
Abstract
Objective. This study aims to investigate compliance and the influencing factors related to pediatric tuberculosis patients who are undergoing treatment with anti-tuberculosis drugs in the Sichuan Province of China. Methods. A questionnaire survey was conducted between March 2019 and March 2021. The survey was distributed to caregivers of children aged 0 to 14 who had been diagnosed with pulmonary tuberculosis. These children had been receiving oral anti-tuberculosis drug treatment for more than 1 month. The survey was administered at the pediatric infection departments of West China Second University Hospital, Sichuan University, and The First People’s Hospital of Ganzi Prefecture. Results. The study revealed a notable lack of medication adherence among the pediatric patients. Through multiple linear regression analysis, it was determined that several factors played a role in influencing medication adherence among children with tuberculosis. These factors include the educational level of the parents, the frequency of daily anti-tuberculosis drug prescriptions, and the parents’ comprehension of the disease. All of these factors showed statistically significant influence on medication adherence among pediatric tuberculosis patients (all P < .05). Conclusion. In order to enhance adherence among pediatric patients undergoing anti-tuberculosis treatment, it is imperative to focus on reinforcing health education, particularly for parents with lower educational attainment and limited understanding of the disease.
Introduction
Tuberculosis (TB) is a chronic infectious disease, one of the oldest to affect humans. According to reports, tuberculosis remains the primary cause of human deaths worldwide. 1 In 2022, China held the third-highest number of tuberculosis cases globally, following India and Indonesia, according to a WHO report. 2
The treatment of tuberculosis extends over a prolonged period. The standard approach to treating tuberculosis involves oral anti-tuberculosis medications. In China’s TB planning guidelines, the briefest treatment regimen spans 6 months. For conditions like tuberculous meningitis and osteoarticular tuberculosis, treatment may extend to 12 months, while drug-resistant cases necessitate even more extended courses. The effectiveness of treatment exhibits a direct correlation with adherence to anti-tuberculosis therapy. It has been established that a considerable portion of tuberculosis patients exhibit poor adherence to anti-tuberculosis treatment.3-5 Currently, the limited adherence of tuberculosis patients to medication has evolved into a significant barrier in controlling the global tuberculosis epidemic. 6 The inadequate commitment of these patients to treatment could potentially lead to the persistence, escalation, recurrence, emergence, and widespread propagation of drug-resistant tuberculosis bacilli, culminating in severe ramifications. 7 Previous studies have indicated that the adherence of adult patients with pulmonary tuberculosis is influenced by factors such as their registered place of residence, educational attainment, and economic status, as well as their comprehension of the disease and adverse drug reactions.3,8,9 Nonetheless, there exists a paucity of research concerning medication adherence among pediatric tuberculosis patients.
In the present investigation, questionnaires were employed to assess the adherence status and associated factors relating to anti-tubercular treatment in pediatric tuberculosis patients within China’s Sichuan Province.
Materials and Methods
Ethical Approval and Informed Consent
The research study received approval from the Ethics Committee of West China Second University Hospital (No. 2019-055). Prior to administering the questionnaire, written parental consent was obtained from all participants.
Research Design
This retrospective cross-sectional survey study employed a questionnaire to investigate parental knowledge regarding their child’s diagnosis and treatment.
Study Subjects
Children who had tuberculosis and were treated between March 2019 and March 2021 at the pediatric infection departments of West China Second University Hospital and the First People’s Hospital of Ganzi Prefecture in Sichuan province were included in this study. The inclusion criteria were as follows: (1) the child’s age was ≤14 years old; (2) they met the criteria for confirmed TB or unconfirmed TB according to accepted consensus agreements 10 ; (3) the child had received anti-tuberculosis treatment for more than 1 month, and their caregiver had received TB knowledge and medication health education on at least 3 occasions; (4) the caregiver possessed normal communication and comprehension abilities.
The exclusion criteria were: (1) inability to understand the content of the informed consent form and the questionnaire; and (2) failure to cooperate with the investigation or provide informed consent.
Sample Size
The sample size required for conducting a multiple linear regression analysis should ideally be 10 times the number of independent variables. In this study, there were 20 independent variables, which implies an anticipated sample size ranging between 200 and 300 participants. Moreover, considering a 10% rejection rate, factors such as the unique clinical circumstances of the patients, the questionnaire recovery rate, and the possibility of invalid questionnaires were taken into account. Ultimately, the estimated sample size for this study was determined to be 220 participants.
