
Abstract
Objective. The aim was to determine the association between access to dental services and toothbrushing in Peruvian children under 12 years old. Methods. This was a cross-sectional study with a population of 2021 database of the Demographic and Family Health Survey. Records of children under 12 years old who provided answers about their toothbrushing were included. Variables were evaluated descriptively and followed by a bivariate analysis; multivariate tests were performed using Poisson regression with a multilevel regression analysis. Results. General toothbrushing was 96.32% (n = 34 198), and daily toothbrushing was 88.05% (n = 28 444). Access to dental services was associated with general toothbrushing (aPR: 1.18; 95% CI: 1.14-1.22; P < .001), daily toothbrushing (aPR: 1.08; 95% CI: 1.04-1.12; P < .001) and minimum toothbrushing 2 times a day (aPR: 1.12; 95% CI: 1.07-1.17; P < .001). Conclusion. Access to dental services was associated with general toothbrushing, daily toothbrushing and toothbrushing at least twice a day.
Introduction
Access to health services refers to a process involving factors such as availability, efficacy, acceptability, and the presence of barriers and facilitators for its use, considering its main purpose to satisfy the population’s needs.1,2 From a dental perspective, access is limited and inequitable, resulting in a more significant disease burden, mainly affecting lower-income populations. 3 In Peru, it has been identified that extreme age groups such as children and older adults face limited access to dental services, with the area of residence, natural region, wealth quintiles, and sex being perceived as mediating factors.4 -6
On the other hand, the high prevalence of oral pathologies such as dental caries is a problem for global public health, particularly in developing countries, highlighting the necessity to reinforce effective preventive habits against this disease. 7 Evidence suggests that diet control, access to information, use of fluorides, and toothbrushing are the main preventive habits. 8 Thus, access to dental care is essential in ensuring the provision of preventive tools for this condition. 9 Regarding toothbrushing, it is urged that this habit should begin before the first year of life to ensure consistency in its practice over time; it is also recommended to practice it at least twice daily, given its preventive purposes against dental caries. It is essential to emphasize that toothbrushing is a beneficial, affordable, widespread, and culturally accepted act; hence, it is an effective measure for public health.10,11 At the national level, specific reports indicate a limited frequency of toothbrushing, mainly in younger individuals and members of families with limited economic resources.12,13
Promoting healthy practices, like toothbrushing, 14 within the context of the lowest dental care access is challenging, especially in vulnerable communities. Scientific evidence shows that the successful establishment of the toothbrushing habit is linked to receiving information on the prevention of oral cavity diseases, which in many countries is provided in the dental office.15,16 On the other hand, it was observed that the poorest adults have the same or greater predisposition to follow preventive practices than others with a higher socioeconomic level; contradictorily, their use of dental services was the lowest. 17 In this regard, the Peruvian Dental Caries Clinical Practice Guideline suggests that before the first year of life, children should receive a dental evaluation, an opportunity to make parents aware of the initiation and frequency of brushing. 18 In this sense, evidence has yet to be identified on the association between these 2 factors, and it is necessary to consider that Peruvian children have an inadequate frequency of this good oral health practice. Therefore, the aim is to generate studies that address this problem, starting with this one that seeks to determine the association between access to dental services and toothbrushing in Peruvian children under 12 years old.
Methodology
A cross-sectional study was performed, where the population comprised the 2021 Demographic and Family Health Survey (ENDES) database, carried out by the National Institute of Statistics and Informatics of Peru (INEI). It is worth noting that a trained team executes the ENDES survey every year. This team conducts in-home interviews and administers questionnaires to the designated population.
It had a 2-stage, stratified, probabilistic, balanced, and independent sampling at the departmental level, both by urban and rural area. The sample size for the year 2021 amounted to 36760 dwellings, which meant 168145 children under 12 years old; only the data provided by survey respondents regarding their toothbrushing habits will be used for analysis, leading to a final sample size of 32023. As a criterion for managing the records, incomplete ones were eliminated (Figure 1). The ENDES survey comprises 3 questionnaires: health, household, and individual; it should be clarified that the person providing the information is the individual (over 15 years old) responsible for the children’s health care. 19

Flow chart of sample screening inclusion and exclusion.
