
Abstract
Sleep-related health problems are under investigated among adolescents in low-income countries, including our country, Ethiopia. Therefore, this study aimed to assess the sleep quality and its associated factors among adolescents aged 10 to 19 years in Ethiopia. A community-based cross-sectional study was conducted among 799 adolescents from May 27 to July 27, 2021, using a systematic random sampling technique. Sleep quality was assessed by using the Petersburg sleep quality index. The data was entered into Epi-data version 3.1 and exported to the Statistical Package for Social Science (SPSS) Version 21. A logistic regression model was used, and variables with a P-value less than .05 in the final fitting model were stated as independent predictors of poor sleep quality (PSQ). About 1 in 3 adolescents (38%) had a poor sleep quality. The rates of inhalant, khat, and internet use disorders were 16%, 38%, and 18%, respectively. Also, 27.4% of adolescents used alcohol as a sleep medication, and 75% of adolescents with internet addiction had PSQ. Moreover, adolescents with physical illness had about 4 times higher odds of association with PSQ (AOR = 3.76 and 95% CI = 2.30-6.15%CI), and inhalant use disorder (AOR = 1.98 and 95% CI = 1.29-3.04%CI), internet addiction (AOR = 3.33 and 95% CI = 2.09-5.30%CI), and khat use disorder (AOR = 1.74 and 95% CI = 1.11-2.73%CI), were positively associated with PSQ. PSQ was higher among adolescents, and problematic inhalants, khat, and internet use and physical illness were risk factors for PSQ.
Background
Sleep is an indispensable part of life that plays a major role in health and growth. 1 Major physiological functions and brain activities occur during sleep. 1 Sleep is one of the major contributing factors to the physical and mental health well-being of adolescents. Sleep is critical to somatic, cognitive, and psychological processes. 2 Sleep patterns vary throughout life 3 and influenced by a variety of internal and external factors.4-7
Sleep deprivation is defined as not getting enough sleep on a regular basis.8,9 Suboptimal sleep quality is associated with a wide range of adverse health outcomes; such as conduct problems, inattention, depression, anxiety, drug and alcohol use, decreased academic performance, and suicidal behaviors.9,10 Sleep efficiency, bedtime, daytime dysfunction, waking time, and sleep duration are all examples of sleep habits. 11 Numerous studies have found that sleep disorders have a negative impact on adolescent mental health, including decreased work efficiency and learning ability, being inattentive, distracted, uninterested, impulsive, and hyperactive.12-16 Chronic sleep disorders have been linked to major depression, anxiety, and substance use disorders.17,18 Furthermore, sleep quality was associated with age, gender, residence, body mass index, physical activity, or sports. 19 Chronic physical illness, 20 nicotine, alcohol, and caffeine use disorders, sedentary lifestyle, malnutrition, and skipping breakfast are associated with poor sleep quality among adolescents. Short-term effects of sleep disorders among adolescents include daytime sleepiness and fatigue during the day.9,10
Adolescents use the internet for many reasons, such as; social networking, communicating, playing music, emailing, and playing games. 21 Having internet availability with devices such as mobile phones and tablets provides adolescents access to use the internet during the day and bed time. Adolescents are at risk of internet addiction due to the availability of such facilities.22-24 Excessive internet use (addiction) is also associated with poor sleep quality and sleep disturbances.12,25-28 It has been reported that adolescents who use the internet go to bed later in the night, take more time to fall asleep, and experience an increased number of awakenings during the night. 29 About 16% to 24% of adolescents in Asia who use the internet excessively have poor sleep quality, which leads to depressive symptoms.30,31
A meta-analysis study of the sleep patterns of adolescents found that about 45% of adolescents in grades 6 to 12 had insufficient sleep quality. 32 Poor sleep quality is prevalent in studies conducted in Europe, the United States, and Japan, with prevalence ranging from 20% to 48%. 33 Poor sleep quality is a common problem among adolescents, and both biological and social factors contribute to poor sleep quality. 34 Poor sleep quality among adolescents needs great attention since adolescents are going through rapid physical, mental, and emotional changes during this age. 33 Given the heavy burden of poor sleep quality among adolescents, identifying factors for the prevention and management of sleep-related behavioral and physical health problems is a crucial strategy. Although many studies have been investigated among high school and university students,2,8,15,19 little is known regarding sleep quality and factors predicting poor sleep quality among adolescents aged 10 to 19 years in low-income countries, including our own country, Ethiopia, and Africa. Up to date, the prevalence of sleep quality and the relationship between sleep quality, and substance use disorders (khat, cannabis, inhalants, alcohol, nicotine, and caffeine), internet addiction, physical activity, conduct disorder, and chronic physical illness among adolescents aged 10 to 19 years has not been investigated in our country, Ethiopia. Moreover, the previous studies conducted among high school and university students were only institution-based which lacks collateral information from parents and guardians for sensitive issues like substance use, and excludes adolescents who were not in the school. Therefore, this study assessed poor sleep quality and associated factors among adolescents in Bonga, Mizan-Aman, and Tepi towns in southwest Ethiopia.