Questionnaire Design
Employing a self-developed unified questionnaire (Supplemental Appendix 1), on-site face-to-face interviews were conducted as a means of data collection. Following a review of pertinent literature, the researchers extended invitations to 5 experts with expertise in nursing, pediatric tuberculosis diagnosis, and treatment. These experts were engaged to evaluate and refine the preliminary version of the questionnaire prior to the actual experiment. Subsequently, the questionnaire underwent revisions based on their feedback, with a focus on enhancing its reliability and validity.
Questionnaire Content (Variable of Questionnaire)
The questionnaire comprised mainly 5 sections: (1) basic information of the caregiver; (2) general condition of the children and tuberculosis; (3) medication adherence scale following the methods outlined by Weihua X 11 ; (4) Medication behavior questionnaire of children in parental custody; and (5) Knowledge on TB.
The medication adherence score indicates the extent to which a patient adheres to the prescribed drug. 11 Medication adherence refers to how well a patient follows medical advice and takes the medication as prescribed. 12 It can be determined by comparing the timing, quantity, and dosage of medication administration with the doctor’s prescription. Consistently following the physician’s instructions for taking the medication over the long term is considered good drug compliance. For measuring medication adherence among patients with chronic diseases, a medication adherence scale based on Xu’s methods was utilized, which is widely accepted for its reliability and validity. Prior to investigating anti-tuberculosis treatment adherence in children with pulmonary tuberculosis, the Cronbach’s α coefficient was calculated as .733. The scale’s total score is 25, with higher scores indicating better compliance.
The TB prevention and treatment knowledge questionnaire has undergone thorough review by numerous studies and has been designed with clinical expertise. Five experts in relevant fields participated in modifying, pre-testing, and refining the questionnaire’s content before finalization. The total score on this questionnaire ranges from 0 to 13, with higher scores reflecting greater knowledge related to TB.
Questionnaire Implementation
The questionnaires were collected by independent evaluators. Before the investigation, we provided training to these evaluators for data collection. The training aimed to ensure that all questions in the questionnaires could be understood accurately by the respondents. Throughout the investigation, in cases where respondents were unable to complete a written questionnaire, either the respondents themselves or the evaluators completed the questionnaires on their behalf.
Cross-checks on the collected questionnaires were conducted to ensure their completeness. This involved verifying the key and reverse items and engaging with the respondents promptly to ensure accurate and timely responses, thereby minimizing the likelihood of incorrect answers.
Statistical Analysis
Data analysis was carried out using SPSS 20.0 software, employing double data entry. The continuous data in this study exhibited a normal distribution. Descriptive analysis was used to depict the subjects’ characteristics, while a t-test was employed for single-factor analysis. For multivariate linear regression, factors that displayed statistical significance in the univariate analysis were included. A significance level of P < .05 was utilized to determine statistical significance.