Regarding the variables established, general toothbrushing (Does [NAME] brush his/her teeth with a toothbrush?), daily toothbrushing (Does [NAME] brush his/her teeth every day?) and toothbrushing at least twice a day (How many times a day does [NAME] brush his/her teeth?) were considered dependent. In contrast, access to dental services, time since last dental care (measured in years) and place of dental care were determined as independent. According to the information given, the healthcare provider that carried out the service was classified as either the Ministry of Health of Peru (MINSA), Social Health Insurance of Peru (ESSALUD), Armed Forces (FF.AA) and Police (PNP), or the private sector. In addition, covariates were defined as the natural region, categorized into Metropolitan Lima, the rest of the coast, the highlands and the jungle. The area of residence was also evaluated, organized into urban and rural; place of residence divided into capital, city, town, and countryside; altitude measured at less than 2500 meters above mean sea level (MAMSL) or from 2500 MAMSL and more. Wealth index is a measure of a household’s ability to access and enjoy goods and services; subsequently, a score was assigned to each household and its residents using a formula utilized by the United States Demographic and Health Surveys Program. It made it possible to classify each dwelling according to quintiles from the poorest to the richest.20,21 It also included health insurance coverage, whether public or private; sex of the individual and age, divided into 2 groups: 0 to 5 and 6 to 11 years old.
Data Collection Procedures
The 2021 database was downloaded from the INEI’s official web page (http://iinei.inei.gob.pe/microdatos/), obtaining the survey’s modules and technical datasheet, and finally exported to STATA SE 17.0.
Statistical Analysis
For the statistical analysis, absolute and relative frequencies of the variables were obtained through a descriptive analysis, followed by a bivariate analysis using the Chi-square test to find associations between the variables under study. It is essential to clarify the use of the svy command, which allowed representative estimates to be established following the survey design, where the sampling patterns were distinguished according to stratum, primary sampling unit, and weights. Furthermore, Poisson logistic regression was utilized to conduct multivariate tests to determine the crude prevalence ratios (PR) and adjusted prevalence ratios (aPR) based on the previously demonstrated significance variables. The variables’ association with toothbrushing was analyzed using multilevel regression; it should be noted that the 24 regions of Peru were established as the level of analysis. With this information, a variance component model was built (null model) using general toothbrushing, daily toothbrushing and toothbrushing at least twice a day as dependent variables, but without inserting explanatory variables; the null models estimated the general variability of the dependent variables and attributed it to the regions justifying proceeding with the analysis (P < .001). Subsequently, a series of explanatory variables were included to analyze the association with each independent variable and covariates. Four models were created: unadjusted model 1 of access to dental services, unadjusted model 2 of geographical characteristics, unadjusted model 3 of sociodemographic characteristics and adjusted model 4 of access to dental services by covariates. This research used a confidence level of 95%, and as an indicator of statistical significance, a value of P < .05 was defined in all tests.
Ethical Approval and Informed Consent
The study was approved by the Institutional Ethics Committee of Universidad Peruana Cayetano Heredia (CIE-UPCH), with a SIDISI code of N° 206253. It should be noted that these databases are publicly accessible, and the records are coded to maintain the anonymity of the respondents. For this research, CIE-UPCH waived the requirement for informed consent due to the survey characteristics.
Results
General toothbrushing was 92.76% (n = 32 023), daily toothbrushing was 84.28% (n = 25 511), while minimum toothbrushing 2 times daily was 79.95% (n = 19 871). Access to dental care was 52.96% (n = 17 519), 12.72% (n = 2071) reported that their care was less than 2 years ago, and the main place of dental care was the Peruvian Ministry of Health with 46.37% (n = 10 306) (Table 1). In a bivariate manner, access to dental care, time since last dental care, and place of dental care presented an association with general toothbrushing (P < .05); concerning daily toothbrushing, it was associated with access and place of dental care (P < .05). While toothbrushing at least twice a day was associated with access to dental care and place of that care (P < .05). Similarly, the 3 variables of interest were associated with the natural region, area of residence, place of residence, altitude, wealth index, and age. On the other hand, sex was associated with general toothbrushing (P < .05) (Table 2).
