
Abstract
Conservative treatment of duodenal trauma in children has long been the first line of treatment for duodenal wall hematomas. However, it has rarely been described in duodenal perforations. Our purpose is to highlight the possibility of conservative treatment in selected cases of duodenal perforation. In the period between 2009 and 2022, 6 children were treated for duodenal injury following abdominal blunt trauma in the pediatric surgical emergency department. The clinical presentation, diagnosis and treatment are reported and analyzed. Three patients presented with duodenal hematomas, they were treated non-operatively with hospital stays between 12 and 20 days and good clinical outcome. One child presented with duodenal hematoma and retroperitoneal air bubbles; non-operative conservative treatment was carried with favorable results. The fifth patient had a duodenal perforation; he underwent a primary duodenal 2-layers closure. The last patient had a combination of duodenal hematoma and perforation involving 75% of the duodenal diameter for which he underwent a gastro-jejunostomy with pyloric exclusion. An isolated duodenal lesion can be subject to a conservative treatment whenever allowed by a stable clinical condition and the availability of appropriate clinical and radiological monitoring.
Introduction
Post-traumatic injuries of the duodenum are rare due to its retroperitoneal location. However, they pose a diagnostic problem particularly because of the non-specificity of the clinical presentation. The treatment of duodenal injuries has long been exclusively surgical. Non-operative conservative treatment has recently been described.
Patients and Outcomes
A review of pediatric surgical emergency registers identified 6 cases (Table 1) of duodenal injury following abdominal blunt trauma. The study period was from 2009 to 2022.
Summary of Patients Treated for Duodenal Post-Traumatic Injury in the Pediatric Emergency Department Between 2009 and 2022.

The patients’ age ranged from 5 to 15 years with an average of 9 years. Three girls and 3 boys were treated; there was no gender predominance. Domestic accidents were the most common mechanism of injury, represented in 5 cases, followed by road accidents; 1 case.
In the majority of cases (5 cases), the time to consultation exceeded 24 hours. Abdominal pain was a constant symptom in all 6 patients, 2 patients had bilious vomiting.
Ultrasound allowed diagnosis in 2 patients (Figure 1). It revealed a duodenal hematoma in one patient and an abdominal effusion in favor of a digestive perforation in the second case.
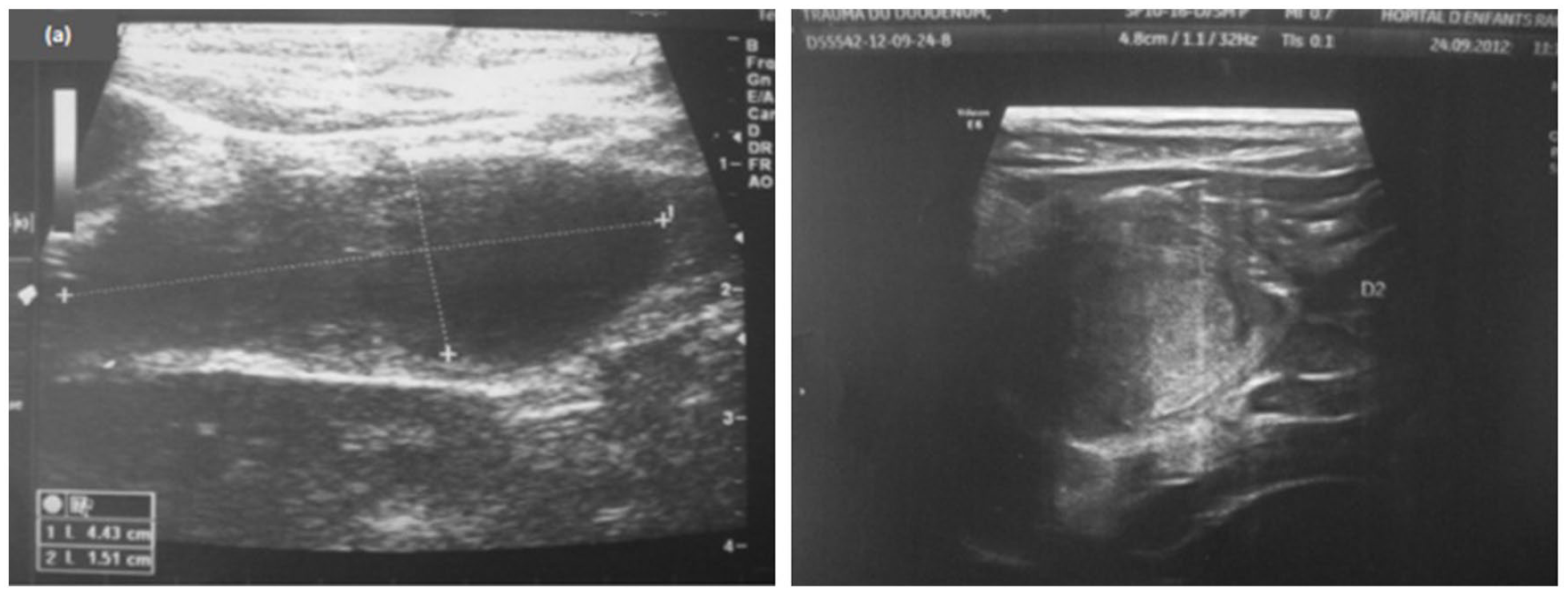
Ultrasound revealing a duodenal mass suggestive of intramural duodenal hematoma.
Abdominal/Pelvic CT scan was the most sensitive examination and confirmed the diagnosis in 4 patients; 2 cases of isolated duodenal hematoma (Figure 2), 1 case of duodenal hematoma with retroperitoneal air bubbles (Figure 3), 1 case of parietal duodenal hematoma and duodenal defect of approximately 11 mm with pneumo-peritoneum (Figure 4).

