
Abstract
Objective. This study aims to highlight the low birth weight (LBW) in Taiz City (Yemen), as LBW is one of the public health challenges experiencing a profound effect on newborns. Methods. This was a cross-sectional study since the interview and medical records were the sources of data to be analyzed by SPSS. Results. The findings of this study include; a high prevalence of LBW (39.11%), the maternal age was not associated with LBW (P = .68), and education level, economic status, residence place, and health status were not associated with LBW (P < .05). Although the pre-pregnancy BMI, during-pregnancy BMI, MUAC, and gestational age were significantly associated with LBW (P < .05), the only risk factor was gestational age (OR = 9.606, CI = 3.988-23.135, P = .00). Conclusion. LBW is highly prevalent in Taiz (Yemen), so providing good healthcare services is essential to manage LBW incidence.
Introduction
Low birth weight (LBW) is considered one of the significant public health challenges as it is a risk factor for early neonatal mortality and morbidity, particularly in developing countries.1,2 According to the World Health Organization (WHO), birth weight is defined as the first weight of the fetus or neonate measured after birth; and an infant with a weight of less than 2500 g is considered LBW regardless of gestational age. Infants with less than 1500 g and less than 1000 g are classified as very low birth weight (VLBW) and extremely low birth weight (ELBW), respectively.3 -7
Globally, it is estimated that 15.5% of infants are LBW, and most of these (96.5%) are in developing countries. The LBW incidence rate varies considerably across countries, ranging between 6.4% in Europe as the lowest incidence and 27.1% as the highest in South-Central Asia.4,5 According to the joint WHO and United Nations International Children’s Emergency Fund (UNICEF) study, the incidence of LBW in Yemen was 32% in 1997. 8 Another more recent 12-year retrospective survey conducted in Yemen reported that the pre-term LBW was 35.6% of hospital-admitted neonates, and 71.2% died. 9 Of concern is the increasing rate of LBW in low and middle-income countries.
The obstetrics, medical, nutritional, and lifestyle factors are crucial in determining the infant’s birth weight, which is considered an essential determinant of an infant’s survival and development.10 -13 LBW is a heterogeneous outcome of pre-term birth (born early, before 37 weeks of gestational age) or small size for gestational age (birth weight below the tenth percentile), or both. 5
LBW is at higher risk for growth and development retardation, chronic diseases, neurologic disability, impaired language development, impaired learning achievement, and early death.14 -16 In addition, its potential cost burden on the health system and households in the developed and developing countries.17 -21
LBW-associated factors, including nutritional status, have been investigated worldwide.16,22 -29 To the best of the researcher’s knowledge, this is the first study to report on LBW and its potential associated factors in Taiz, Yemen. However, the LBW had been reported last decade as a public health issue in other Yemeni cities.
Therefore, this study aims to highlight low birth weight as a complicated health problem, address the sociodemographic and nutritional status of mothers giving birth with low weight, and investigate the factors contributing to LBW among pregnant mothers attending certain hospitals and clinic centers in Taiz (Yemen).
Methods
Study Setting and Design
A cross-sectional study was conducted from April to September 2021 among pregnant mothers attending birth room centers and hospitals in Taiz City, which is located in southwestern Yemen (44.01°E, 13.34°N; about 1311 m above sea level), 280 km from the capital Sana’a. 30
Inclusion and Exclusion Criteria
All mothers, who were in the first hours of birth, and those who agreed to participate were eligible for inclusion in this study. Mothers who did not meet these criteria or had many missing data in the medical records were excluded.
Data Collection
A well-structured questionnaire was developed based on the related literature and then used to collect the data of the study participants by the pre-trained students from the therapeutic nutrition department under the supervision of a lead researcher. The questionnaire includes 5 parts; the first part is about the sociodemographic data, which includes age, educational level, residence place, and economic status (money income vs expenses; “not satisfied” means expenses are more than income, “good” means income is equal or less high than expenses and “perfect” means income is higher than expenses), the second part is about nutritional data, the third part is about mother’s anthropometric measurements, the fourth part is about medical test results (to be extracted from the medical record), and the fifth part is the information about the newborn. This questionnaire was pilot-tested in 25 mothers, and the internal consistency was evaluated by calculating Cronbach’s alpha. This study considered a Cronbach’s alpha of .7 or greater acceptable.