Toothbrushing, Access to Dental Services and Characteristics of Children Under de 12 Years Old in Peru, 2021.

n: Absolute frequency; %: Relative frequency.
Toothbrushing According to Access to Dental Services and Characteristics of Children Under 12 Years Old in Peru, 2021.
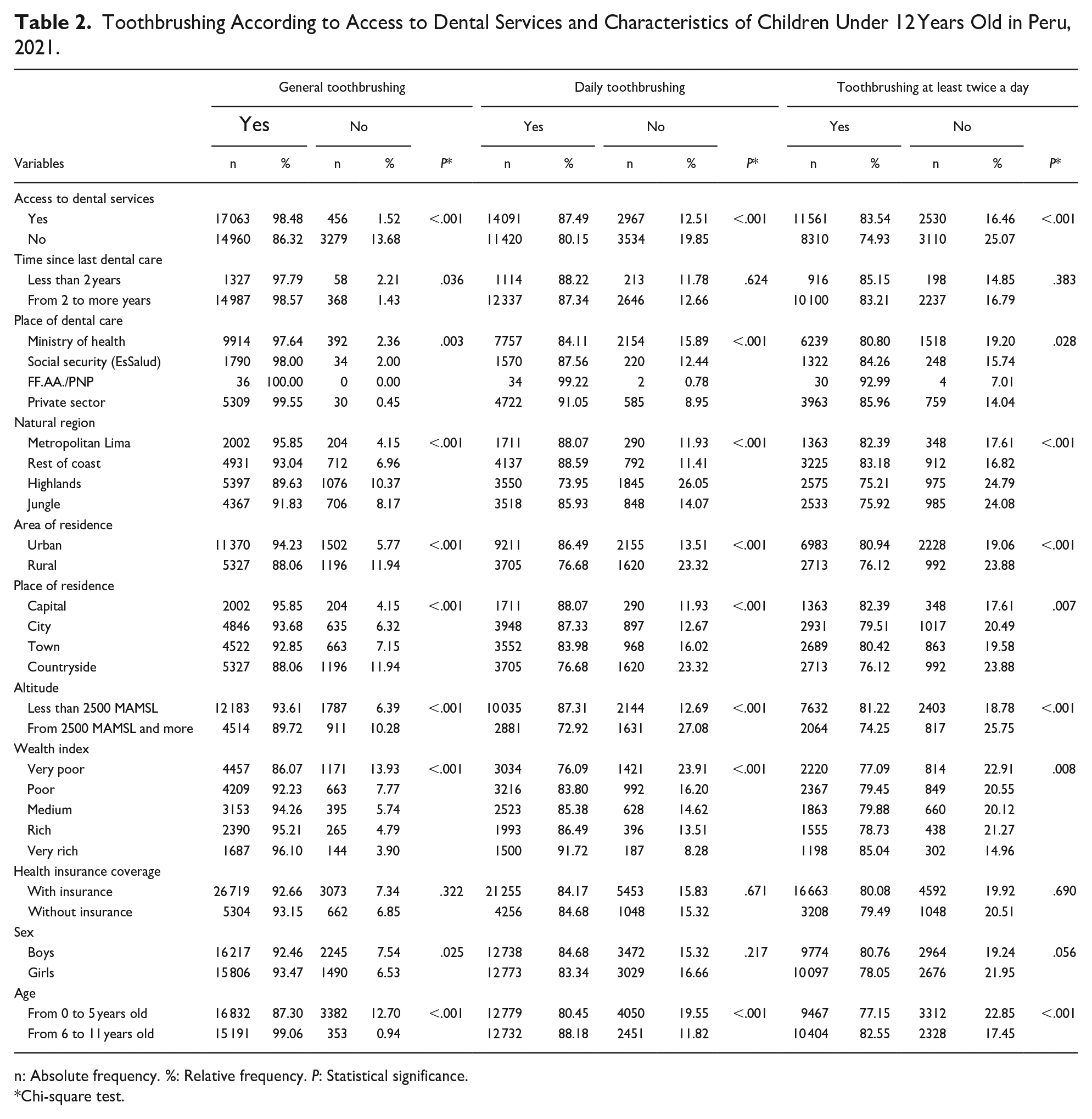
n: Absolute frequency. %: Relative frequency. P: Statistical significance.
