
Abstract
Nephroblastoma is a renal blast tumor, the most common malignant renal tumor in children between 1 and 5 years of age. The average age of onset is 3.5 years, rarely occurring in children over 10 years of age. Its treatment is a model of medical-surgical collaboration. The prognostic factors are mainly the stage but recent studies have also shown that the advanced age of the child is a negative prognostic factor. We report a case of a 14-year-old child who presented with pain with swelling of the right hypochondrium, ultrasound showed a heterogeneous right retroperitoneal mass, MRI showed a large retroperitoneal tumor process with a right renal origin, in heterogeneous T2 signal, in T1 hyposignal, diffusion restricted, containing necrotic areas and heterogeneously enhancing after injection, responsible for pyelocalic dilatation and right renal venous thrombosis, extended to the IVC and the right atrium, with adenopathies, suggesting first a sarcoma. The extension workup showed pulmonary nodules of secondary appearance. An echo-guided biopsy was performed and the anatomopathological study confirmed the diagnosis of nephroblastoma.
Introduction
Wilms’ Tumor (WT) is the most common type of kidney cancer in children. It affects approximately 1 in 10 000 children worldwide before the age of 15. The median age at diagnosis of WT is approximately 3.5 years. 1 This tumor becomes rarer after the age of 10 years. 2 The most important prognostic factors for patients with WT appear to be stage. 3 In the last decade, age at diagnosis has also been suggested as an important risk factor for recurrence in the COG, UK, and SIOP studies. 4 We report a case of nephroblastoma in a 14-year-old child.
Case Report
This is a 14-year-old child, with no notable history, who presented for 1 month with pain with swelling of the right flank progressively increasing in volume associated with hematuria evolving in a context of altered general condition (asthenia, anorexia, and weight loss). The clinical examination revealed a hemodynamically and respiratorily stable conscious patient with a palpable mass in the hypochondrium and the right flank, painful, and fixed in relation to the deep plane without inflammatory signs or fever. A biological workup was performed and was without significant abnormalities. An ultrasound was performed and showed a right retroperitoneal mass with a right renal origin, heterogeneous, with areas of central necrosis and calcifications (Figure 1). A complementary MRI was performed for a better characterization of the lesion, having objectified the presence of a voluminous retroperitoneal tumor process occupying the right renal compartment, with lobulated contours, heterogeneous T2 signal, T1 hyposignal, diffusion restriction, containing necrotic areas, and heterogeneously enhancing after Gadolinium injection (Figure 2). This process encompasses almost the entire kidney with capsular effraction and pyelocalic dilatation, it pushes back the adjacent digestive and vascular structures, responsible for a voluminous endoluminal thrombus of the right renal vein, extended to the inferior vena cava and to the right atrium and associated with lombo-aortic adenopathies (Figure 3), evoking in the first place a sarcoma. A thoracic CT scan was performed for a workup of extension and showed the presence of secondary pulmonary nodules with pleurisy (Figure 4). An echo-guided biopsy was performed and the anatomopathological study showed cytoplasmic labeling of the tumor cells by the anti-WT1 antibody, confirming the diagnosis of nephroblastoma (Figure 5). Given the deterioration of the general condition, the patient was admitted to the intensive care unit and died a few days later.
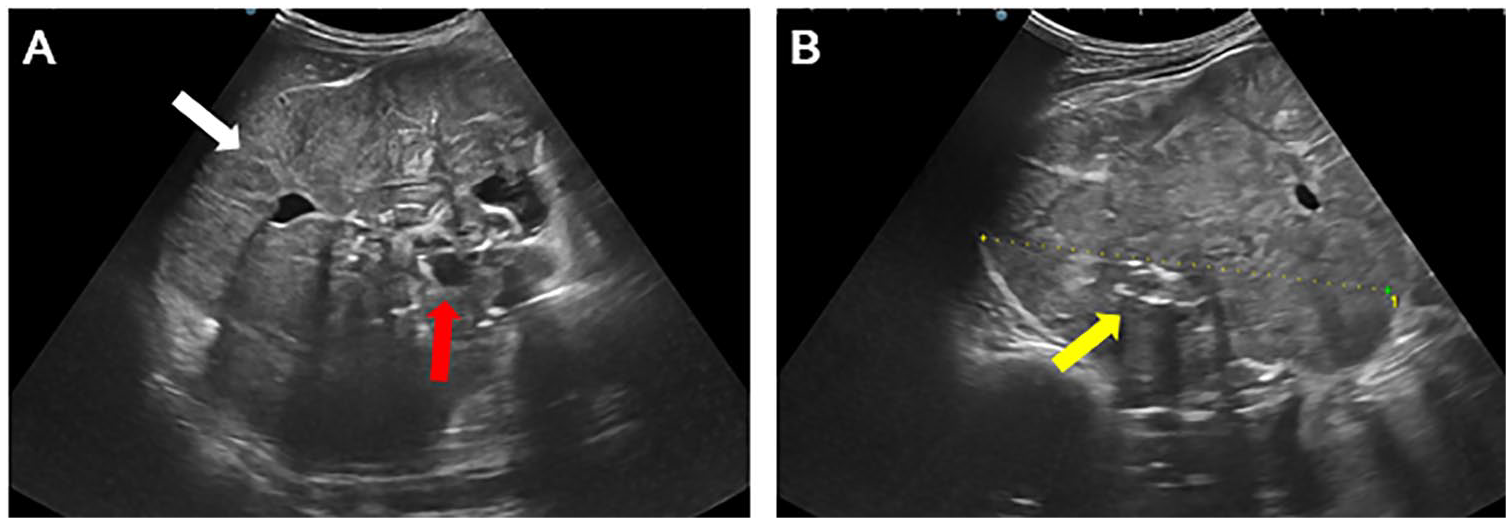
Abdominal ultrasound showing a heterogeneous right kidney (A) (white arrow) with a large, irregular, heterogeneous tissue mass at its upper and middle pole, containing areas of central necrosis (A) (red arrow), and calcifications (B) (yellow arrow).

