
Abstract
Neuroblastomas commonly metastasize to the cranium and orbit, although other facial bones were less implicated. In this report we present a 3 years old child with metastatic neuroblastoma to the mandible that presented with swollen right jaw. The first assessment of the head with computed tomography revealed soft tissue mass with permeative lytic changes of the osseous structures centered on the right mandible, as well as osteo-meningitis metastases. These masses were proven to be metastatic lesions from intra-abdominal neuroblastoma of the right adrenal gland. Over the previous several years, only 29 cases of neuroblastoma metastasis to the mandible have been reported in the literature.
Introduction
The neuroblastoma (NB) is the most frequent pediatric solid tumor metastatic in 50% at the time of the diagnosis. However, the occurrence of metastases within the mandible, one of the facial bones, remains a relatively infrequent phenomenon, with only a handful of documented instances in the medical literature. In this report we discuss the radiological features of the case of a 3 years old child with mandibular metastatic neuroblastoma. We aim to expand our understanding of the less-common trajectory that neuroblastoma can take, emphasizing its infrequent involvement within the mandible.
Case Report
We report the case of a 3-year-old child who was referred to our hospital with a fast-developing and mildly painful enlargement of the right mandibular. Clinical examination revealed an apyretic infant with scalp swelling and a fixed mass on the left body of the jaw. This was coupled with moderate facial asymmetry. Bilaterally, numerous enlarged cervical lymph nodes were palpable.
Computed tomography (CT) of the head revealed permeative lytic alterations of the osseous structures of the mandible with aggressive periostitis and an invasive soft tissue mass centered at the right body of the mandible, as well as imaging of a distinct masticator muscle soft tissue mass and bilateral cervical lymph nodes (Figure 1). The head imaging showing a strongly enhancing extra-axial lesion with a wide dural base with bony erosion (Figure 2).
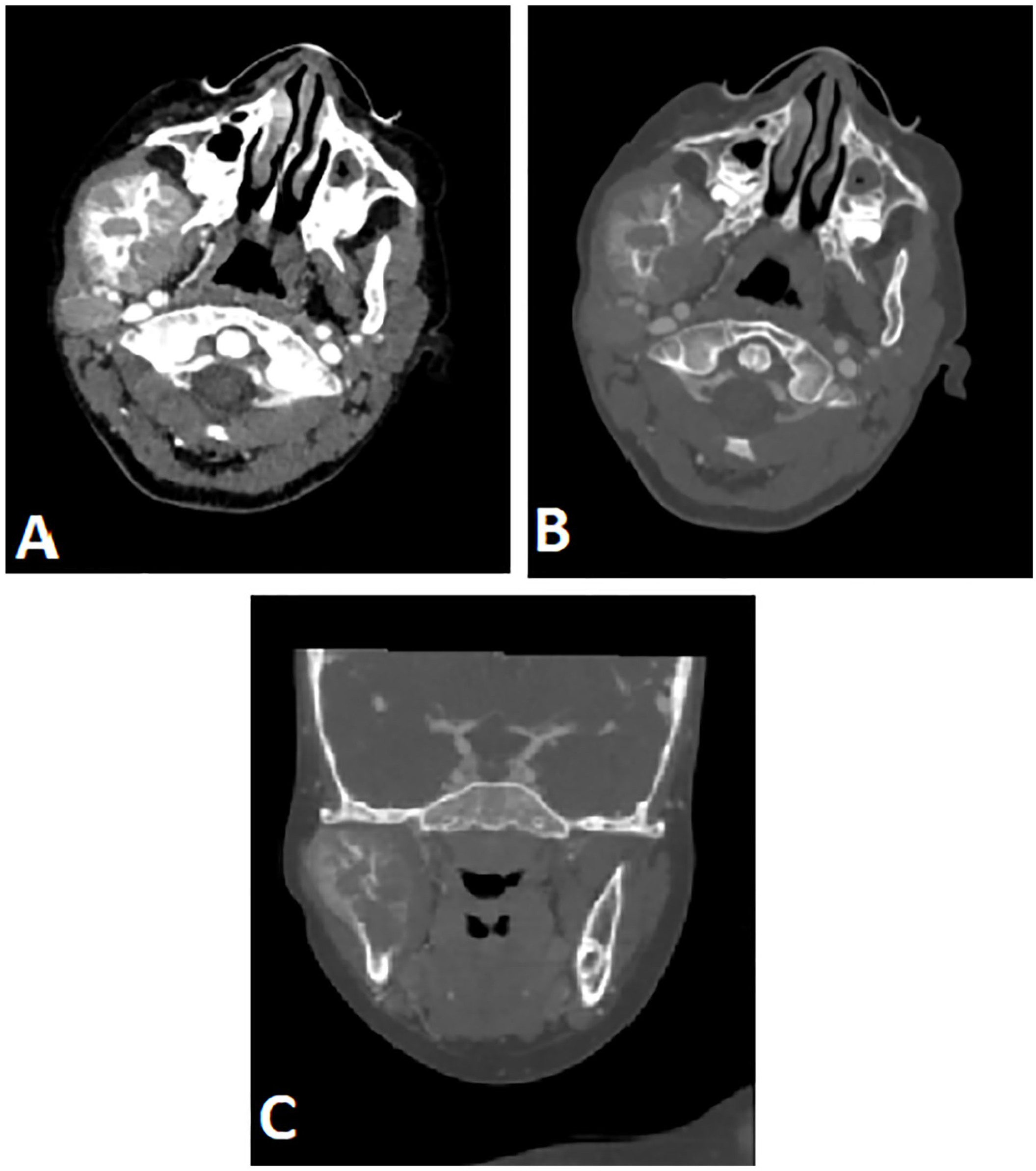
Axial CT images shows a soft tissue mass centered on the ramus of the right mandible (A) with bone reconstruction in axial (B) and coronal images shows aggressive periosteal reaction centered at the ramus of the right mandible (C).