Methods
Study Setting and Period
The study was carried out in Mizan-Aman, Bonga, and Tepi towns among adolescents aged 10 to 19 years from May 27 to July 27, 2021. Mizan-Aman town is located in Bench Sheko zone, 561 km away from Addis Ababa, which is the capital city of Ethiopia. Bonga town is located in the Kafa zone, 460 km away from Addis Ababa, while Tepi town is located in the Masha zone, 611 km southwest of Addis Ababa. Mizan Aman town has 2 health centers and 1 teaching hospital, while there is 1 health center and 1 general hospital for both Bonga and Tepi towns.
Study Design and Population
A cross-sectional investigation was carried out. All adolescents who are living in towns in Ethiopia were the source population, while adolescents who met the eligibility criteria at the data collection time were the study population. Adolescents who were available during the study period were included, but those with communication impairment and those who were unable to respond due to psychiatric or physical illness were excluded.
Sample Size Determination and Sampling Techniques
The sample size was determined using the single population proportion formula, assuming a prevalence (p) of 50% since no similar study was carried out in our country among adolescents aged 10 to 19 years. Using a 95% confidence interval and a margin of error (d = .05) and a non-response rate of 10%. The total sample size was 845. A systematic random sampling technique was used. The 3 towns; Mizan-Aman, Bonga, and Tepi, were purposely selected because of their large population sizes. About 30% of each town’s kebele were chosen. Based on the total number of households in each kebele, the sample size was allocated proportionally. A list of respondents’ households was obtained from health extension workers. After obtaining a list of participant households, every Kth household was recruited by labeling each household that had adolescents aged 10 to 19 years, and the initial household was selected by a lottery method. A lottery method was also used if there was more than one eligible adolescent in a household.
Procedure
Pretested semi-structured questionnaire with socio-demographic, environmental, clinical, and substance-related variables were used to collect data. The Pittsburgh Sleep Quality Index (PSQI) was used to measure the sleep quality among adolescents. The Pittsburgh Sleep Quality Index is an instrument used to assess the quality and patterns of sleep in adolescents. It measures 7 components to differentiate “poor quality of sleep from good” by assessing the following dimensions: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medications, and daytime dysfunction over the last month. All components received a score based on a Likert scale of 0 to 3, where a score of 0 reflected the positive extreme (“not during the past month”) and a score of 3 reflected the negative extreme. A global PSQI score of >5 was indicative of poor sleep quality. 35 The reliability (Cronbach’s alpha) in this study was .83.