Results
Characteristics of the Study Participants
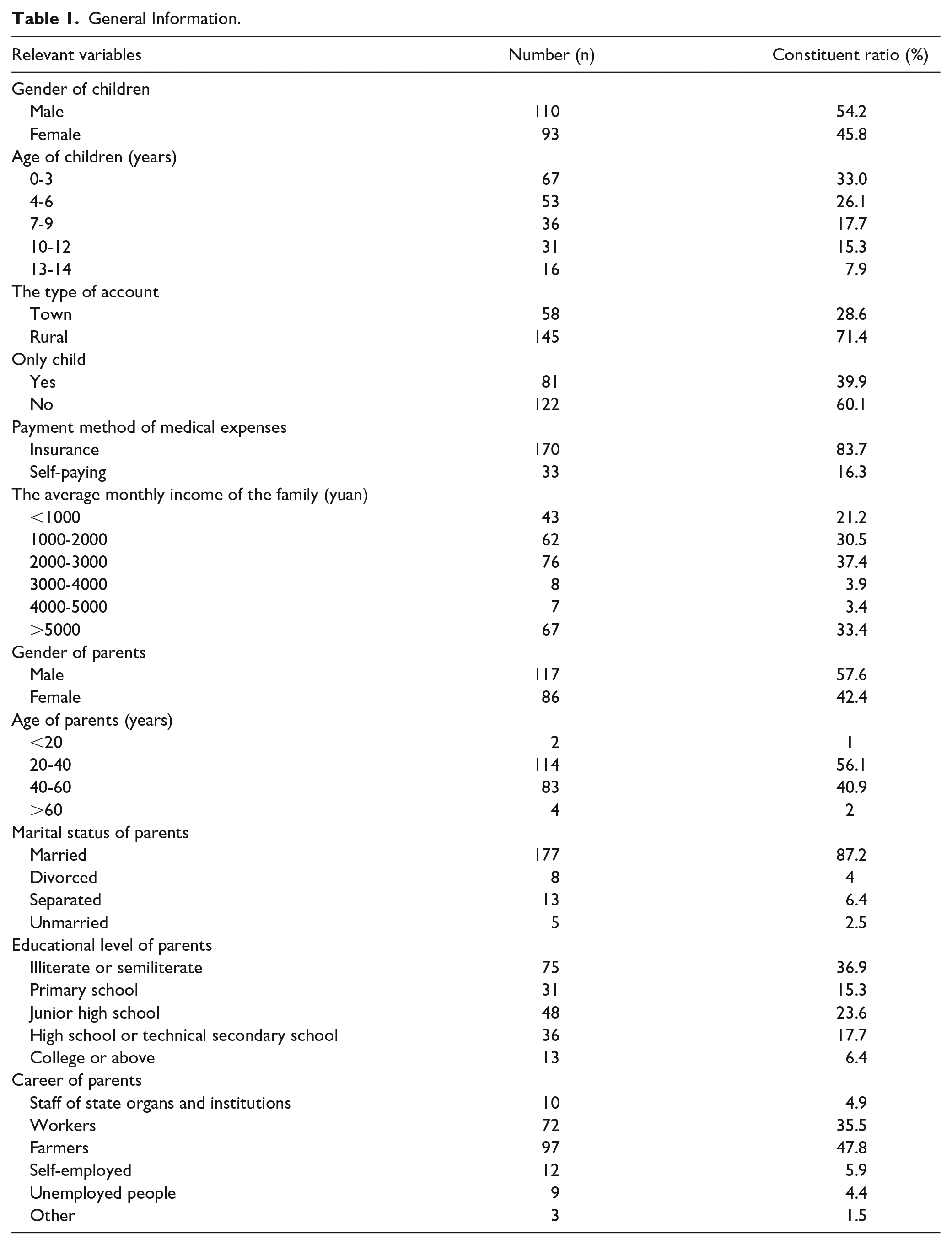
This study gathered a total of 222 questionnaires, out of which 203 were returned, resulting in an effective recovery rate of 91.44%. It took participants approximately 5 to 10 minutes to complete the questionnaires. Any missing items were addressed after being identified by the investigators. Reverse questions were responded to as required, and questionnaires without identical responses were deemed valid. Of the children diagnosed with tuberculosis, 59.1% were under the age of 6, 71.4% hailed from rural areas, 52.5% of the children’s parents had received a primary school education or less, and 51.7% had a per-capita income of less than 2000 RMB. Detailed general information is shown in Table 1.
General Information.
Parents of Children With TB Related Knowledge
The findings from the survey on TB knowledge among parents of young children revealed a range of scores, with the lowest being 0 and the highest reaching 13 points. The average score stood at 8.79 ± 3.52 points. Notably, the accuracy rate for certain aspects was less than 50%. Specifically, respondents exhibited less than a 50% correct rate concerning the duration of TB treatment, the primary approach for preventing TB in children, the contagious nature of certain tuberculosis types, and the timeframe after completing formal treatment when tuberculosis patients cease to be contagious (Table 2).
Parents’ Knowledge of Tuberculosis.

The Status Quo of Medication Adherence in Children With Tuberculosis
Children with tuberculosis who underwent medication administered by their parents achieved scores ranging from 45 to 81, with an average score of 64.15 ± 7.78.