Axial CT of the head before (A) and after (B) enhancement shows a strongly enhancing extra-axial lesion with a wide dural base.
Based on these findings, we proceeded with our investigation to determine the placement and extent of both primary and metastatic lesions. And we identified a right retroperitoneal adrenal tumor that was well confined, with calcifications and faint enhancement, measuring 81 × 73 × 89 mm (Figure 3), along with numerous mediastinal and abdominal lymph nodes (Figures 3B and 4A). and lytic mass of the chest wall involving the eighth right posterior costal arc (Figure 4B).

An axial CT of the abdomen reveals a massive soft tissue mass with a considerable mass impact on the right kidneys and liver (A). There are also numerous retroperinoneal lymph nodes encasing the arterial vasculature with no intraspinal extension (B).
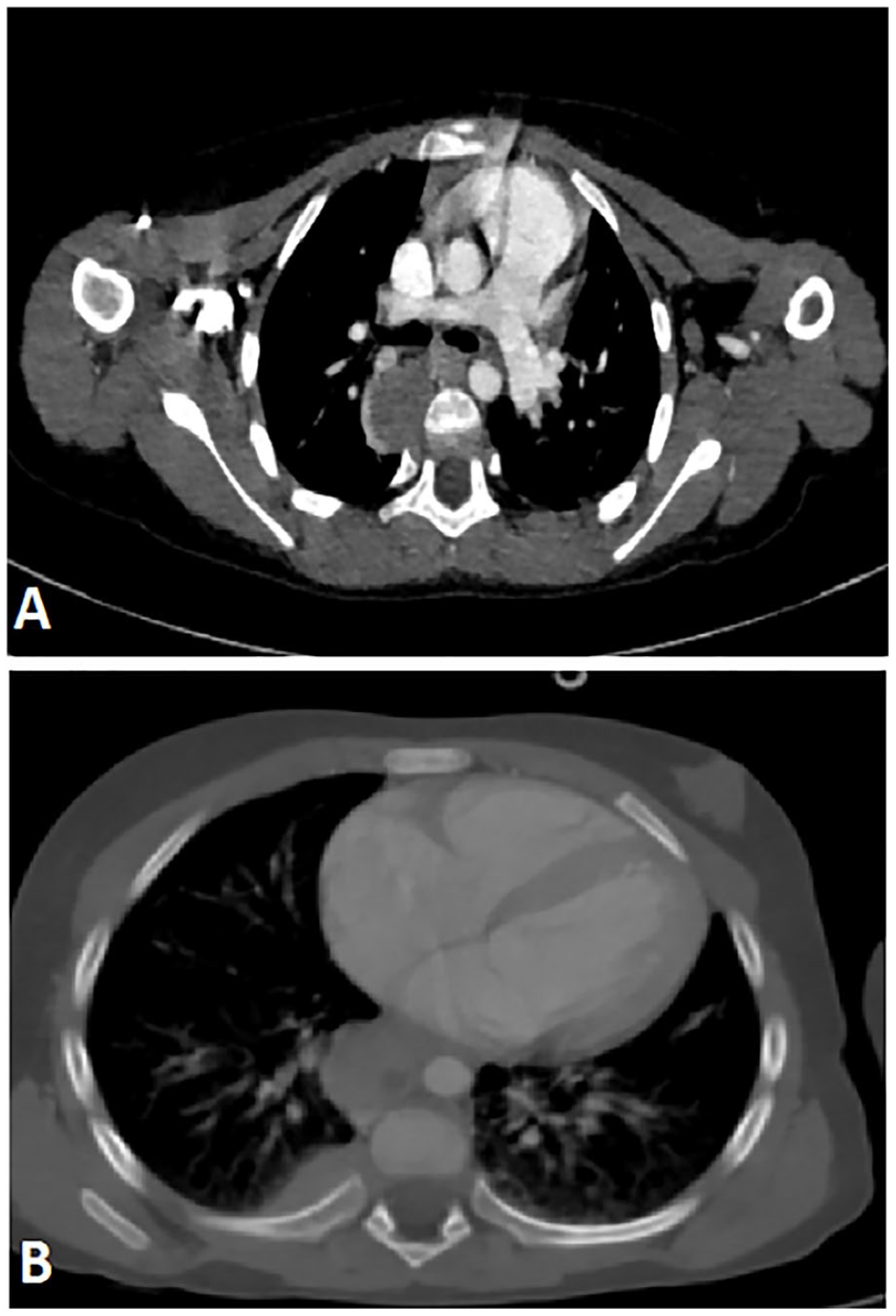
Axial CT of the chest shows mediastinal lymph nodes (A) and a lytic mass of the chest wall involving the eighth right posterior costal arc (B).