Axial (A and B) and coronal (C) sections of an abdominal MRI scan showing the presence of a large right retroperitoneal tumor process occupying the right renal compartment in hypo T1 signal (A) with heterogeneous T2 signal (B), containing areas of necrosis and enhancing after Gadolinium injection (C).

Axial (A) and coronal (B) T2 sequences showing reflow of adjacent digestive and vascular structures (white arrow) and a Voluminous endo-luminal thrombus of the right renal vein, extended to the IVC and right atrium (yellow arrow).
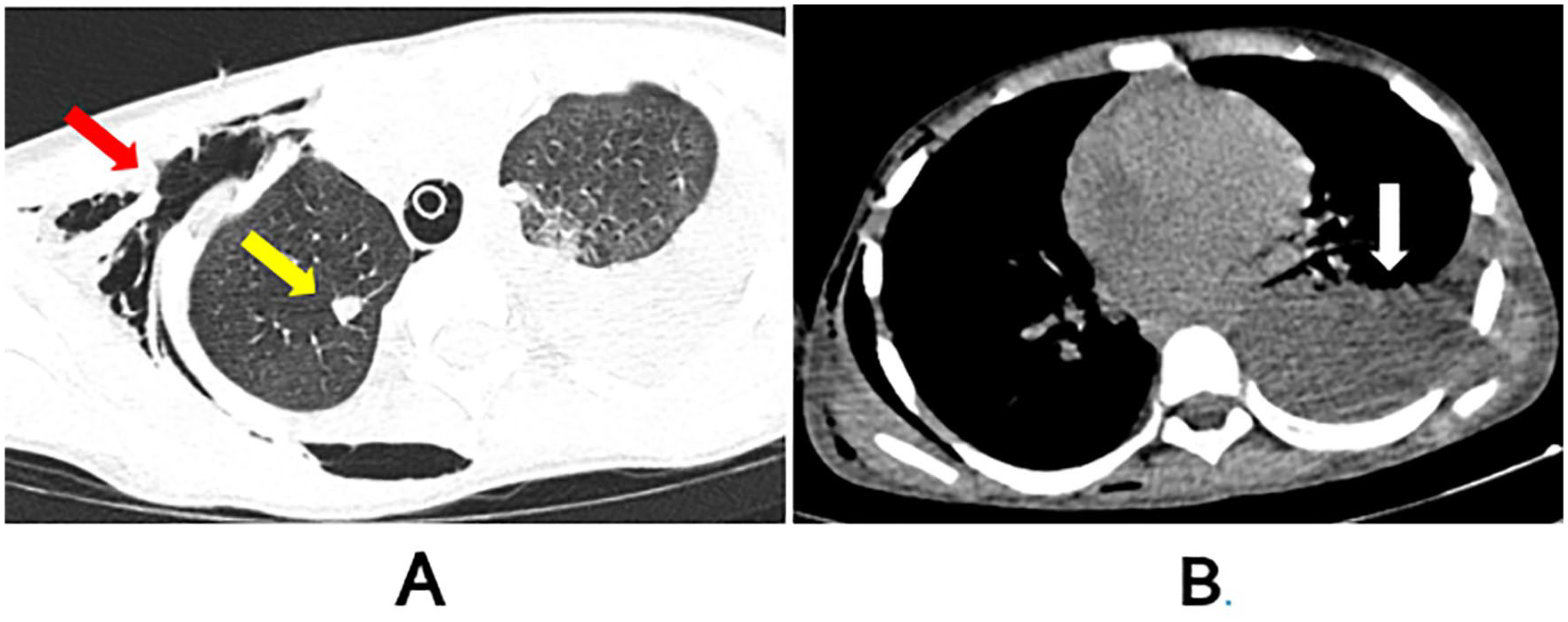
Axial sections of thoracic CT in parenchymal window (A) and mediastinal window (B) showing a metastatic pulmonary nodule (yellow arrow), subcutaneous emphysema dissecting the right cervical and thoracic soft tissues (red arrow), and left pleurisy of small to moderate volume (white arrow).