Chi-square test.
In the multilevel regression analysis, access to dental care was associated with general toothbrushing (aPR: 1.18; 95% CI: 1.14-1.22; P < .001), daily toothbrushing (aPR: 1.08; 95% CI: 1.04-1.12; P < .001), toothbrushing at least twice a day (aPR: 1.12; 95% CI: 1.07-1.17; P < .001), adjusted for the variables in which an association was previously identified. However, this analysis was also developed for the time since last dental care, showing the absence of statistical significance in the results for general toothbrushing (aPR: 0.98; 95% CI: 0.92-1.05; P = .598), daily toothbrushing (aPR: 1.05; 95% CI: 0.98-1.13; P = .171), toothbrushing at least twice a day (aPR: 1.03; 95% CI: 0.95-1.11; P = .501). At the same time, none of the providers of the place of dental care, according to general toothbrushing, did present statistical significance: Social security (EsSalud) (aPR: 1.01; 95% CI: 0.93-1.10; P = .797), Armed Forces/PNP (aPR: 1.03; 95% CI: 0.63-1.68; P = .904) and the private sector (aPR: 1.03; 95% CI: 0.97-1.10; P = .285); for daily toothbrushing, Social security (EsSalud) (aPR: 1.04; 95% CI: 0.95-1.14; P = .347), Armed Forces/PNP (aPR: 1.04; 95% CI: 0.63-1.171; P = .890) and private sector (aPR: 1.07; 95% CI: 1.00-1.14; P = .051) were not statistically significant. Finally, toothbrushing at least twice a day indicated that Social Security (EsSalud) (aPR: 1.03; 95% CI: 0.94-1.14; P = .525) and the Armed Forces/PNP (aPR: 1.14; 95% CI: 0.68-1.92; P = .614) and private sector (aPR: 1.06; 95% CI: 0.99-1.14; P = .110) were not statistically significant (Table 3).