Data Analysis
The data were extracted from the corresponding questionnaires and entered into the SPSS (version 21). The variables’ adjustment, encoding, and correction checks were successfully performed before the analysis. The normality test for the variables was checked. The Mann-Whitney Test compared the 2 groups (LBW v NBW) regarding non-normally distributed variables. The Wilcoxon test was run to explore the effect of BMI before and after gestation on birth weight. The Odds Ratio (OR) of the risk factors was calculated. Univariate and multivariate regression analysis was performed to investigate these risk factors further.
Ethical Approval and Informed Consent
Ethical approval (JustMed/ 04/2021) was obtained from the Institutional Review Board (IRB), Faculty of Medical Sciences, Al Janad University of Science and Technology, Taiz, Yemen. The mothers, who agreed to participate in the study, provided verbal or written consent after sufficient explanation and promised to keep their information and answers confidential.
Results
Sociodemographic Characteristics of Study Participants (n = 225)
The sociodemographic characteristics of mothers who voluntarily participated in this study were presented in Table 1, where the birth weight was considered. The prevalence of low birth weight was 39.11%. The results showed that half of the mothers with LBW newborns (50%) were aged 26 to 35. In contrast, the percentage of mothers with NBW newborns was equally distributed regarding their ages. Regarding education level, the secondary holders were more than other certificate holders in both groups; 39.8% of mothers had LBW newborns, and 35% had NBW newborns. Most of the study subjects had good economic status in both groups; 69.3% of mothers had LBW newborns, and 76.6% had NBW newborns. Most of the study subjects were urban residents, and in both groups, 72.7% of mothers had LBW, and 63.5% had NBW. Similarly, most study subjects were healthy; 85.2% of mothers had LBW newborns, and 81.8% had NBW newborns.
Sociodemographic Characteristics of Mothers (n = 225) Attending Birth Rooms of Centers and Hospitals According to the Birth Weight, Taiz, Yemen, 2021.

Mann-Whitney test.