CT scan imaging showing isolated duodenal hematomas in 2 children.

CT scan imaging showing a duodenal hematoma with retroperitoneal air bubbles.

CT scan imaging showing a parietal duodenal hematoma and duodenal defect of approximately 11 mm with pneumo-peritoneum.
CT scan was also used to search for associated lesions, which were found in 3 patients. Two patients had pancreatic lesions and one patient had right kidney laceration.
Two patients were treated surgically. The first patient presented with abdominal tenderness with impure fluid effusion on ultrasound and was admitted for suspicious digestive perforation. Surgical exploration found a perforation of about 3 cm of the posterior face of D2 with biliary effusion. The surgical procedure consisted of a primary repair of the duodenum.
The second patient had a duodenal rupture on CT scan with extensive parietal duodenal hematoma and homogeneous swelling of the pancreas. The patient was admitted to the OR where a perforation of 75% of the diameter of D2 was found. The procedure consisted of a 2-layer closure of the duodenal perforation with gastrojejunostomy and pyloric exclusion. These procedures were combined with external drainage of the gallbladder by a Foley probe at the vesicular fundus. On the 15th postoperative day, the cholecystostomy tube was removed. The child was discharged home after a hospital stay of 18 days.
The other patients received a conservative non-operative treatment based on resting the digestive tract by placing a nasogastric tube and parenteral nutrition with close clinical, radiological and biological monitoring. Radiological follow-up was carried out by abdominal ultrasound in 2 cases, showing liquefaction of the hematoma. For the other 2 cases, CT scan showed regression of the hematoma in one case and a reduction in the retroperitoneal bullae with the absence of extravasation of the contrast enema in the second case. Length of hospitalization for these patients varied between 9 and 30 days.
Ethical Approval and Informed Consent
Ethical approval was not required for the report of this case series.
Written informed consent was obtained from the patients and their parents for the publication of this case series.
Discussion
The anatomy of the duodenum is unique and complex because of its different relationships. Located deep in the abdomen, the duodenum is well protected in the retroperitoneal space. Therefore, duodenal lesions are rare and are often associated with vascular, hepatic, pancreatic and biliary lesions, making the clinical presentation non-specific and the pre-operative diagnosis very difficult. The diagnosis can therefore go unnoticed in 18.75% of cases. 1
In the case of abdominal contusion, the risk of duodenal injury is greater in children than in adults, mainly because of the lesser amount of intra-abdominal fat and the absence of protection by the more horizontal rib cage. In children, duodenal hematomas are more frequent.
Several injury mechanisms have been incriminated in the pathogenesis of duodenal-pancreatic trauma. First, crushing of the duodenum on the spine in a sustained trauma. Secondly, tearing by deceleration movement leading to vascular lesions at the level of the muscular and sub-serosal layers with the formation of intramural hematomas. Last, bursting of the duodenal frame either by sudden irruption of the gastric contents into the duodenum or by sudden increase in intraluminal pressure.
Patients presenting with duodenal injuries have most often been victims of everyday accidents or road traffic accidents. Depending on the context, the possibility of abuse should be considered. 1
Once the patients have been explored by radiological examinations or surgically, the duodenal lesions can be classified according to the Duodenal Organ Injury Scale of the American Association for the Surgery of Trauma (Table 2).
Duodenal Organ Injury Scale: American Association for the Surgery of Trauma. 2