Substance (alcohol, khat, nicotine, cannabis, inhalant, and caffeine) use patterns were assessed using the DSM V criteria of substance use disorder, which included the following components: the amount of specific substance use for at least a year; the desire to cut down or many unsuccessful attempts to cut down or stop; spending a significant amount of time while using or obtaining a substance; the strong desire to use the substance; continuing substance use despite persistent social problems; preferring substance use over family, occupational, and recreational activities; using a substance in situations where it is physically hazardous (while driving, manipulating a machine, etc.); using a substance despite knowing that it has psychological and/or physical health problems; increasing the dose of the substance to achieve the desired effect or reduced efficacy when the usual amount is used; and experiencing psychological or physiological symptoms if the dose is decreased or stopped at all. In order to score a substance use disorder, adolescents must score 2 out of the 11 criteria for at least a year. Adolescents with mild, moderate, or severe substance use disorders must fulfill 2 to 3, 4 to 5, and 6 or more from the 11 criteria, respectively. 36
Internet addiction was assessed by using an internet addiction test. The internet addiction test contains 18 items that can be scored on a three-point Likert scale (never, sometimes, and often).The scoring ranges from 0 to 36. A score of 0 to 14 indicates no addiction, a score of 15 to 19 indicates borderline internet addiction, a score of 20 to 29 indicates possible internet addiction, and a score of greater than 30 indicates probable internet addiction. 37 Conduct disorder was assessed by using DSM 5 diagnostic criteria for conduct disorder. Adolescents were said to have conduct disorder if they scored 3 or more of the 13 symptoms of childhood conduct disorder. 36 The standardized Oslo-3 social support scale was used to assess the social support status of the adolescents. Social support status was measured as the following: poor support 3 to 8, moderate support 9 to 11, and strong support 12 to 14. 38
In addition, socio-economic and demographic variables (sex, age, family occupational status, family marital status, family educational status, religion, ethnicity, family income, death of parents, school misconduct, absence from school, ever being a street child, having a boy or girl friend), academic performance, physical exercise, and having physical illness were assessed.
Data collectors were clinicians with bachelor’s degrees in clinical psychiatry. A senior clinical mental health specialist provided training on tools for data collectors and supervisors to ensure data quality. A standard was checked for scoring individual items of the questioner before data collection. In addition, data were gathered using a structured, locally translated Amharic version of the questionnaire. The pretest was carried out with 5% of the required sample size in a Shako town to minimize errors in the data collection instruments. Finally, the data collection took place in private place for adolescents, and the collateral information was collected from their parents or guardians.