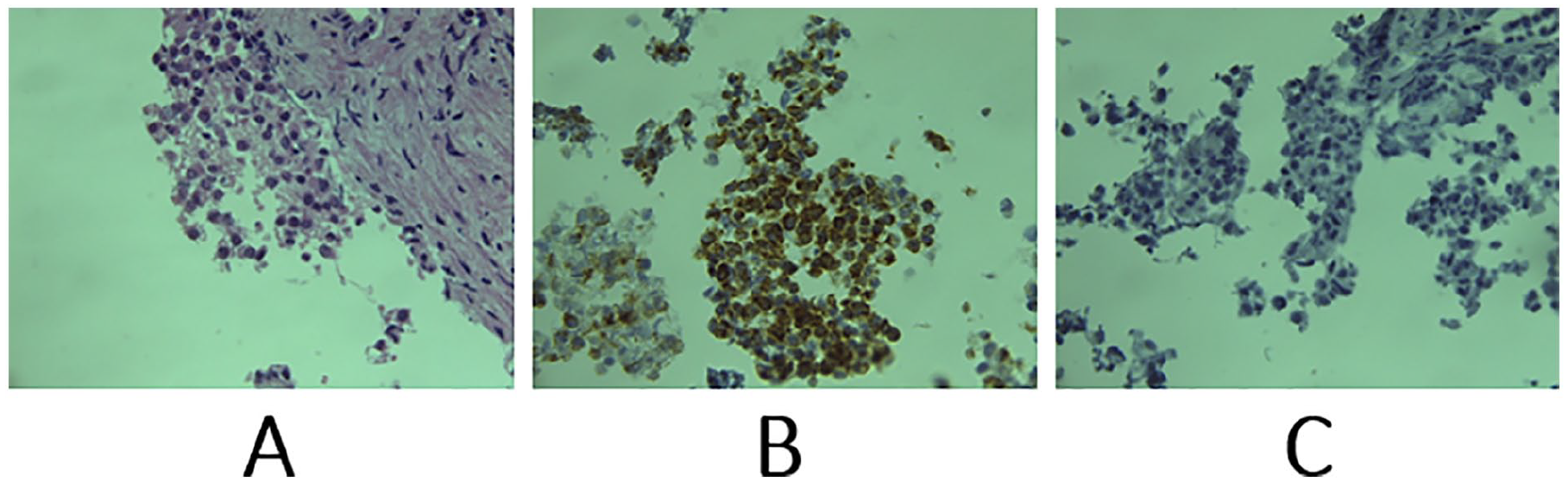
(A) Clusters of round cells with reduced cytoplasm and finely nucleated hyperchromatic with no obvious signs of differentiation. (B) Cytoplasmic staining of tumor cells by anti-WT1 antibody. (C) Absence of anti-LCA antibody staining.
Discussion
Nephroblastoma is an embryonic malignancy developed from cells of the nephrogenic blastula. The tumor cells usually show several differentiation pathways, mimicking the histology of the developing kidney. 5 It is the most common genitourinary cancer in children, affecting approximately 1 in 10 000 children. The average age of diagnosis is 3.5 years, with 98% of cases occurring below the age of 10 years, but this tumor can still occur at any age. 6 About 1 in 10 nephroblastomas is associated with a well-characterized dysmorphic syndrome. The first one is the WAGR syndrome (Wilms, Aniridia, Genito-urinary malformation, Mental retardation) which is associated in 30% of the cases with nephroblastoma, Denys-Drash syndrome, Beckwith-Wiedemann syndrome, Perleman syndrome, Bloom syndrome, and other hypergrowth syndromes.6,7 Sporadic forms are neither familial nor occur in the context of a malformation or predisposition syndrome. They represent more than 90% of nephroblastoma cases. However, cytogenetic studies and systematic searches for loss of alleles (deletion mapping) have identified several regions involved in the genesis of sporadic nephroblastoma: 11p13 (WT1); 11p15.5 (WT2); 16q; 1p; 1q and 17p.8,9
Nephroblastoma occurs with equal frequency in both kidneys and is usually revealed by an abdominal mass. Pain, hematuria, hypertension, and symptoms following traumatic rupture are also common. 6
The purpose of imaging prior to nephroblastoma tumor therapy is to define the extent of disease, assess the contralateral kidney, and determine the presence of tumor thrombus by Doppler ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI).
