specifically remarked that the warmer was a beneficial instrument in low-resource settings; they found it a strong alternative to competing warming methods, specifically electric warming tables (Q4), because it required less monitoring (Q1), allowed for easier regulation of temperature (Q1), thereby reducing the likelihood of causing hyperthermia.
Effectiveness
Of the 80 encounters in which infants were enrolled for hypothermia and were on the warmer for the study duration, the starting temperature of the infants ranged from 33.1°C to 35.9°C with a median of 35.5 (IQR = 35.0-35.7; Figure 2 and Table 3). Seventy-nine out of 80 (98.8%) achieved a temperature 36.5°C. The infant who remained hypothermic had a gestational age of 38 weeks, was born at a warm site, had a starting temperature of 35.5°C, and a maximum temperature of 36.3°C after being on the warmer for 2 hours. The temperature then fell to 36.1°C at 4 hours, at which time the mother elected to take the baby off of the warmer. During a second encounter with the warmer, this infant achieved euthermia. During 73/79 (92.4%) of the hypothermic encounters, patients who achieved a temperature ≥36.5°C achieved this temperature in ≤2 hours (Table 4). During 64/80 (80%) of hypothermic encounters, the rate of temperature rise was ≥0.5°C/h (Table 3).

Effectiveness of infant warmer. Infant temperature at study initiation compared to maximum infant temperature on warmer (n = 81).
Effectiveness of Infant Warmer.

Excludes 1 hypothermic patient only on warmer for 15 minutes.
Excludes 1 hypothermic patient who did not achieve a temperature of 36.5°C.
Percentage Distribution of Encounters by Time When Hypothermic Infants Achieved Euthermia.

The rates of success (Table 3) were not affected by regression adjustment for the infants’ gestational age or birth weight, owing in part to low statistical power in the face of the near-unanimous successful outcomes. Encounters at cold sites and warm sites differed minimally and nonsignificantly. Euthermia was reached in 60/61 encounters at warm sites (98%) and 19/19 encounters at cold sites (100%; P = 1 by Fisher’s exact test). Of successful encounters, 57/60 attained euthermia by 2 hours at warm sites (95%), compared with 16/19 at cold sites (84%; P = .15). The rate of rise was at least 0.5°C/h in 47/61 encounters at warm sites (77%), compared with 18/19 at cold sites (95%; P = .10).
Before use, some interviewees reported skepticism that the warmer would help the infants. After use, participants overwhelmingly found that the device successfully warmed infants (Q2). Additionally, they found it to be faster and more helpful in warming infants when compared with electric warming tables (Q1, Q4), KMC alone (Q2, Q5), or clothing. Many reflected that they would use the warmer again with another infant, or recommend it to a friend. There were no negative comments related to the effectiveness of the warmer.
Feasibility
Usability
In all 102 encounters, the warmer was prepared, used, and cleaned correctly. Caregivers and parents overwhelmingly liked the warmer design and reported that the warmer was comfortable for the infant and easy to use (Q6). Caregivers found the temperature indicator easy to understand. Nurses described the simplicity and electricity-free functionality of the warmer to be key assets, explaining that many hospitals in the area are vulnerable to power outages and lack consistent electricity. A recurring theme found among a minority of nurses was that preparation took too long and the warmer was not readily available for urgent cases (Q7).
Functionality
Five out of 12 warmers (42%) showed signs of wear and tear. One warmer developed an internal leak after 23 uses allowing water to move between the inside (not outside) plastic layers. One warmer’s temperature indicator fell into the cold zone too early after 32 uses, 3 warmers’ low-literacy instruction ink started fading, and one of the insulating sleeves was described as peeling during a single encounter. The infant warmer temperature remained in goal temperature range (35°C and 38°C) for the duration of the study for 90 out of 102 (88.2%) encounters (Figure 3). The median temperature was 37°C for the 6-hour study period (Figure 3). All out-of-range temperatures were due to the warmer measuring above the maximum temperature of 38°C.