The results revealed that the maternal characteristics; age, education level, economic status, residence place, and health status exerted no effect on the birth weight since there were no significant differences between mothers who delivered low birth weight newborns and mothers who delivered normal birth weight newborns (P > .05).
Maternal Nutrition Status and Birth Weight
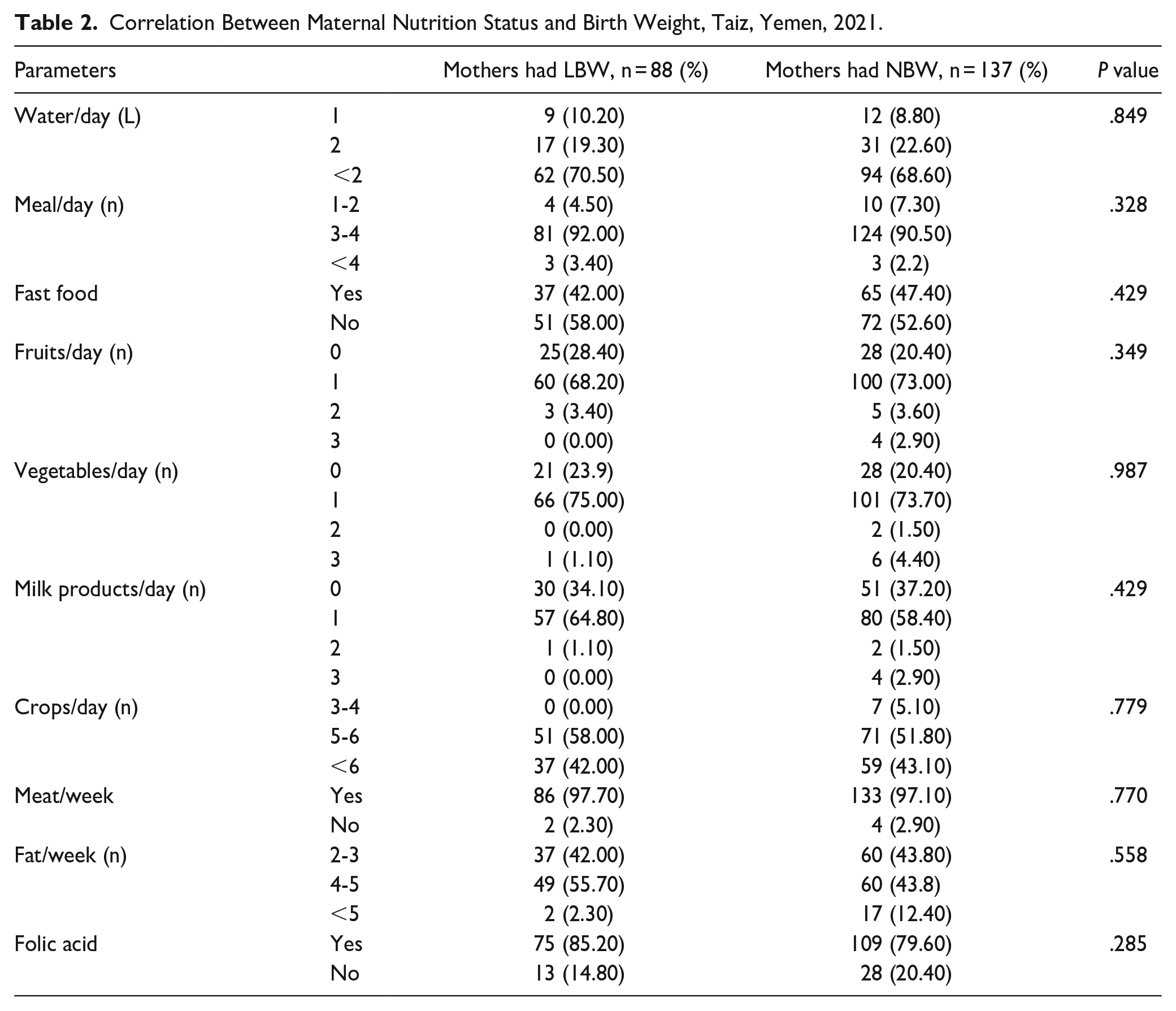
Most study subjects in both groups took more than 2 L/day; 70.5% of mothers had LBW, and 68.6% had NBW. Most of the study subjects in both groups had 3 to 4 meals daily; 92% of mothers had LBW, and 90.5% had NBW. Slightly more than half of the study subjects did not eat fast food. On the other hand, about two-thirds or more of the study subjects had fruits, vegetables, and milk products at least once per day. Most of the study subjects in both groups took meat and folic acid as a supplement.
The results of the correlation investigation between maternal nutrition status and birth weight are presented in Table 2. The results revealed that the numbers of meals, fruits, vegetables, and milk products taken per day were not significantly correlated with birth weight, and the numbers of meat and fat taken per week were not significantly correlated with birth weight. Similarly, folic acid as a supplement was not significantly correlated with birth weight (P > .05).
Correlation Between Maternal Nutrition Status and Birth Weight, Taiz, Yemen, 2021.
Maternal Anthropometric and Biochemical Parameters
The anthropometric and biochemical parameters of the study subjects are presented in Table 3. The pre-pregnancy weight, during-pregnancy weight, and mid-upper arm circumference (MUAC) of mothers who delivered normal birth weight newborns were significantly higher than those of mothers who delivered low birth weight newborns (P = .002, .026, and .004, respectively). The body mass index (BMI) of mothers with NBW newborns was significantly higher than that of mothers with LBW newborns. In general, the BMI of the mothers after gestation was significantly higher than their BMI before gestation, as deduced from the Wilcoxon test (P = .000). The results showed that the concentrations of hemoglobin and calcium did not differ between both groups (P = .534 and .694, respectively).
Anthropometric and Biochemical Parameters of Mothers Attending Birth Rooms of Centers and Hospitals, Taiz, Yemen, 2021.

Mann-Whitney test.