Ultrasound alone most often ensures the diagnosis of the renal tumor. It is particularly well adapted to small children. It shows the tumor, specifies its retroperitoneal intra-renal location, its volume, its limits, and its relations. There is a pseudo-capsule usually determining with clarity the contours of the mass. It specifies its echogenicity, its solid or cystic nature or most often mixed. It also allows the detection of hemorrhage, necrosis and/or intra-tumoral calcifications. With the help of Doppler, ultrasound can give us information about the vascularization of the kidney, can show the renal artery and the inferior vena cava up to the right atrium. 10
A CT scan is essential before starting the treatment; it allows to identify a renal parenchyma partially surrounding the tumor (spur sign). The mass appears well limited, rounded, sometimes poly-lobed, most often heterogeneous with central hypodense areas after injection of contrast medium, cystic areas and thick partitions. It allows to eliminate another cause of non-tumoral renal mass: renal dysplasia, pyeloureteral dysplasia, horseshoe kidney, xantogranulomatous pyelonephritis, or pseudo-tumoral renal abscess. It complements ultrasound in the exploration of intravascular extensions (thrombosis of the IVC or renal vein), the study of the status of the contralateral kidney, the search for distant metastases and the detection of synchronous nephrogenic remnants on the contralateral kidney. 11
MRI is the main diagnostic tool for the differentiation and staging of renal tumors in children. In recent years, MRI has gained great importance in nephroblastoma imaging and has replaced CT. It provides important information on tumor extent and distant metastasis, venous extent of the tumor in the inferior vena cava. It plays an important role in chemotherapy monitoring and in preoperative planning through volume rendering and three-dimensional post-processing. It shows a retroperitoneal mass with renal origin in T1 hyposignal, heterogeneous signal in T2, restrictive in diffusion, heterogeneously enhancing after injection of Gadolinium and sometimes containing cystic, hemorrhagic or necrotic areas. 12
The metastatic sites are in decreasing order of frequency: lung 50% to 80%, liver 10% to 35%, bone 10% to 35%, brain 3.5% to 7%, adrenal 2% to 5%. 13
The histological variety is of considerable importance with a distinction for the forms of “standard” histology, containing in variable proportion 3 types of tissue: - blastematous, undifferentiated, monomorphic tissue, - tissue with epithelial differentiation (glomeruli, tubules) and mesenchymal elements (fibroblastic or muscular) - and forms of “unfavorable” histology (10% of cases) in particular sarcomatous and anaplastic or predominantly blastematous.6,14
The principles of treatment are based on nephrectomy, which remains the essential stage of treatment. It is always preceded by tumor reduction chemotherapy which greatly facilitates excision, with a minimal risk of tumor rupture and based on clinical and radiological arguments, and without histological evidence. Anatomopathological confirmation of the diagnosis on the excisional specimen and staging determine the postoperative treatment, which is based on chemotherapy and in some cases radiotherapy.14,15
The most important prognostic factors for patients with Wilms’ tumor (WT) appear to be stage, histological subtype, and loss of heterozygosity (LOH) of 1p/16q in chemotherapy-naive WT. In the last decade, age at diagnosis has also been suggested as a risk factor. 16 Several studies have analyzed age as a prognostic factor. These studies found that age <2 years was a favorable prognostic factor, whereas age >4 years was described as an unfavorable prognostic factor. One study specifically addressed adverse outcomes in adolescents. 2 Nevertheless, even in the group of patients with favorable histology, advanced age seems to correlate with a higher risk of relapse and death, although prognostic factors such as stage or histology seem to be more powerful. 17 Other reasons suggested for the adverse survival rates in older children are delayed diagnosis, advanced tumor stage at presentation, and inherently different biological behaviors. 17
Wilms’ tumor is considered one of the most treatable tumors in children, with an excellent survival rate of approximately 85%. However, survival for children older than 10 years is significantly worse, with only 63% 5-year overall survival for children aged 10 to 14 years diagnosed with Wilms’ tumor. 18
Conclusion
Nephroblastoma or Wilms’ tumor is the most common malignant renal tumor in children, representing 90% of all solid pediatric renal tumors. This tumor mainly affects children between 1 and 5 years of age and is rare in older children. Tumor diagnosis is based on imaging, in particular ultrasound, which may be supplemented by CT or MRI. The management is multidisciplinary, combining preoperative chemotherapy, surgery with or without radiotherapy. The indication for surgery depends on the degree of extension, which underlines the importance of preoperative morphological examinations. In the majority of cases, the postoperative prognosis is favorable, especially for young children, making nephroblastoma a model of therapeutic success and multidisciplinarity.
Footnotes
Author Contributions
All authors contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.