Analysis of Drug Dependence in Children With Tuberculosis
The results of the univariate analysis indicated significant variations in anti-tuberculosis treatment adherence among children with differing parental educational levels, occupations, family per capita monthly income, ethnic backgrounds, types of residence (rural or urban), medication duration, frequency of medication, occurrence of side effects, and caregivers’ knowledge of the disease (P < .05). No correlations were observed between the age of parents, marital status, the child’s age, being an only child, the quantity of drugs administered, and medication adherence (P > .05) (Table 3).
Medication Adherence in Children With Different Characteristics of Tuberculosis.

P < .05.
Multi-Factor Analysis of Drug Dependence in Children With Tuberculosis
A multiple linear regression analysis was carried out using the medication adherence of TB children as the dependent variable (factor variable) and statistically significant variables from the univariate analysis as independent variables (parameters). The results of this analysis revealed that several factors significantly influenced medication adherence among children with tuberculosis: the educational level of the parents, the number of daily anti-tuberculosis drug prescriptions, the specific hospital visited by the children, and the parents’ knowledge of the disease (all with P < .05). The allocation of influencing factors regarding medication compliance in children with pulmonary tuberculosis is presented in Table 4. The details of the multiple linear regression analysis are shown in Table 5.
Evaluation Table of Influencing Factors of Medication Compliance in Children With Pulmonary Tuberculosis.

Multi-Weight Linear Regression Analysis of Medication Adherence Among Children With Tuberculosis.

P < .05.
Discussion
Children diagnosed with tuberculosis exhibited an average medication adherence score of 64.15 ± 7.78 points. Only 34 cases (16.9%) achieved a compliance score exceeding 70 points, while the majority of children demonstrated low medication adherence. Previous studies13-16 have indicated that medication adherence among adult tuberculosis patients was notably suboptimal. Likewise, medication adherence among diverse children with chronic illnesses also proved inadequate,17-20 aligning well with our findings.
The fifth China Tuberculosis Epidemiological Sampling Survey disclosed that regions with low economic income in rural areas showed a heightened prevalence of tuberculosis. 21 Within this survey, 71.4% of families hailed from rural backgrounds, with correspondingly low average family incomes. In a broader context, parents of children with tuberculosis exhibited limited educational attainment, with the highest percentage (52.5%) having achieved a primary school education or less. Among the population, 59.1% of children were aged between 0 and 6 years. Following infection with Mycobacterium tuberculosis, the incidence rate for children under 5 years old was 33.3%, decreasing to 19.1% for those aged 5 to 14 years, and further dropping to 8.7% for children above 14 years, 22 underscoring the increased vulnerability of younger children to tuberculosis infection.
During the course of treatment, children experienced drug-related side effects at a rate of 39.4%. These findings were consistent with prior research, revealing that the most prevalent adverse effects included nausea, vomiting, various gastrointestinal reactions, impairment of liver function, and rash. 23 This study underscores that children experiencing drug side effects tend to display lower medication adherence compared to those without such effects. Meng et al 24 corroborated these results, identifying adverse drug reactions as the primary factor influencing treatment compliance among patients with pulmonary tuberculosis. Hence, when disseminating health education to parents, it becomes imperative to apprise them of potential drug side effects and appropriate treatment modalities.
Zhemei et al 25 discovered that a higher level of education is associated with greater compliance. Regression analysis of drug adherence in children with tuberculosis revealed a correlation between drug adherence and parental education. Children whose parents possessed a higher level of education adhered to medication therapy more diligently compared to those whose parents had a lower level of education. This might be attributed to the fact that highly educated parents possess multiple channels of information, a better understanding of drug administration methods, and other disease-related information, enabling them to recognize the significance of prolonged drug usage. As a result, the supervision provided by such parents amplifies children’s commitment to their medication regimen. This urges us to take into account the educational background of parents, evaluate their capacity to receive and comprehend pertinent information, enhance the dissemination of disease-related knowledge and proper drug administration techniques among parents with lower educational backgrounds, and assess parents’ proficiency, with re-education as an option if necessary.
Furthermore, disparities in medication adherence were observed among children with tuberculosis undergoing treatment at the 2 hospitals. Children treated at West China Second University Hospital, Sichuan University exhibited higher compliance rates. This discrepancy could stem from the elevated level of economic development in Chengdu, the provincial capital. Previous research has emphasized household income as a significant influencer of drug dependency,26-28 thereby suggesting that we should prioritize children with tuberculosis in regions with relatively modest economic conditions. In such areas, it is imperative to augment investments in medical care, enhance health education for parents, and bolster medication adherence.