Anthropometric Parameters of Newborns
The anthropometric parameters measurements of the newborns were considered according to the birth weight and presented in Table 4. The results revealed that the gender and birth order exhibited no significant differences between newborns who have NBW and those who have LBW, and thus the gender and birth order exerted no effect on the birth weight (OR = 1.031 and 1.017; P = .509 and .536, respectively). Notably, 34% of the LBW newborns are pre-term (gestational age <37 weeks), while only 5% of the NBW newborns are pre-term. The gestational age was significantly correlated with the birth weight (OR = 9.606, P = .00). Consequently, newborns born before 37 weeks of gestational age were more likely to be LBW by 9 times than newborns born after 37 weeks. The height and head circumference of newborns with NBW were significantly higher than those with LBW (P = .00 for each Mann-Whitney test).
Anthropometric Parameters of Newborns, Taiz, Yemen, 2021.

Pearson Chi-square.
Mann-Whitney test.
Risk Factors of LBW, Univariate and Multivariate Logistic Regression
The factors, which previously exhibited significant differences among both groups, were subjected to more investigation through univariate and multivariate regression analysis to elucidate the effect magnitude of these factors on birth weight (Table 5). The univariate regression analysis revealed that the pre-pregnancy weight, during-pregnancy weight, pre-pregnancy BMI, and MUAC were not associated with birth weight (P > .05). On the other hand, the gestational age was significantly associated with the birth weight (P < .05). The multiple regression analysis reinforces the results of the univariate regression analysis regarding the association of gestational age with birth weight. In contrast to the univariate analysis, the multiple regression analysis indicated the presence of a possible association between pre-pregnancy weight and birth weight (P = .024). Other factors were excluded from the multiple models, indicating the absence of their actual effect on birth weight (Table 5).
Univariate Simple and Multiple Linear Regression Model Examining the Associations Between Maternal Risk Factor Variables and Birth Weight, Taiz, Yemen, 2021.

Discussion
Low birth weight (LBW) exerts a profound effect on the morbidity and mortality of infants and a possible effect on their health status during adult life; a recent study reported that LBW seems to be a risk factor for severe COVID-19 in adults. 31 LBW as a public issue should be considered by all healthcare providers, health academic institutions, and health-related authorities and agencies. The present study aims to investigate the prevalence of LBW and its potential associated factors in Taiz, Yemen. One of the significant findings of the current study is that the incidence of low birth weight was estimated to be 39.11%. This rate is higher than that reported in developed and developing countries; since it was 5%-7% and 19%, respectively. 32 It is more than 2-fold higher than estimated recently in Sana’a (Yemen), where the incidence was 18%. 33 Although the prevalence of LBW varies widely across and within countries, it is most common in low- and middle-income countries. 34 According to the joint UNICEF and WHO study in 2000, Yemen had the highest incidence of LBW among regional countries; Saudi Arabia (11%), Kuwait (7%), Qatar (10%), Oman (9%), Lebanon (6%), Syria (6%), Algeria (7%), Libya (7%), Tunisia (7%) and Bahrain (8%), Jordan (10%), Morocco (11%), Egypt (12%), Nigeria (14%), and Sudan (31%). 35
The current study revealed that the age of mothers was not associated with birth weight. However, the percentage of the 26 to 35 age group of mothers with LBW newborns was higher than the other 2 age groups, 15 to 25 and 36 to 45 years old (50% v 27.3% and 22.7%, respectively). In the same line as what was reported in a 2019 registry-based study of low birth rate incidence in Northern Tanzania by Mvunta et al, 25 74.2% of mothers with LBW newborns were in the age group 20 to 34 years old. Similarly, a 2017 study on risk factors of LBW in Sana’a (Yemen) by Shuaib and Frass 33 reported that 73.5% of mothers giving LBW infants were in the age group 20 to <30 years old. The other maternal sociodemographic characteristics, education level, economic status, residence place, and health status, were not associated with birth weight.
This study showed that the foods, including fruits, vegetables, meat, fat, and milk products, that mothers had taken were not significantly correlated with birth weight. Taking folic acid as a supplement was not significantly correlated with birth weight.