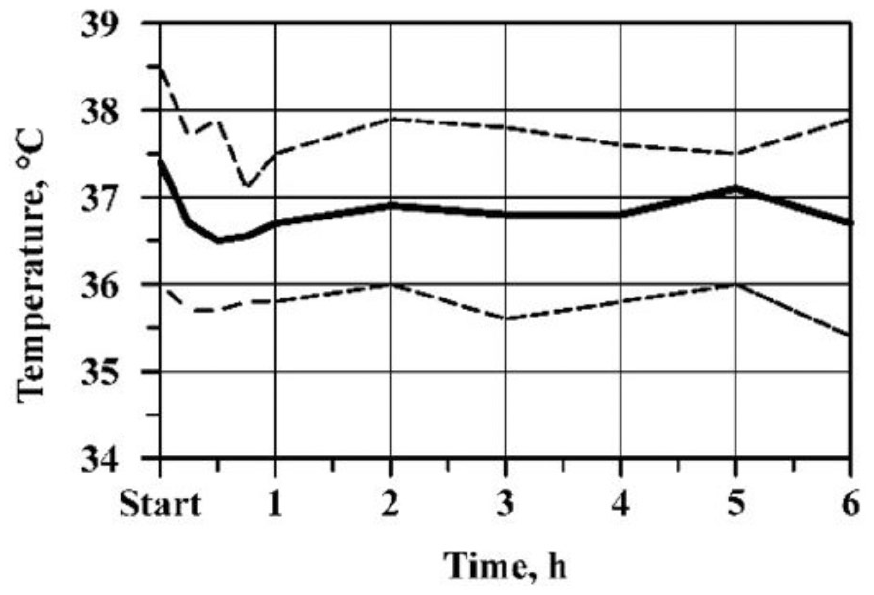
Warmer temperature over time (median, minimum, and maximum).
Caregivers overwhelmingly found the warmers to be well made. Several participants suggested that it be longer to accommodate the feet of long babies (Q8), and that the low literacy instructions could be easier to understand.
Participants found that the warmer allowed for the use of complementary care. They described that it worked well with breastfeeding (Q9), during medical interventions and resuscitation. They appreciated that the warmer avoided separation of the mother and newborn (Q4). Caregivers specifically preferred this method to the use of an electric warming table, as they were still able to lie with, breastfeed, and provide KMC while their newborns were using the warmer.
Nurses reported that the warmer was particularly beneficial for resuscitation, as some had a perception that putting an infant who had experienced fetal distress on an electric warming table may cause an increase in distress of the infant. Again, caregivers enjoyed being able to remain in close contact with their newborns during resuscitation, and both caregivers and nurses valued the ability to treat the infant as necessary, while allowing the caregiver to maintain a connection with the baby.
Finally, nurses found that the warmer allowed for easy medical access to the baby, for vaccinations, oxygen, or intravenous medication. Users were quick to recommend the infant warmer, and many suggested that it be used broadly in health clinics to save more lives. Caregivers and nurses overwhelmingly appreciated its ease of use, electricity-free operation, allowance of medical interventions, and maternal care (Q2, Q3, Q5, Q6, and Q9).
Discussion
The World Health Organization reports that over 20 million infants weighing <2500 g are born each year, more than 96% in developing countries. 29 They acknowledge that while KMC is the preferred method of preventing and treating hypothermia for these LBW newborns, it is not always possible; therefore, technologies aimed at complementing KMC are an important means for improving health outcomes of preterm and sick neonates. 29 While incubators are the most advanced technology for thermoregulation, they can be prohibitively expensive, deny easy access to the infant, and introduce infectious risks.29,30 Warming beds provide a potential alternative to the incubator that avoid these problems. 29
In response to the widely recognized need for improved technological options, the Program for Appropriate Technology in Health convened a panel of neonatal experts who generated the following list of important characteristics of an ideal warming devices for use in the low-resource settings: generates and maintains heat, real-time temperature indicator for infant, limited temperature control by user, minimal maintenance/consumables, ease of use by trained health workers in urgent care settings, easy access to baby, baby visible for monitoring, low-literate and written instructions imprinted on device, compatible with alternate power source, durable for routine daily use, able to be reused, easy to clean, appearance of high-tech design to appeal to health professionals, able to hold infant securely with no risk of dropping/falling, manufactured of nontoxic materials, no chance of suffocation or strangulation, able to transport infant in case of surgery, or when infant needs to be moved to another location or within the facility. 31
They then reviewed available devices against their metrics, in the categories of radiant warmer beds, TransWarmer mattresses, and occlusive wraps. 23 All of the devices they reviewed lacked many of these characteristics. In the category of mattresses, they fell short in being single use, not allowing visibility and accessibility to the infant, and not including low literacy instructions. Our infant warmer measures highly favorably against these characteristics, with the possible exception of a falling risk similar to any infant laid on a bed.
In a more recent review of exothermic mattresses designed for the resource-limited setting, options are considerably more expensive than our infant warmer, do not allow access for medical interventions and assessments, and have an attached fabric design that is not amenable to multiple users in an environment in which diapers and clothes washers are in scarce supply.24,31-34
In this context, we report a mixed-methods study of a nonelectric infant warmer used in rural health centers in Rwanda. This builds on our previous study in Rwandan district hospitals by assessing its performance in a population with more term newborns in a setting with less consistent electricity, fewer nurses, who have a lower level of education and experience. The warmer’s performance confirmed and exceeded our results from the hospital setting.