Data Analysis
Before being exported to SPSS version 21 software for analysis, data were coded, edited, cleaned, and entered into epidata version 3.1. Descriptive statistics like frequency and percentage were calculated. Logistic regression was used; both bi-variate and multivariate logistic regressions were used to identify the independent factors for poor quality of sleep, and crude and adjusted odds ratios were computed for each variable to determine the strength of association. The candidate variable with a P-value less than .25 on bi-variate analysis was entered into multivariate logistic regression to control the con-founder after checking the multicollinearity. Independent factors were declared at a P-value <.05 cut-off point, and the strength of association was evaluated using AOR with their corresponding CI at 95%. A (P < .05) on the multivariate logistic regression model was considered statistically significant.
Results
Socio-Demographic and Economic Characteristics
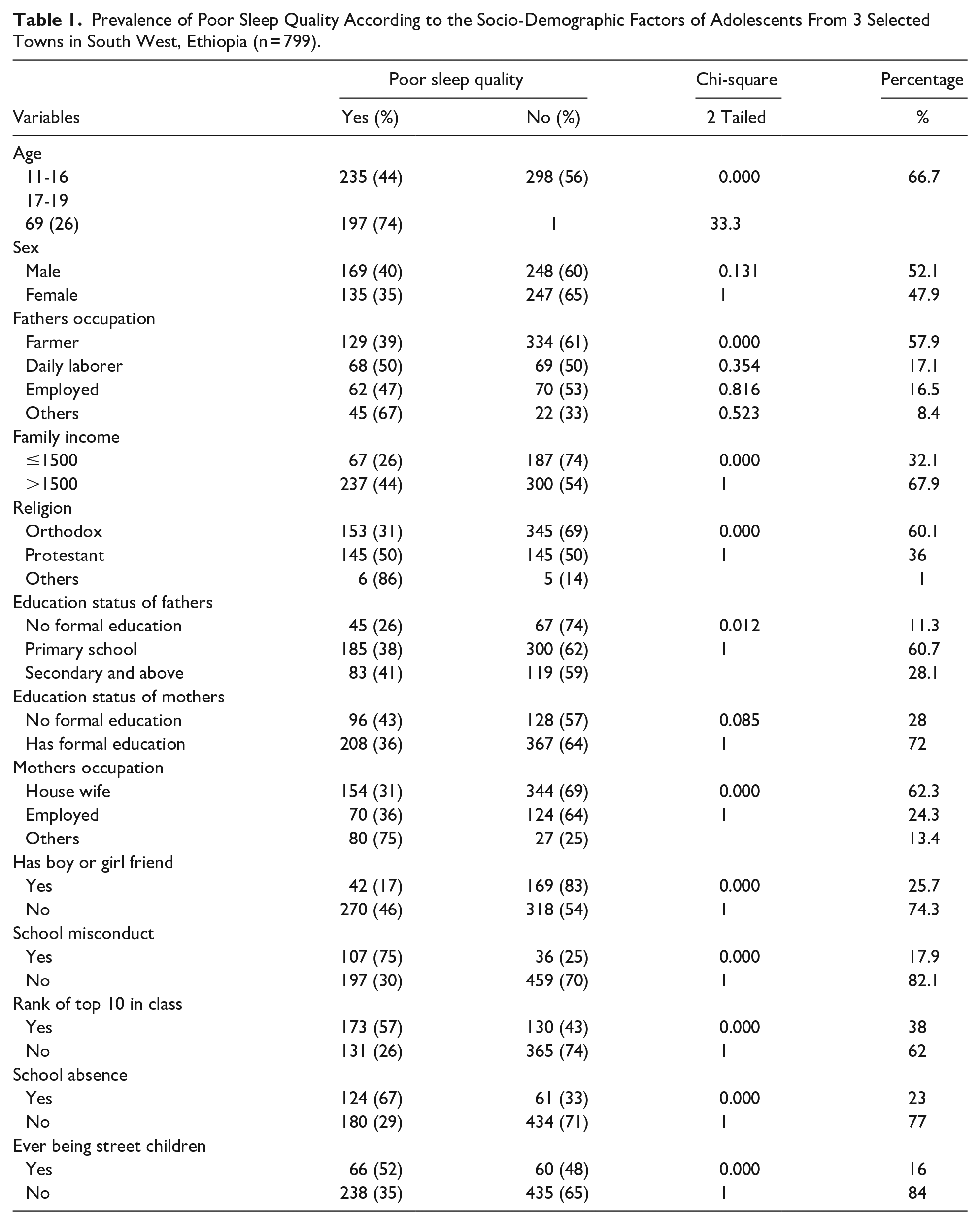
Of the total of 845 participants required to participate, only 799 adolescents participated, whose response rate was 94.6%. The mean and standard deviation of the participants’ ages in a year was 15.33 and 2.51, respectively. The females and males were almost equal, and the most common religion in this study was orthodox. Socio-demographic information is provided below in Table 1.
Prevalence of Poor Sleep Quality According to the Socio-Demographic Factors of Adolescents From 3 Selected Towns in South West, Ethiopia (n = 799).
The Prevalence of Sleep Quality and the Relationship Between Determinant Variables of Sleep Quality According to Specific Components of the PSQI Score
A total of 304 (38%) of the adolescents had poor sleep quality, and the prevalence of daytime dysfunction, bad subjective sleep quality, sleep disturbance, and short sleep duration was 77.2%, 14.3%, 16.3%, and 20.4%, respectively, among adolescents. Moreover, about 3 in 4 adolescents with khat use disorder had poor subjective sleep quality and slept later than adolescents without khat use disorder. Again, more than 1 in 3 adolescents with khat use disorder reported that they had disturbed sleep and daytime dysfunction compared to those with no khat use disorder. Almost all adolescents and more than 1 in 3 adolescents with internet addiction reported that they had sleep latency and poor subjective sleep quality, respectively. Nearly half and more than 1 in 5 adolescents with physical illness reported that they had poor sleep quality and took sleep medication, respectively (see Table 2).
