
Abstract
Polysplenia syndrome is an uncommon condition associating several splenic nodules (sometimes polylobed spleen and cases of normal spleen have been described) with a number of malformations that appear between the fourth and sixth week of embryonic development. Although it has been suggested that genetic, teratogenic, and embryogenic factors may be at fault, the exact etiology remains unclear. Clinically, it is generally asymptomatic or mildly symptomatic. The authors report the case of an 11-months-old infant from a poorly monitored pregnancy. He was admitted to the emergency room for respiratory discomfort in a context of apyrexia. A thoraco-abdominal CT scanner revealed a polysplenia syndrome.
Case Report
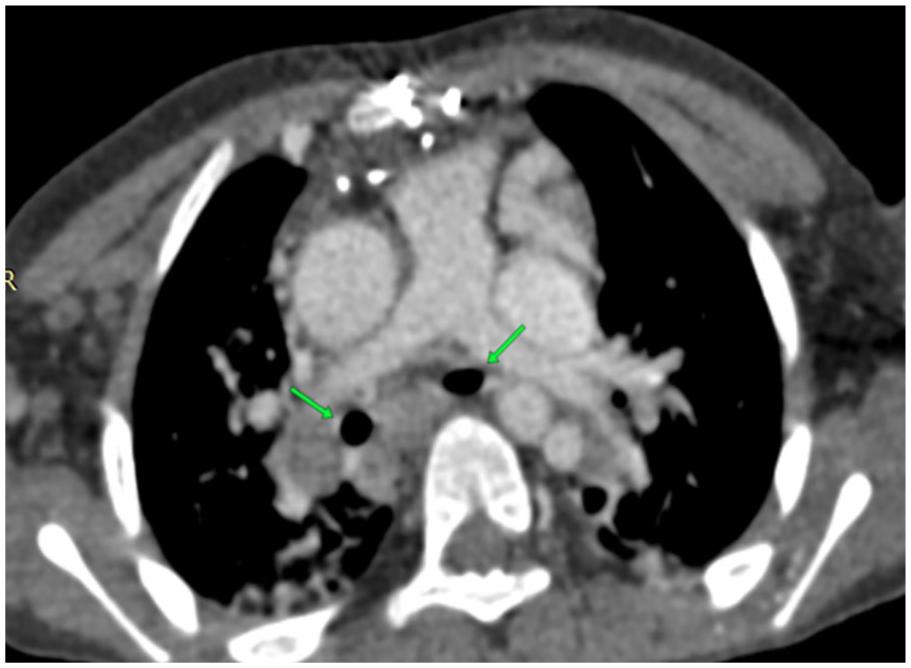
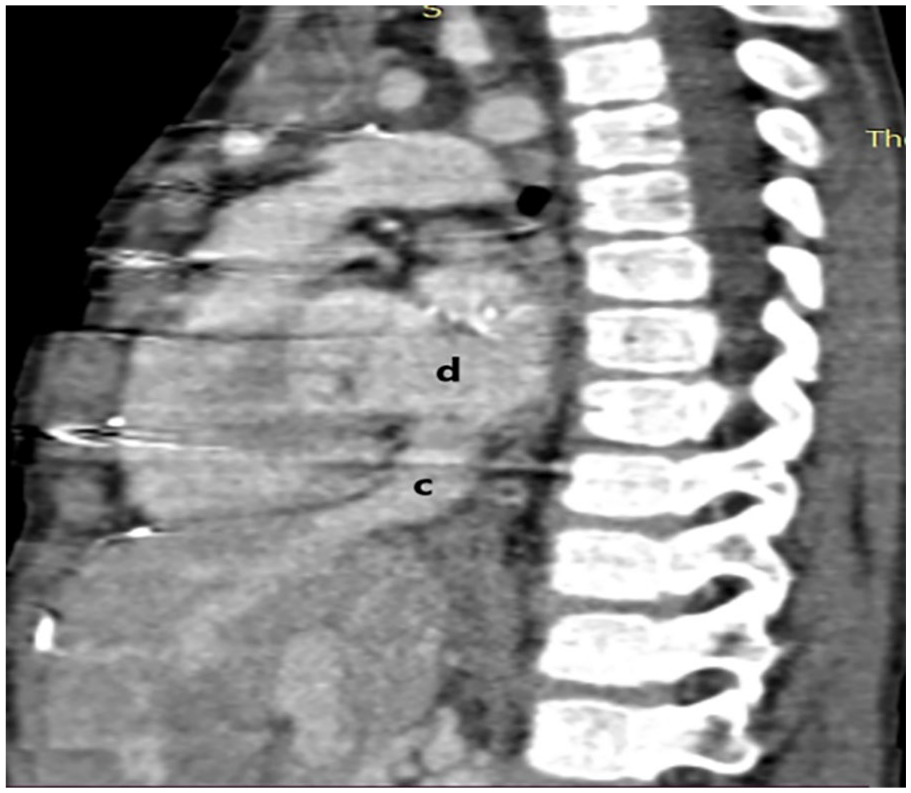
An 11-month-old boy, from a poorly monitored pregnancy, got operated on for a common atrioventricular canal. After a 6 months, he was brought to the emergency room with respiratory discomfort, no fever and no other history according to the mother and the referring physician. At admission, the infant was conscious and responsive but hypotonic, with an oxygen saturation level of 89%. The patient was started on oxygen therapy and a chest radiograph was performed. It showed some alveolar opacities of both lung fields, which prompted us to realize a thoraco-abdominal CT scan. On the mediastinal window, we discovered an situs ambiguous with a mesocardia, a medial liver, a spleen replaced by several right splenic nodules and a right stomach (Figure 1); with left isomerism: both atria were of left morphology and a hyparterial bronchi (Figure 2). In addition to that, we found associated anomalies of venous return such as the azygos continuation of the inferior vena cava, which was agenesic in its retro-hepatic part, with hepatic veins flowing directly into the patient’s right atrium (Figures 3 and 4). Moreover, the superior vena cava was located on the left (Figure 