It was consistently safe, highly effective, and appropriately used. Participants offered predominantly positive feedback regarding the safety, effectiveness, and feasibility. The biggest concern was raised by nurses, some of whom found the preparation time challenging. We will incorporate this finding in future educational materials for the infant warmer, stressing the value of preparing the warmer in anticipationg of neeed, letting it sit in the thermos in anticipation of need. The warmer exhibited unacceptably high rates of wear and tear in these handmade prototypes. As we prepare for automated factory manufacturing of the warmer, we are improving robustness of the plastics and sealing process, temperature indicator, and ink.
We combined the results of our current and prior study, 27 in which we employed identical methods and analysis, to provide overarching indicators of the warmers cumulative record. With a total of 204 encounters, 3.4% resulted in hyperthermia with no instances of burns, rashes, or other adverse events, 97.6% of hypothermic encounters warmed to ≥36.5°C, 90.8% within 2 hours, and 77.2% warmed at a goal rate of ≥0.5°C/h. Hypothermia was prevented in 100% of encounters when patients were put on the warmer because they were at risk for hypothermia due to LBW when KMC was not available. In all instances, the preparation, use, and cleaning of the warmer was correct. A total of 7/12 (58%) warmers demonstrated wear and tear. Thus, the infant warmer has an accumulating record of safety, effectiveness, and feasibility, but requires more a robust plastic and manufacturing process.
Our study had several limitations. This was not a randomized controlled trial comparing the infant warmer to current standard of care; rather, it was a pilot study in a purposeful sample. We had intended to study the warmer on transport but were unable due to logistical issues. Its use in resuscitation was difficult to interpret due to the short duration that infants were exposed to the warmer. It did demonstrate the safety and feasibility of this indication, with no instances of hyperthermia, adverse events, or improper preparation, use, or cleaning. The resuscitation population was useful in demonstrating that the warmer could be prepared in advance and be ready for use if resuscitation were needed.
Given our promising results, our next step is to conduct a stepped wedge randomized controlled trial in 10 district hospitals in rural Rwanda over a 6-month period, motivated by the sentiments expressed by this caregiver in our qualitative interview, “For me, I found that the warmer doesn’t cause any problem, it is a very good thing. Maybe you should see how you can supply the warmers to all health facilities and health posts, just everywhere so that new babies can be warmed up”.
Supplemental Material
Appendix_1,2 – Supplemental material for Performance of a Nonelectric Infant Warmer in Rwandan Health Centers
Supplemental material, Appendix_1,2 for Performance of a Nonelectric Infant Warmer in Rwandan Health Centers by Leana May, Alphonse Nshimyiryo, Marthe Kubwimana, Evrard Nahimana, Natalie Schoen, Ashok Gadgil, Fredrick Kateera, Henry A. Feldman, Merab Nyishime and Anne Hansen in Global Pediatric Health
Footnotes
Acknowledgements
We acknowledge critical support from the Rwanda Ministry of Health, Partners In Health/Inshuti Mu Buzima, and the neonatology teams from Rwinkwavu, Kirehe, and Butaro District Hospitals for facilitating the study. We thank David N. Williams, MA, PhD, and Annie Michaelis, PhD, for their assistance with the qualitative research analysis, and Hema Magge, MD, for her assistance with the study design. We thank the Lawrence Berkeley National Laboratory for the technical design of the Infant Warmer. Our special thanks goes to the patients and families who are the true inspiration for this innovation.
Author Contributions
Drs Hansen and May conceptualized and designed study, drafted the manuscript, performed data analysis, reviewed and revised the manuscript, and approved the final manuscript as submitted.
Ashok Gadgil, the lead engineer, designed and tested the Infant Warmer.
Alphonse Nshimyiryo performed data analysis, reviewed and revised the manuscript, and approved the final manuscript as written.
Marthe Kubwimana collected data, reviewed and revised the manuscript, and approved the final manuscript as submitted.
Dr Nahimana conceived and designed the study and reviewed and approved the final manuscript as written.
Natalie Schoen analyzed the qualitative data and approved the final version of the manuscript as submitted.
Dr Kateera reviewed the study design and approved the final manuscript as submitted.
Dr Feldman performed data analysis, reviewed and revised the manuscript, and approved the final manuscript as submitted.
Merab Nyishime assisted with data collection and study support, and reviewed and revised the manuscript and approved the final manuscript as written.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Hansen reports other support from the Arthur Rosenfeld Fund at Harvard Medical School. Nonfinancial support was provided by Global Newborn Solutions. The Regents of University of California hold patent US D773681 for the Infant Warming Pad.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Arthur Rosenfeld fund at Harvard Medical School.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.