
Abstract
Wilson disease is a rare autosomal recessive genetic disease, caused by the mutation of the ATP7B gene leading to decreased secretion of serum ceruloplasmin in blood and decrease biliary excretion of copper leading to toxic level accumulation in the liver, brain, kidney, and cornea, resulting in development of characteristic liver disease and neuropsychiatric symptoms. Our case presented with mainly clumsiness and gait abnormality without any psychiatric component and any history of liver disease. A 13-year old male, born out of non-consanguineous marriage, presented with clumsy walking and slurring of speech. The child also complained of poor handwriting and slipping of slipper from foot, without any history of abnormal behavior and poor scholastic performance. On examination gait was abnormal with sidewise swaying, increased muscle tone with rigidity and bilateral flexor plantar reflex. Slit lamp examination of eyes revealed bilateral Kayser-Fleischer rings. Serum ceruloplasmin was low (0.03 g/L) and 24-hour urinary copper was high (119.64 μg/day). MRI brain showed B/L putamen hyperintensity and panda sign suggestive of Wilson disease. After the diagnosis of Wilson disease was made, patient was treated with penicillamine and zinc. Child was also followed-up and re-examination showed slight improvement. Though not rare, Wilson disease is an uncommon entity with varied presentations and disabling consequences. Hence high index of suspicion and clinical correlation is required to diagnose it. Early initiation of treatment and good compliance ensure a better outcome.
Introduction
Wilson disease is an autosomal recessive, copper storage disease due to mutation in ATP7B gene, leading to decreased secretion of ceruloplasmin in blood and decrease in excretion of copper in bile. 1 Wilson disease occurs due to excessive accumulation to toxic level of copper, mainly in liver and in others organs like brain, kidney, and cornea. 2 The majority of patients with neurological Wilson disease have clinical features of dysarthria and/or abnormal movement. 3 The most common psychiatric and behavioral manifestations are depression, personality changes, and irritability. 4 Interestingly, this case did not present with clinical features of liver disease, psychiatric and abnormal behavior, or deterioration of scholastic performance; which are the typical presentations of Wilson disease.
Clinical Description
A 13 year old male, born from parents of non-consanguinous marriage, was admitted with complaints of clumsiness in walking and slurring of speech for last 1 year. Clumsiness was gradual in onset, progressive in nature and the patient swayed to both sides walking with the slippers frequently slipping off the feet. Parents had also noticed deterioration of his hand writing but no history of poor scholastic performance and abnormal behavior. Child had no history of seizure, loss of consciousness, head trauma, jaundice, and any exanthematous fever. No complaints of joint pain and skin rash were present either. There was no family history of similar disease or unusual death.
On examination, the child was conscious and oriented and appeared to be always smiling (Figure 1). The height of the child was 157 cm, head circumference was 52 cm, and weight was 45 kg. In CNS examination, tone was increased with rigidity with bilateral planter downward. Complete blood count revealed hemoglobin value of 11.5 g/dL, total count of 10 410, and N/L (neutrophil/lymphocyte) of 42/34. The liver function test (LFT) and kidney function tests (KFT) reports were also normal. On the basis of the history, examination, and initial investigations, the diagnosis was narrowed to include neurodegenerative and metabolic diseases.

Showing smiling facies of patient.
Management and Outcome
In slit lamp examination of the eyes, bilateral Keyser-Fleischer (KF) ring was present (Figure 2). Serum ceruloplasmin was 0.03 g/L by nephelometry technique and 24-hour urinary copper was 119.64 μg/day (range 3-50 μg/day) by ICPMS (inductively coupled plasma mass spectrometry) and 132.93 μg/L (Range 2.00-80.00) as reported by Dr Lal Path Lab.

Showing bilateral KF ring slit lamp examination.
MRI brain showed bilateral putamen hyperintensity and panda sign suggestive of Wilson disease (Figure 3). Hence a diagnosis of Wilson disease was made and accordingly the patient was treated with penicillamine, zinc, and other supportive measures. The child was also followed up till 6 months and reexamination showed slight improvement was noted in terms of less swaying while walking and decrease in slurring of speech.