Prevalence of Khat Use Disorder, Internet Addiction, and Epilepsy According to Specific Components of PSQI of Adolescents From 3 Selected Towns in South West, Ethiopia (n = 799).

Abbreviations: KUD, khat use disorder; IA, internet addiction; PSQI, Petersburg sleep quality index.
The Relationship Between Sleep Quality and Specific Substance Use Disorders
Of the total participants, 117 (15%), 89 (11%), and 98 (12%) had mild, moderate, and severe khat use disorders, respectively. A total of 437 (54.6%) of the adolescents had an alcohol use disorder, and among them, nearly all (85%) had good sleep quality. Of the total participants, 270 (33.8%), 89 (11%), and 98 (10) had mild, moderate, and severe alcohol use disorders, respectively. A total of 91 (11%) of the adolescents had cannabis use disorders, and among them, 41 (5%), 33 (4%), and 16 (2%) had mild, moderate, and severe cannabis use disorders, respectively. Moreover, a total of 129 (16%) of the adolescents had an inhalant use disorder, and among them, about one-fourth (26%) had poor sleep quality. Of the total participants, 43 (5%), 58 (7%), and 28 (4%) had mild, moderate, and severe inhalant use disorders, respectively. Furthermore, a total of 140 (17%) of the adolescents had a nicotine use disorder, and among them, more than one-fourth (28%) had poor sleep quality. Of the total participants, 49 (6%), 50 (6%), and 41 (5%) had mild, moderate, and severe nicotine use disorders, respectively. Of the total participants, 143 (18%) had an internet addiction, and among them, 108 (75%) had poor sleep quality (see Table 3).
Prevalence of Poor Sleep Quality According to the Specific Substance Use Disorder of Adolescents From 3 Selected Towns in South West, Ethiopia (n = 799).

The Relationship Between Poor Sleep Quality, and Clinical and Social-Related Variables
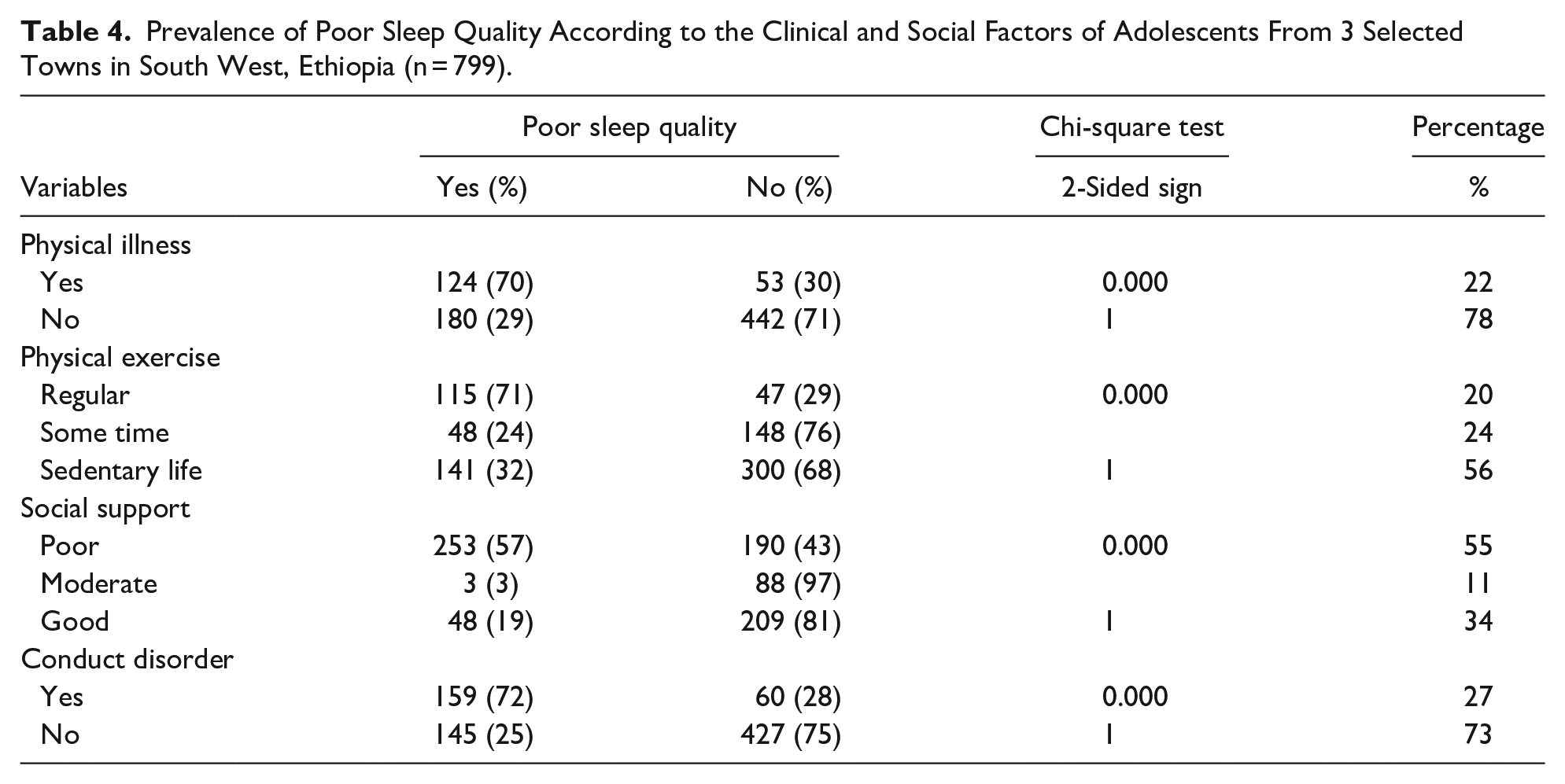