5) receiving both the azygos vein (Figures 6 and 7) and the innominate trunk on the left. While the ascending and descending aortas were in place (Figure 5). Furthermore, no abnormalities of the pulmonary arteries or the common mesentery were noted. On the parenchymal window, both lungs were bilobed with mosaic perfusion pattern of the two lung fields (Figure 8).

11-month-old male infant with polysplenia syndrome.
11-month-old male infant with polysplenia syndrome operated for common atrioventricular canal.

11-month-old male infant with polysplenia syndrome operated for commonatrioventricular canal.
11-month-old male infant with polysplenia syndrome operated for common atrioventricular canal.

11-month-old male infant with polysplenia syndrome operated for common atrioventricular canal.

11-month-old male infant with polysplenia syndrome operated for common atrioventricular canal.

11-month-old male infant with polysplenia syndrome operated for common atrioventricular canal.

11-month-old male infant with polysplenia syndrome operated for common atrioventricular canal.
Discussion
Heterotaxy syndrome 1 is an anomaly of distribution of thoracic and abdominal organs. In this entity, the usual left-right distribution of these organs (situs solitus) does not correspond entirely to a situs inversus (complete mirror image). It is thus called situs ambigus.
Polysplenia syndrome 2 is a rare form of heterotaxy syndrome. Also known as left isomerism, it is characterized by a number of spleens greater than or equal to two with identical volume, and a lateralization anomaly in the form of situs ambigus; although situs inversus might exceptionally be encountered. Some forms of polysplenia syndromes can have a single normal or polylobed splenic gland. Moreover, considering the embryology of the splenic tissue that develops in the posterior mesogastrium, the spleen and or the splenic nodules are always located on the same side of the stomach along the greater curvature.