Discussion
Neuroblastic tumors are a diverse category of embryonic cancers that arise from neural crest cells. Neuroblastoma accounts for 10% to 15% of all juvenile cancers. The average age of diagnosis is 22 months. The majority of neuroblastoma cases are sporadic, however about 1% to 2% have familial transmission. 1 At least half of the patients had metastases at the time of diagnosis, with bone marrow and bone being the most prevalent locations of metastases. Therefore, the mandible is a rare location for metastases, only a few published reports on mandibular metastases in neuroblastoma, and the majority of case series were from before the contemporary multimodality treatment for metastatic neuroblastoma was developed. 2
Neuroblastoma patients in addition of the palpable abdominal anomalies and/or symptoms associated to mass effect on surrounding organ systems, the mandibular metastasis has the potential for substantial morbidity, potentially interfering with dentition and oral function, and frequently leading to major esthetic problems. 3
The presence of tumor cells in a bone marrow aspirate or a typical histopathologic examination of tumor tissue can be used to confirm the diagnosis of NB. Elevated urine vanyllylmandelic acid (VMA) and homovanillic acid (HVA), dopamine, serum ferritin, and neuron-specific enolase levels can help establish the diagnosis. 4
CT and MRI are commonly used for definitive imaging of mandibular metastasis, with the latter being the preferred radiographic modality for identifying soft tissue abnormalities because of its higher specificity and sensitivity and stronger soft tissue contrast. 5 Metastatic lesions in neuroblastoma, like other osseous metastases, are generally osteolytic with extraosseous soft tissue expansion, 3 with T2 hyperintense signal, T1 hypointense signal, restricted diffusion, and heterogeneous enhancement after Gado injection.
The usual functional imaging modality for detecting skeletal metastases is the iodine-123-MIBG (123I-MIBG) scan, which is positive in 90% of neuroblastomas and can differentiate between the latter and other mandibular bone lesions. However, MIBG scans for the maxillo-mandibular area must be carefully reviewed for metastasis identification due to the close existence of the salivary glands, which have strong sympathetic innervation that can interfere with the diagnosis of the tumoral cells of neuroblastoma. 6
Because of the elevated red marrow vascularity of the mandibular body and angle, the lesion’s location within the ramus of the right mandible suggests hematogenously disseminated original tumor, 7 like the case of our patient.
The most recent findings 3 show that, in contrast to prior publications, 2 mandibular metastasis in neuroblastomas does not always have a poor prognosis when compared to individuals with metastases at other bone sites. Three-year survival with multimodality therapy in these patients. Many of these survivors, however, have treatment-related dentofacial abnormalities that require extensive rehabilitation to restore oral function. 3
The recommended strategy for managing neuroblastomas in children involves a comprehensive approach that begins with surgically excising the tumor, followed by targeted radiation therapy directed at the surgical site. This method has proven to be highly effective, particularly for localized tumors, resulting in a commendable cure rate ranging between 85% and 90%. Additionally, palliative radiation therapy has demonstrated its effectiveness in alleviating bone pain arising from metastases. However, it’s important to note that the current consensus is that chemotherapy’s effectiveness in managing advanced neuroblastoma is limited.
Concurrently, the research underscores the critical role of radiotherapy not only in preventing relapse and treating measurable disease but also in managing concurrent dental disturbances and complications associated with neuroblastoma treatment, which include disrupted dental development and a heightened risk of dental abnormalities. 8
For high-risk neuroblastoma, our patient received conventional multi-modality therapy, including high-dose chemotherapy, anti-GD2 monoclonal antibody therapy and radiation therapy. The size of the mandibular growths continued to enlarge. Palliative radiation therapy was initiated for the mandible. Despite these efforts, the disease continued its progression, and sadly, the patient passed away 6 months after being diagnosed with neuroblastoma.
Conclusion
The occurrence of neuroblastoma with metastases in atypical sites, such as the mandible, introduces a diagnostic complexity. Recent studies challenge historical poor prognosis associated with mandibular metastasis. Management typically involves surgical resection and targeted radiation therapy, offering promising outcomes for localized tumors. However, treatment-related dentofacial issues necessitate comprehensive rehabilitation efforts.
Footnotes
Author Contributions
All authors contributed to this work. All authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Written informed consent for publication was obtained from the legally authorized representative of the patient.