Almost one-fifth of the total participants, 177 (22%), had a physical illness, with almost half (49%) having a seizure disorder; among them, 124 (70%) had poor sleep quality. More than half of the adolescents had sedentary lifestyles, and among them, 141 (32%) had poor sleep quality, and only 162 (20%) of the respondents practiced regular physical exercise. Among the respondents, 443 (55%) had poor social support, and among them, more than half (57%) had poor sleep quality. Furthermore, nearly one-third (27%) of the adolescents were screened positive for having conduct disorders, and among them, the majority (72%) had poor sleep quality (Table 4).
Prevalence of Poor Sleep Quality According to the Clinical and Social Factors of Adolescents From 3 Selected Towns in South West, Ethiopia (n = 799).
Factors Associated With Poor Sleep Quality Among Adolescents
According to the bivariate analysis, being in the top 10 of the class, having misbehavior in school, multiple absences from school, having khat, alcohol, nicotine, cannabis, and inhalant use disorders, having conduct disorder, internet addiction, a history of physical illness and seizure disorder, being a street child, and having poor social support were all associated with poor sleep quality. However, multivariate logistic regression showed the following variables; having any seizure or other medical illness (AOR = 3.76 and 95% CI = 2.30-6.15%CI), inhalant use disorder (AOR = 1.98 and 95% CI = 1.29-3.04%CI), internet addiction (AOR = 3.33 and 95% CI = 2.09-5.30%CI), and khat use disorder (AOR = 1.74 and 95% CI = 1.11-2.73%CI) were positively associated with poor sleep quality among adolescents in this study (See Table 5).
Poor Sleep Quality and Associated Factors in Both Bi-Variate and Multivariate Logistic Regression Analysis of Adolescents From 3 Selected Towns in South West, Ethiopia (n = 799) of the Sampled (N = 799) Adolescents in Bonga, Mizan Aman, and Tepi Town, South West, Ethiopia, 2021.

Abbreviations: 1, reference category; COR, crude odds ratio; AOR, adjusted odds ratio.