In the acute phase, a precise diagnosis is very difficult because of the anatomical situation of the duodenum and the non-specific and often misleading symptomatology.
Various additional tests may be requested. Biologically, a blood count shows a drop in hemoglobin and hyperleukocytosis, which is almost always present due to a demargination phenomenon. Pancreatic enzymes, if elevated, can point to an associated pancreatic lesion.
On imaging, plain abdominal X-ray can be requested to show indirect signs of duodenal injury: a pneumoperitoneum or a pneumo-retroperitoneum. In the case of a parietal hematoma, the X-ray may reveal gastric dilatation or hydro-air levels in the duodenum.
Ultrasound may reveal a duodenal mass suggestive of intramural duodenal hematoma or an impure peritoneal effusion which would suggest a perforation.
In case of suspicion of a duodenal lesion, CT is the first line examination which can reveal a pneumoperitoneum or a leak of contrast enema often associated with an effusion and evoking an intraperitoneal duodenal rupture. In case of duodenal hematoma, it would allow its direct visualization in the form of parietal thickening with duodenal obstruction.
Concerning duodenal hematomas, the various series reported3,4 conclude that the conservative non-operative treatment is to be considered in the first instance. It consists of fasting which allows resting of the digestive system, nasogastric or nasoduodenal tube for decompression, antibiotics and parenteral nutrition. All accompanied with rigorous clinical, biological and radiological monitoring. In the absence of improvement or in case of aggravation, percutaneous drainage5-7 or surgical exploration may be indicated. Surgery may be performed immediately in cases of hemodynamic instability or associated lesions.
Duodenal perforations and ruptures have long been treated exclusively by surgery, and are associated with a high morbidity and mortality rate. This is mainly due to intraoperative difficulties and the risk of duodenal fistula; the most frequent complication (10%). The latero-lateral gastro-jejunal anastomosis with pyloric exclusion described by Vaughan et al 8 has reduced the incidence of fistula to less than 5%. This is the recommended technique for severe duodenal injuries. 9
Only a few cases of duodenal perforations in adult and pediatric patients 10 have been reported in the literature. The number of cases does not allow us to draw reproducible conclusions. In our experience and after studying the cases in the literature, if the perforation is localized to the retroperitoneum in a hemodynamically stable patient, non-operative conservative treatment can be considered. Antibiotic coverage and rigorous clinical and paraclinical monitoring are nevertheless mandatory.
Conclusion
Although conservative non-operative treatment has become the first line management for duodenal hematomas, most duodenal perforations are still dealt with surgically. The small number of reported cases doesn’t allow a clear establishment of its indications. A multi-centric study remains mandatory.
Footnotes
Author Contributions
All authors contributed to the writing of this manuscript, all read and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The patients and their parents written approval was obtained for publication of this article.