
Abstract
Purpose. To compare the sensitivity of axillary and rectal temperature in infants who presents to the emergency department with a recent history of fever. Methods. A single-center cross-sectional comparative study of 201 patients who presents with a recent history of fever. Infants Up to 12 months of age were included. Demographic characteristics such as age and gender, weight, mean axillary and rectal temperatures were documented. Fever is defined as rectal temperature >38°C as opposed to >37.4 in the axillary method. Results. The mean age was 6.1 ± 3.5 months. The mean (SD) rectal-axillary temperature difference was 0.8°C ± 0.7°C which was statistically significant (P < .001). The sensitivity, specificity, positive predictive and negative predictive values of the axillary method for fever >37.4 were 79.34% (95% CI [73-84.9]), 14.3% (95% CI [0.36-57.9]), 96.2% (95% CI [95-97.2]), and 2.4% (95% CI [0.4-13.5]), respectively. Conclusion. The rectal method remains highly important for accurate and prompt diagnosis in infants.
Introduction
Fever is a paramount vital sign that indicate illness in infants.1,2 Accurate temperature measurement is important especially in infants where higher likelihood of sepsis and hospital admission is a concern. 3 Core body temperature is considered the gold standard measure in establishing the diagnosis of fever represented by several methods such as the oral or the rectal routes. In addition, the most reliable site of core body temperature measurement is the pulmonary artery due to its closest to the thermoregulatory center. The bladder and esophagus are also other means of measure. Despite being tremendously accurate, these methods are invasive and not feasible in clinical settings. 4 Multiple other measures have been also used as alternatives to detect fever such as axillary, tympanic and forehead methods due to their readily availability, no risk of perforation, non-invasiveness and little need for patient cooperation, feasibly and easy utilization. 5 Although they pose a wide range of advantages, controversy remains ongoing with regard to their reliability in detecting fever especially in febrile infants.
A considerable amount of literature showed a concern on the accuracy of axillary method due to poor sensitivity as opposed to rectal temperature which cannot be used interchangeably.2,6-10 Some pediatricians also suggest that AT is accurate enough in detecting fever.11,12 However, it has been shown that a high number of false negative results have been reported when the AT method is used especially in infants according to the current standard practice. Despite the controversy, The World Health Organization (WHO) recommend the use of the AT method because of hygiene, safety and perforation risk in the rectal method. 13 Furthermore, recent National Institute for Health and Clinical Excellence (NICE) and pediatrics Italian society guidelines update also recommend against routine use of rectal temperature method and encourage the use of AT measurement in children below the age of 5 despite the ongoing controversy.14-17
In the present study, we will compare the sensitivity of AT and RT in infants who presents to the emergency department in Al-Yamamah Hospital, Riyadh with a recent history of fever in order to implement a proper diagnostic approach to reduce risk of sepsis and decrease the need for delayed hospital admission. Moreover, fever screening requires high level of convenience for patients, families and healthcare providers to ensure fast and easy measurements especially in an overwhelming working environment. We hypothesize that the AT is relatively unreliable to detect fever in febrile infants due to high false negative rate.
Methods
Approval from the institutional review board (IRB) was obtained. Informed consent was waived due to nature of the study. Up to 12 months of age were included. The study was single-center cross-sectional comparative study. Inquiry about the number of patients presented to the pediatric emergency department in Al-Yamamah hospital, Riyadh, Saudi Arabia with history of recent onset of fever from February 2021 until September 2021 yielded a total of 201 patients. The clinical ER triage sheets were evaluated by 2 investigators who managed to obtain all baseline characteristics variables. Any patient with the following comorbidities were excluded 1 : Hematological malignancy 2 immunocompromised 3 hyperthyroidism 4 imperforated anus 5 recent administration of antipyretics medications 6 congenital anal or rectal malformation. None of the reviewers were involved in any medical care for the patients included. Baseline characteristics such as age, gender, weight were noted. The temperature was measured for each patient using both the axillary and rectal methods at the same time. Fever is defined as RT > 38°C as opposed to >37.5 for AT. 18 Nevertheless, several cut-off values were considered for AT ranging from 37.2°C to 37.5°C to identify changes in the accuracy of temperature agreements between the 2 methods. 19 Electronic thermometer was used and set differently for each method according to manufacturer setting (Welch Allyn SureTemp Plus Electronic Thermometer (Model 692), Wall Mount).
Statistical Analysis
Continuous variables with a normal distribution were represented as mean ± standard deviation (SD). Categorical variables were depicted as numbers and percentages. Test of normality checked by Kolmogorov Smirnov test. ROC (Receiver operating characteristics) was carried out to determine the sensitivity and specificity of axillary and rectal temperature test for robust and accurate measurement of fever. Cross tabulation was used to predict sensitivity, specificity, PPV and NPV when applicable. Paired sample t-test was used to compare the differences between temperature readings that are normally distributed. Pearson’s correlation between axillary and rectal temperatures was determined. The degree of agreement was evaluated using the Bland-Altman method. P < .05 was considered statistically significant. 95% confidence interval (CI) and P-value were obtained for the independent variables. Data analysis was carried out by SPSS 25.0 (IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.).