Discussion
This study assessed the sleep quality and associated factors among adolescents in Bonga, Mizan-Aman, and Tepi towns in the southwest of Ethiopia. This study disclosed that the prevalence of poor sleep quality was 38%. In addition, more than half (57.4%) of the adolescents had short sleep duration, and the majority (77.2%) of the adolescents reported that they had daytime dysfunction. Moreover, one-fourth (27.4%) of adolescents used alcohol as a sleep medication, and only 25 (3.1%) of adolescents used other prescribed medications as sleep medications. In addition, internet addiction, having a chronic physical illness, inhalant use disorder, and khat use disorder were positively associated with poor sleep quality among adolescents in Ethiopia.
The prevalence of poor sleep quality in this study was almost comparable with the studies done among adolescents in China, India, and Thailand.39-41 However, the current finding was lower than the studies done among adolescents in Thailand and Nepal,8,30 and higher than another study conducted among adolescents in Malaysia. 42 The possible explanation for the difference could be the difference in study setting, sample size, culture, study design, and age difference. The current study was more inclusive among adolescents from age 10 to 19 years while other studies assessed sleep quality among undergraduate students and high school students.
Khat use disorder was one of the factors significantly associated with poor sleep quality in this study, and adolescents with khat use disorder had about 2 times the odds of association with poor sleep quality than their counterparts. This finding was the same as the study conducted in Jimma, Ethiopia, and Yemen.43,44The reason could be due to the sympathomimetic effects of khat that have an amphetamine like effect which cause psycho-stimulation and euphorigenic effects by impairing the sleep center.44,45
The association of khat use disorder with poor sleep quality could also be explained by the culture of problematic khat use among adolescents in Ethiopia. Adolescents chew khat to manage their distress and excessive work load and they chew khat during prayer, mourning, and wedding ceremonies to induce alertness, energy, concentration, feeling free, and to avoid hunger during the daytime. Individuals who chewed khat during the day had difficulty sleeping at night. As a result, they use locally available alcohol content (tella, teji, arake, beer, and borde) to self-medicate themselves regarding the simulative effect of khat to have a good sleeping pattern at night. Furthermore, they also use khat in the early morning as an eye-opener, culturally called “jebena.” According to this study, about one-fourth of adolescents (27.4%) used alcohol as a sleep medication after chewing khat to manage their sleep problems at night. This finding supports the cultural phenomenon called “chebis,” characterized by using alcohol (locally fermented tella, teji, araki, and borde) and beer at night after having “mirkana,” which is the intoxication (high euphoric stage) of khat during the day. Furthermore, if the consumption of khat is excessive and chronic; individuals might develop a motivational syndrome, culturally called “jezba,” which is characterized by poor self-care, living on the street, using leftover khat leaves, begging for khat, and stealing and fighting for daily khat consumption.
In this study, being addicted to the internet had higher odds of having poor sleep quality than its counterparts. This result is the same as another study done in Taiwan, Turkey, and Japan.46-48 A possible explanation might be that adolescents with poor sleep quality use the internet and other media to cope with sleep problems. 49 Another possible explanation could be that the light produced by electronic devices might disturb circadian rhythms by inhibiting melatonin production. This condition could result in the difficulty of initiating sleep at the right time, as the brightness projected onto the retina from electronic devices sends signals to the sleep center to trigger changes in sleep patterns. 12
In this study, those with physical illness had higher odds of having poor sleep quality than their counterparts. This result is the same as another study done in the USA. 50 The possible explanation might be that long-lasting pain and emotional distress due to chronic medical illness might increase the risk of having poor sleep quality, and excessive psychosocial stress, seizure episodes at night in a case of epilepsy, and adverse effects of drugs among adolescents with medical illness might lead to poor sleep quality. 51 Another possible explanation for having poor sleep quality among adolescents with epilepsy or chronic medical illness could be poor seizure control as a result of delay or not using modern treatment at all. In the culture of the study area or Ethiopia, epilepsy or mental illness is believed to be caused by a supernatural power nowadays. Therefore, priests, shakes, pastors, and other traditional healers are visited by the patients and guardians. The most common practices are drinking holy water and fasting in churches, followed by using traditional medicines. Finally, after a long delay, patients might consider modern treatment options. All these situations might have an effect on the quality of sleep among adolescents with physical and or mental illness.