Other anomalies include an agenesis of the supra-renal IVC with a continuous azygos system and a direct drainage of the hepatic veins into the right atrium. Some authors also described associations with other cardiac, pulmonary, vascular and digestive malformations. 2
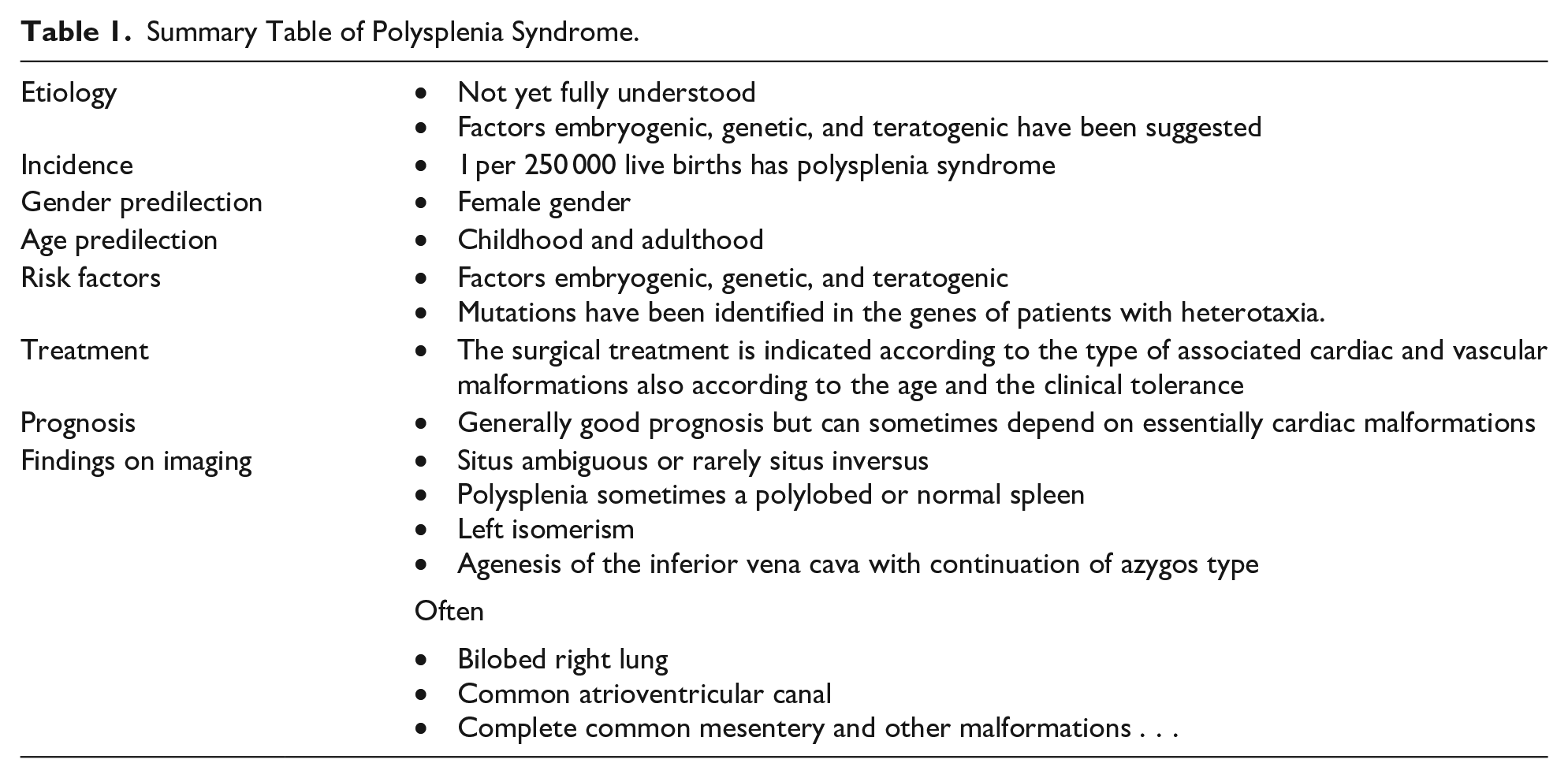
Etiology and Demographics (Table 1)
It is predominant in females with an estimated incidence of 1 per 250 000 live births. And it can be diagnosed during adulthood as well as childhood. 3
Summary Table of Polysplenia Syndrome.