Association Between Toothbrushing and Access to Dental Services in Children Under 12 Years Old in Peru, 2021.
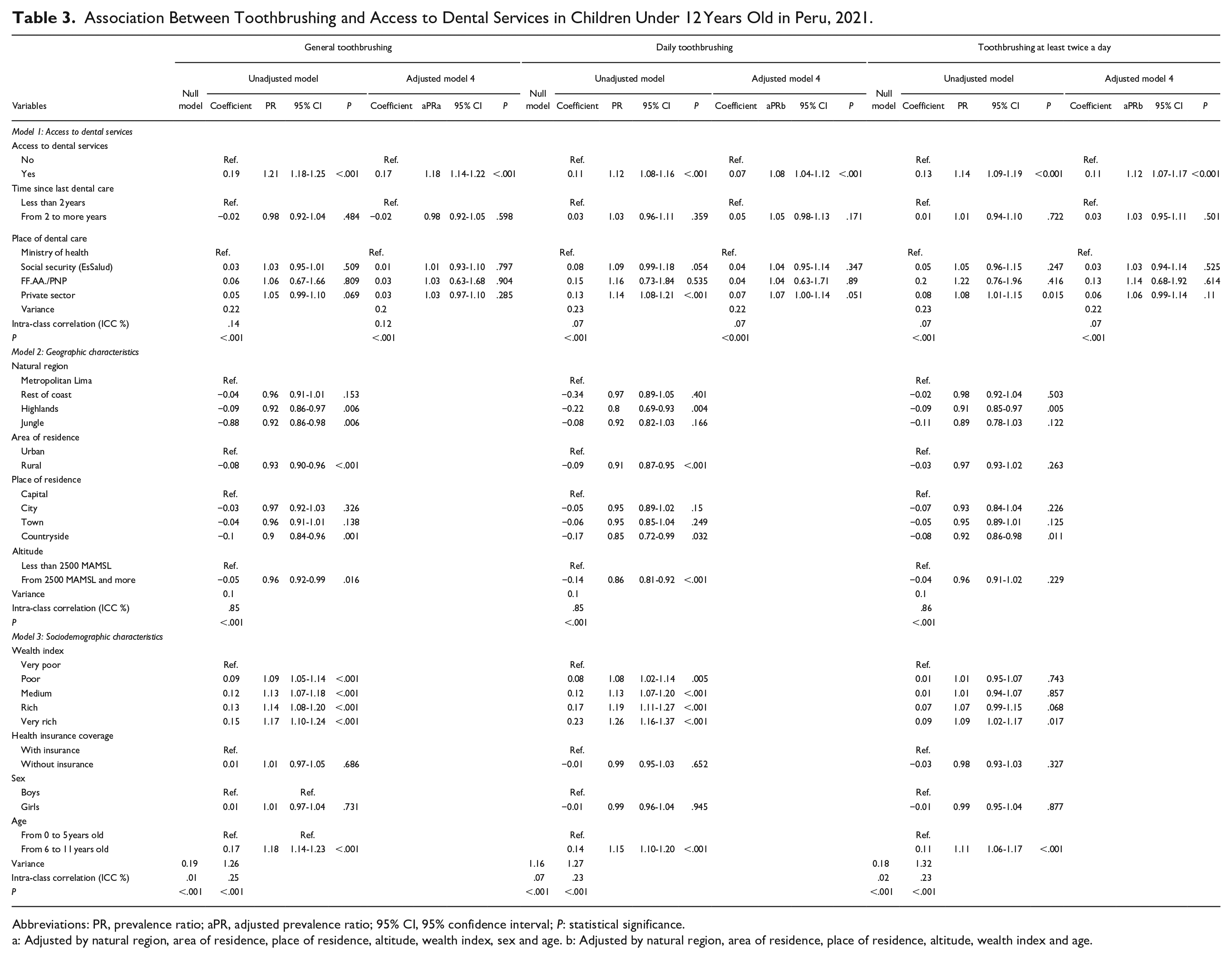
Abbreviations: PR, prevalence ratio; aPR, adjusted prevalence ratio; 95% CI, 95% confidence interval; P: statistical significance.
a: Adjusted by natural region, area of residence, place of residence, altitude, wealth index, sex and age. b: Adjusted by natural region, area of residence, place of residence, altitude, wealth index and age.
Discussion
From the dental perspective, low access to dental care is one of the leading public health problems. This situation prevents the optimal extension of hygienic habits to the population, such as toothbrushing, 14 and there are limitations to its application in vulnerable communities, especially in those individuals in the extreme stages of life. Among the findings of this research, there is evidence of the association between access to dental care and general toothbrushing, daily and at least twice daily, as well as the place of dental care with general toothbrushing, daily and at least twice daily. Research conducted by Hernández-Vásquez and Azañedo suggests that children who have not had a dental visit in the last 6 months may tend to lower levels of brushing compared to those who have had a recent dental visit. Likewise, the study in Mexican children by Vallejos-Sánchez et al mentions that those who had dental care 1 year before the study had a higher probability of frequent brushing.12,22 These suggest that regular contact with the oral health professional reinforces healthy preventive practices such as tooth brushing.