Inhalant use disorder was also significantly associated with poor sleep quality in this study, and adolescents with inhalant use disorders had about 4 times higher odds of association with poor sleep quality than those without inhalant use. This finding was almost similar to the other studies conducted in Saudi Arabia and Yemen, where the prevalence of inhalant use was high, almost comparable to the current study (16.3%), and sleep quality was poor among inhalant users. 52
In this study, the most commonly used inhalants among adolescents were either gasoline or glue (mastish). The possible reasons why they use inhalants might be that both gasoline and glue are easily available in the area; they are the cheapest, longest-lasting (if bought once, it can be used for a long time), and gives them excessive happiness (euphoria), avoids being hunger, and make them feel energetic.
This finding highlights the need to integrate child mental health services with the trained manpower among Ethiopian hospitals and health centers. There is a single hospital in the capital city of Ethiopia, Addis Ababa, which is far away from the study area to provide child mental health care with a few child mental health clinicians. Due to this, most children or adolescents with mental illness are taken to traditional healers; majorities are treated with holy water, and the rest are given traditional medicines. Due to a lack of trained personnel and insufficient mental health services, not only adolescents but also adults with mental illnesses in Ethiopia are entirely treated by traditional healers. Despite the minister of health putting mental health services as an integral part of other health services, it was not put into action due to lack of priority, shortage of budget, and deep rooted cultural beliefs that mental illness is due to supernatural power, and the main stream of treatment was like drinking and washing with holy water and drinking traditional drugs, and if the patient had no improvement after all this effort, patients were left on the street with no basic needs like food, shelter, and social support. Finally, the recommendation to the minister of health, regional health Brue, and zonal health department is to establish child mental health clinics by integrating them with the already established hospitals and health centers in Ethiopia and to provide at least the WHO MHGAP program in action.
Limitations of the Study
As the existing data shows, this study is the first among adolescents to investigate the prevalence of poor sleep quality and its association with internet addiction, misconduct in school, and physical illness/substance use disorder. However, the scientific community needs to understand the following gaps while understanding the results. The interviewer and participants might have recalled bias and substance use history. The medical records were not checked to confirm their physical illness except checking their medical follow-up cards. The cultural nature of substance use among adolescents from khat cultivating areas may not be generalized to non-khat cultivating areas. Furthermore, the relationship between sleep quality and culturally specific substance use disorders needs further longitudinal study to establish a cause-effect relationship. Finally, because younger adolescents require small amounts of substances to have an adverse effect on their immature body organs, the DSM V substance use disorder criteria may under diagnose adolescent substance use disorders.
Conclusion
The poor quality of sleep was higher among adolescents, and khat and inhalant use disorders, internet addiction, and chronic medical illness were risk factors for poor sleep quality among adolescents. Therefore, Parents, guardians, and Ethiopian schools need to promote sleep hygiene and reduce problematic substance and internet use for adolescents. In addition, awareness creation and working on prevention are crucial strategies.
Footnotes
Acknowledgements
The author is very grateful to the respondents, data collectors, and others who helped during the study.
Author Contributions
The authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mizan Tepi University provided funding for this study. The funders had no role in the study’s design, data collection, analysis, or interpretation, manuscript writing, or the decision to publish the study.
Ethics Approval and Consent to Participate
The procedure was carried out in accordance with the Declaration of Helsinki. The ethical clearance permission letter was obtained from the Mizan Tepi University Research Review Board. After permission letter was given from the selected town health department, the purpose of the study was explained to the participants and their parents. Then, written consent and assent were obtained from the participants and their guardians, respectively, prior to the interview. Participation was completely voluntary and the right to not participate in the study was also secured. Confidentiality was fully ensured in the study.
Availability of Data and Materials
It is possible to get the data set from the authors with a reasonable request.