Peoples et al 4 described the first case of polysplenic syndrome in 1781. After performing a series of 146 autopsies, they assessed the prevalence of the most frequently found abnormalities. 58% of patients had bilateral bilobed lungs with left-type bronchial segmentation, 47% had bilateral superior vena cava, more than 60% had cardiac abnormalities, and 56% had gastrointestinal positional abnormalities.
Although no clear etiology has been identified yet, some clues tend toward embryogenic, genetic and teratogenic causes. 5 Furthermore, mutations have been identified in the genes of patients with heterotaxia.
Clinical and Imaging Findings (Table 1)
The malformations generally found in polysplenia syndrome appear between the fourth and sixth week of embryonic life 2 :
Cardiovascular anomalies are represented by a defect of the inter-ventricular or inter-auricular septum, a common atrioventricular canal, a double outlet of the left ventricle, a common atrium, interposition of the portal vein in preduodenal, transposition of the large vessels, sometimes a double superior vena cava and rarely persistence of the left superior vena cava without individualization of the right inferior vena cava (which was the case in our patient). 2
Digestive anomalies include a complete common mesentery, an annular pancreas, a microcolon, gallbladder agenesis (50%) and/or biliary atresia, which in some cases requires a liver transplant.
Most pulmonary anomalies consist of bilateral bilobed lungs with a left type segmentation since it is a left isomerism malformation. Trilobed lungs, having a right type segmentation, are generally associated with asplenia, another kind of heterotaxy syndrome. This asplenia syndrome or Ivemark syndrome is characterized by a right isomerism and is a differential diagnosis of the polysplenia syndrome.
Thanks to the viable cardiac malformations, polysplenia syndrome can remain asymptomatic and diagnosis is usually fortuitous in adulthood. Whereas in asplenia syndrome, these cardiac malformations are lethal. 6
Prenatal ultrasound can help in prenatal diagnosis, revealing essentially lateralization anomalies.
Imaging techniques, including thoraco-abdominal CT scan with contrast, are essential for the minutiose assessment of the malformations as well as for the preoperative strategy.
Treatment and Prognosis (Table 1)
Surgical treatment is adapted to the type of cardiac and vascular malformations and to age and clinical tolerance.
In case of atrioventricular canal; as the case was for of our patient; surgical management will be adjusted to the age (2 and 6 months) as well as to the valvular leaks and the pulmonary vascular resistances).
Prognosis depends on the morbidity and mortality of the associated malformations, especially congenital heart disease. As a matter of fact, prognosis of these cardiopathies is generally good thus the overall favorable outcome seen in polysplenia syndrome patients unlike asplenia syndrome.
Differential Diagnoses (Table 2)
Asplenia syndrome is a type of heterotaxy syndrome (situs ambiguous) which is characterized by asplenia, right isomerism, trilobate left lung, superior vena cava duplication, complex congenital heart disease, and gastro-intestinal anomalies.
Differential Diagnosis Table for Polysplenia Syndrome.