Regarding toothbrushing, this study found that approximately 90% of the sample reported that they typically brushed their teeth; in addition, comparable results were achieved with daily practice, but the effectiveness decreased when it was considered that the activity should be performed at least twice daily. On this matter, the Peruvian Ministry of Health, through its Clinical Practice Guideline for preventing, diagnosing, and treating dental caries in children, recommends that this preventive habit be performed at least twice daily, starting from the first tooth’s eruption, approximately after 6 months of age. 18 On the other hand, a national database study carried out in Iran states that the frequency of children who brush their teeth twice daily is 4 times less than those who do it once; it has also been suggested that this occurrence may be related to socioeconomic and demographic factors, as well as the healthcare system that the child and their family are associated affiliated. 23 Studies conducted on the Peruvian population confirm that the frequency of toothbrushing increases with age, and this practice is widely adopted and established,12,13 aligning with the findings of this study.
It is essential to consider that the information produced by this research covered only the year 2021, within a national context perceived as a “new social coexistence” due to the COVID-19 pandemic. 24 However, the situation experienced in the country in 2020 would have impacted different sectors of Peruvian society, including oral health. The scientific evidence developed from health emergency reports that the time since the last dental care in Peruvian children would have increased by 1.39 years, indicating that this dilation in the search for timely care would be associated with the year of the pandemic, noting that in previous years, variables such as place of dental care, natural region of residence and age already showed significant differences, but the year itself denotes greater relevance. 25 Regarding toothbrushing, it was observed that the pandemic harmed its daily practice at least twice daily, which could be explained by the complex context faced by the country due to multiple measures to contain contagions that impacted the economy and social habits of Peruvian households, so that more pressing aspects may have been prioritized, rather than a preventive habit; similarly, it was found that factors such as geographic region, area and place of residence, altitude, health insurance coverage, economic level, age, and sex were associated with brushing. 26
Among the limitations of this research is the use of secondary information sources such as the ENDES survey, where the information collected could present inaccuracies due to self-reporting. Regarding the study design, the cross-sectional type cannot infer causality from the associations or results found. Additionally, given the nature of the survey, it is not feasible to classify individuals by months of age, only by years completed. Therefore, it was decided to include those from 0 years of age, even though they did not yet have teeth. The Peruvian Clinical Practice Guidelines on dental caries recommends starting toothbrushing at 6 months of age, 18 so it can be expected that minors do not brush their teeth. Finally, it was observed that the survey lacks sufficient variables to assess the need for access to dental care, which would allow suggesting future modifications for future versions.
Despite the abovementioned limitations, the present study provides a first understanding of the link between access to dental health services and establishing preventive habits in Peruvian children, such as tooth brushing. It is essential to recognize that access to dental care in territories with emerging economies is still fragile and scarce, even though the country has been developing strategies such as Universal Health Insurance, intending to narrow the gap between people who do not have insurance and those who for financial reasons have not been able to obtain the necessary care. The multilevel regression analysis allowed us to understand the relevance of geographical characteristics variables; although these influence toothbrushing, access to dental services is still associated. Finally, policymakers at the national level should evaluate the importance and success of the application of these hygiene habits in oral health, not limiting it to coverage indicators, which, according to the study, access to a dental health service does not provide a guarantee that individuals in vulnerable situations, such as children under 12 years old, can enjoy optimal oral health and quality care.
Conclusion
Access to dental services was positive associated with general toothbrushing, daily toothbrushing, and toothbrushing at least twice a day. Likewise, specific covariates such as natural region, place of residence, wealth index, and age showed association with the three variables of interest; additionally, area of residence and altitude were.
Footnotes
Acknowledgements
We would like to thank to Facultad de Estomatología of Universidad Peruana Cayetano Heredia for covering publication charges.
Author Contributions
All the authors were involved in study conception, data collection, data acquisition and analysis, data interpretation, manuscript writing, review and editing. All the authors read and approved the final version of the manuscript for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Policy and Institutional Review Board Statement
The study received approval of the Institutional Ethics Committee of Universidad Peruana Cayetano Heredia (CIE- UPCH) SIDISI code N° 206253.
Patient Declaration of Consent
Not applicable.