Our study revealed that the pre-pregnancy weight, during-pregnancy weight, pre-pregnancy BMI, and MUAC of mothers were significantly associated with the birth weight since these parameters in mothers who delivered NBW newborns were significantly higher than those of mothers who delivered LBW newborns. Although the study on risk factors of LBW among rural and urban Malaysian women by Kaur et al 36 agreed with our study regarding MUAC but reported that pre-pregnancy BMI and gestational weight gain were not associated with LBW. 36 It is well known that maternal undernutrition is a crucial contributor to low birth weight (LBW). Underweight mothers (BMI < 18.5 kg/m2) are more likely to deliver LBW newborns due to intrauterine growth retardation. 37 An Ethiopian systematic review showed that maternal BMI < 18.5 kg/m2 is an LBW risk factor. 38 However, our study showed that the mean pre-pregnancy BMI was within normal weight for both mothers groups, while the mean during-pregnancy BMI was slightly upraising to overweight for both mothers groups, which could be considered a logical rise due to the expected weight gain during pregnancy.
The results revealed that gender was not associated with birth weight. This result agrees with several studies, such as that reported in Sana’a (Yemen), 33 Southern Ethiopia, 39 and North West Ethiopia. 40 A conflicting finding was reported in the previous studies, where the female gender was found to be at risk of having LBW as in the United Arab Emirates, 28 South Africa, 41 Ghana, 42 Burkina Faso, 43 and Iran, according to a systematic review and meta-analysis study. 27 The same finding was reported in this study regarding birth order since the birth order was not associated with birth weight. This result disagrees with what was reported in the United Arab Emirates 28 and Kashmir, 44 where the first child order was more likely to be LBW.
Notably, gestational age was significantly associated with birth weight, where newborns born before 37 weeks of gestational age could be more likely to be LBW by 9 times than newborns born after 37 weeks of gestational age. This finding agrees with several studies, such as Ethiopia,38,40 Northern Tanzania, 25 United Arab Emirates, 28 Oman, 45 Ghana, 42 and South Africa. 41 According to Guideline, 7 pre-term birth was considered one of the factors leading to LBW.
The current study showed maternal hemoglobin level was not associated with birth weight. This finding is in the same line as the Indian study 46 and Ghana study 42 but in contrast to the Northern Ethiopian hospital-based study conducted in 1017 by Gebregzabiherher et al, 47 since newborns of the mothers with normal hemoglobin were less likely to be LBW, as well our study in conflict finding to studies44,48 and as maternal hemoglobin level was found to have a significantly strong association with incidence of LBW newborns.
However, the strength of this study as it is the first comparative cross-sectional study addressing the LBW and its anticipated risk factors at Taiz (Yemen). The main limitations of this study were that it was conducted at only one hospital. Furthermore, the medical records included insufficient biochemical test results for mothers during the pregnancy, and the biochemical screening for their newborns was unavailable. In addition, the anthropometric measurements were not carefully considered within the medical records, which enforces teamwork to take the anthropometric measurements in the first hours of birth, so many mothers were excluded as samples for this study. Unfortunately, nutritional awareness among pregnant women was poor. Also, the daily energy intake is not calculated, and the recall method for assessing food consumption could not be implemented in this study as the Yemeni dishes have no food composition tables yet.
Conclusion
LBW is one of the public health challenges experiencing a profound effect on the morbidity and mortality of newborns in developing countries, and Yemen is not an exception. LBW is prevalent among pregnant mothers attending hospitals and clinic centers in Taiz (Yemen). As a complicated health problem, LBW should be considered and addressed by healthcare institutions, healthcare providers, and researchers. It is noteworthy to indicate that good healthcare services should be provided to manage LBW incidents.
Supplemental Material
sj-pdf-1-gph-10.1177_2333794X231203857 – Supplemental material for A Comparative Cross-sectional Study on Prevalence of Low Birth Weight and its Anticipated Risk Factors
Supplemental material, sj-pdf-1-gph-10.1177_2333794X231203857 for A Comparative Cross-sectional Study on Prevalence of Low Birth Weight and its Anticipated Risk Factors by Assmaa A. Alsamae, Hala A. Elzilal, Eman Alzahrani, Hala M. Abo-Dief and Mujeeb A. Sultan in Global Pediatric Health
Footnotes
Author Contributions
All authors made a substantial contribution to the concept, design of this work; M.A.S and A.A.A. contributed in acquisition and interpretation of data, All authors approved the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by deanship of scientific research, Taif University, Taif, Saudi Arabia.
Consent for Publication
Not applicable.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.