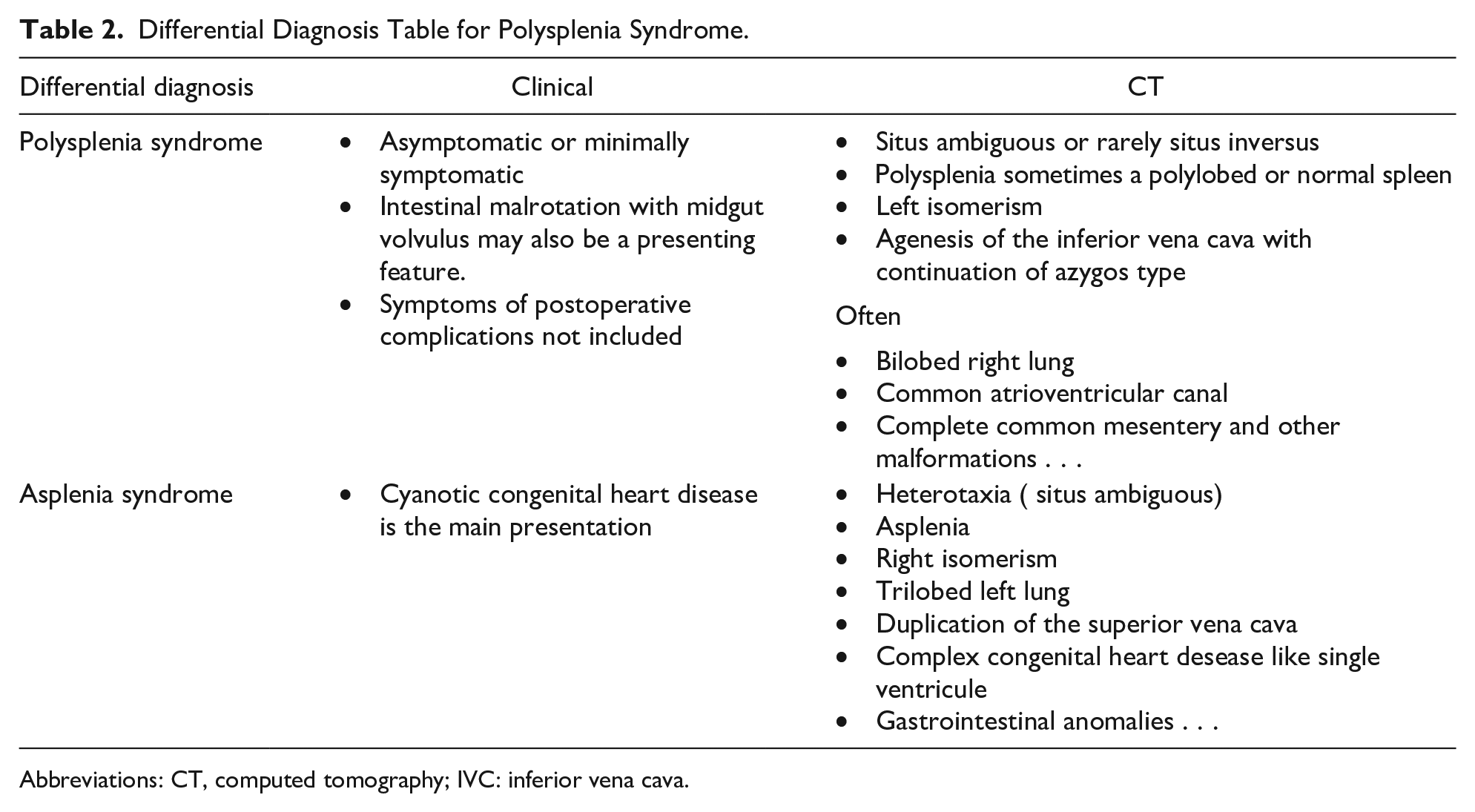
Abbreviations: CT, computed tomography; IVC: inferior vena cava.
Conclusion
Polysplenia syndrome is a rare polymalformative condition associating vascular, cardiac, pulmonary, and visceral malformations. CT imaging is a must in the minutiose assessment of the malformations spectrum, thus making it easier to make an accurate prognosis and eventually plan for surgical management when necessary.
Teaching Point
The importance of this article lies in presenting and describing a unique form of heterotaxy syndrome: polysplenia syndrome with an unusual left inferior vena cava. As well as showing the importance of imaging in the diagnosis and the evaluation of associated malformations for a clearer prognosis, a more precise preoperative workup and early surgical treatment of the cardio-vascular abnormalities.
Footnotes
Authors Contributions
El Houss Salma: Preparation and creation of the published work. Amsiguine Najwa: Preparation and creation of the published work. Tantaoui Mehdi: Preparation and creation of the published work. Chat Latifa: Supervising published work. Allali Nazik: Supervising published work. El Haddad Siham: Supervising published work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
The authors declare that they have no relationship of interest.
Consent
No identifying information was disclosed in the article.
Human and Animal Rights
No human or animal experimentation has been included in the article.