\The frequency at which a child with tuberculosis takes medication has been identified as a factor influencing medication adherence. Previous research on tuberculosis patients has revealed a negative correlation between the frequency of medication administration and patient adherence. However, the present study has uncovered that children who took the medication once per day exhibited a lower rate of adherence, whereas a single child who took the medication 3 times per day demonstrated a higher rate of adherence. This discrepancy could potentially be attributed to the significant differences between the distributions of samples of children with tuberculosis who took the medication once daily compared to those who took it more than 3 times a day.
Among the 4 children who were prescribed 3 daily doses of medication, 2 were diagnosed with drug-resistant tuberculosis, while the remaining 2 were diagnosed with extrapulmonary tuberculosis. Due to the complexity of the disease, parents were more acutely aware of its severity and were consequently more vigilant in overseeing their child’s treatment, resulting in increased medication adherence.
Our findings have illuminated that parental comprehension of their child’s tuberculosis condition constitutes one of the key factors influencing medication adherence among children with tuberculosis. A stronger grasp of tuberculosis was positively associated with higher compliance with anti-tuberculosis treatment in children. Previous studies29-31 have similarly demonstrated that a solid understanding of anti-tuberculosis drugs among adult tuberculosis patients significantly impacts treatment adherence. Additionally, medication adherence in tuberculosis patients displays a positive correlation with their understanding of the prescribed drugs.
On the one hand, the more comprehensive a parent’s understanding of tuberculosis, the better their awareness of the significance of adhering to medication regimens and potential drug side effects. On the other hand, this knowledge can mitigate the fear of the disease, along with misconceptions and resistance during the course of treatment. As a result, healthcare professionals should prioritize enhancing the comprehension of parents with children suffering from pulmonary tuberculosis. This can be achieved through comprehensive, systematic, and easily comprehensible health education delivered through various channels to ultimately bolster medication adherence among children.
The present study is constrained by the several limitations. Firstly, the sample size, number of cases, and size of the research facility were all modest, which has implications for the generalizability of the findings. Additionally, the total number of illnesses is not clearly stated, potentially introducing bias in the representation of children with tuberculosis across the entire Sichuan Province. Secondly, although this study explored the relationship between demographic data, disease status, parental knowledge, and parents’ compliance with anti-tuberculosis treatment, it fell short of comprehensively examining all influential factors. Notably, no questionnaire survey was administered among the children themselves, precluding an assessment of how their thoughts and actions contribute to adherence to anti-tuberculosis treatment. Thirdly, the study solely employed a cross-sectional survey at a specific point in time to gage drug usage. Regrettably, it neglected to conduct a continuous follow-up survey that would have provided a more profound comprehension of the pertinent factors evolving over time. Such an approach is essential for gaining a comprehensive understanding of the dynamics surrounding tuberculosis treatment.
Conclusion
In the Sichuan Province of China, medication adherence among children with pulmonary tuberculosis remains low. This issue is primarily influenced by factors such as parental education, family income, parental understanding of the disease, and medical accessibility. Consequently, there is a compelling need to augment healthcare investment in regions facing economic and cultural disadvantages. Furthermore, the provision of comprehensive health education services concerning the disease, the assurance of uninterrupted nursing care, and the facilitation of equitable distribution of top-tier medical resources are imperative steps toward significantly enhancing medication adherence and the recovery rate among children with pulmonary tuberculosis.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X231199360 – Supplemental material for Assessment of Factors Associated With Anti-Tubercular Treatment Compliance in Children: A Cross-Sectional Study
Supplemental material, sj-docx-1-gph-10.1177_2333794X231199360 for Assessment of Factors Associated With Anti-Tubercular Treatment Compliance in Children: A Cross-Sectional Study by Lihong Gao and Biru Luo in Global Pediatric Health
Footnotes
Author Contributions
Lihong Gao participated in project design, data collection and processing, and wrote the manuscript. Biru Luo was involved in project design, data collection and processing, as well as manuscript editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.