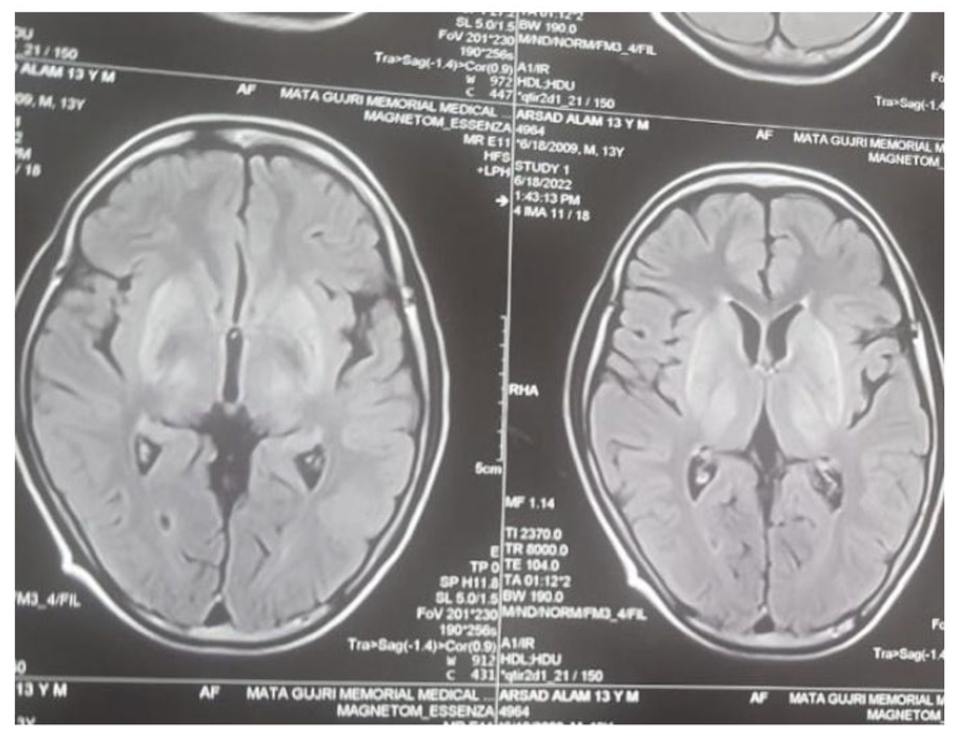
Showing MRI brain: bilateral hyperintensity of putamen and panda sign.
Ethical Approval and Informed Consent
Due consent was taken from the patient party for investigations, treatment, and publication of the case with images.
Discussion
Wilson disease is an autosomal recessive genetic disorder occurring due to mutation of the ATP7B gene on chromosome 13. 1 The gene encodes adenosine triphosphatase (ATPase) protein responsible for copper transport and defect of which leads to excessive accumulation of copper in brain and liver. 5
The clinical presentation of Wilson disease is mainly hepatic, neurological and psychiatric, and many have mixed symptoms. 6 Most of the patients of Wilson disease are diagnosed in between the ages 5 and 35 years. 6 The neurological findings occurring due to brain involvement are almost limited to motor system and typically present as movement disorder. The predominant movement disorders include dystonia, tremor, ataxia, and loss of motor control. Dystonia characterized by mask like face, rigidity, gait disorder, and pseudobulbar palsy (dysarthria, dysphagia, hypersalivation). 7 This patient typically presented with generalized dystonia as mentioned above. The KF ring is present more frequently in neurological cases with compared to hepatic involvement with fact that neurological findings occur at more advance age. 7 Brain MRI finding may be either normal or abnormal. Abnormal MRI findings in neurological Wilson disease show hyperintense signal changes in T1 and T2-weighted image in basal ganglia. 8 In this case, MRI typically showed hyper intensity in T1 andT2 in putamen.
Conclusion
Wilson disease is uncommon but not a rare disease, so high index of suspicion in a patient who present with movement disorder, and unexplained neurological findings and clinical correlation required to diagnose. Early starting of treatment and good compliance ensure better outcome.
Lesion Learnt:
High index of suspicion is required to diagnose a Wilson disease in patient suffering from movement disorder.
Always rule out Wilson disease in a patient suffering from unexplained neurological findings.
Early initiation of treatment and good compliance ensure better outcome.
Footnotes
Author Contributions
Akansha Anushree: Data acquisition, manuscript preparation.
Sudesh Kumar: conceptualization, design, editing.
Piyali Bhattacharya: conceptualization, design, editing.
Siddharth Tripathi: Data acquisition, manuscript preparation.
Nandita Chattopadhyay: Manuscript review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.