Results
The 201 infants who were considered for the analysis had a mean age of 6.1 ± 3.5 months. The study had 111 (55.2%) males and 90 (44.8%) females. The mean weight was 7.4 ± 2.1 kg. All infants underwent axillary followed by RT measurement upon triage in the emergency department. The median IQR for age at triage was 6.12 (3.04-9.1) months. Demographic characteristics of infants enrolled in the analysis are shown in Table 1. The correlation between the 2 methods was linearly significant (P < .001) (Figure 1). In order to establish the optimal cut-off/threshold values of axillary fever to determine the best sensitivity and specificity for the study test, we performed ROC analysis by plotting sensitivity against 100-specificity at different cut-off values of axillary temperature. By using, the value axillary temperature >37.4 detect the positive case of axillary fever.
Demographic Characteristics of Infants Enrolled in the Study (N = 201).


Scatterplot of rectal and axillary temperatures in the pediatric emergency department triage setting (n = 201). (Pearson’s correlation R = 0.4, P < .001).
The mean (SD) rectal-axillary temperature difference was 0.8°C ± 0.7°C which was statistically significant (P < .001). The range of temperature difference from the mean was −0.7°C to 0.9°C. The Bland–Altman plot was constructed to show the level of agreement between each axillary and rectal readings (Figure 2).
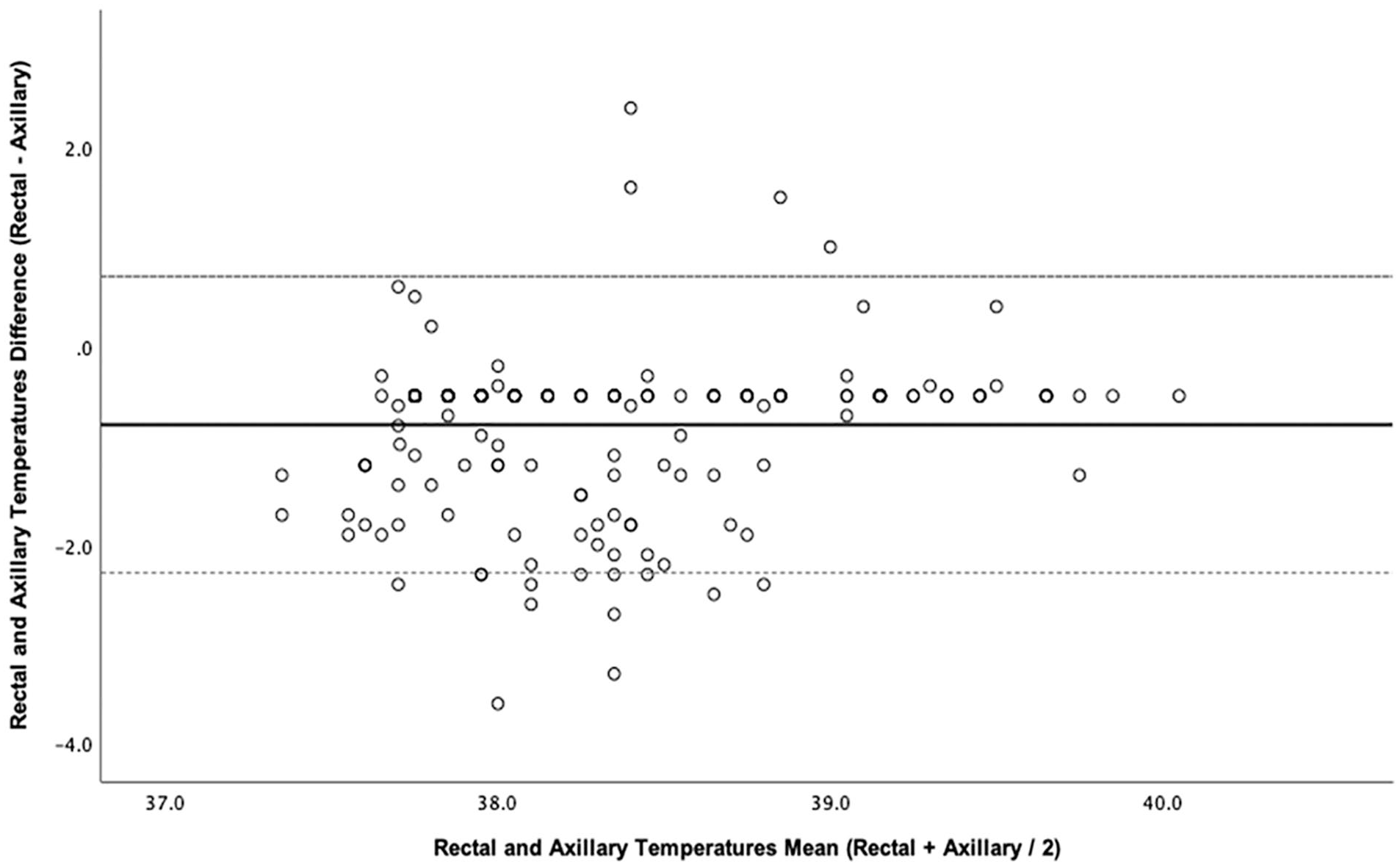
Scatterplot of the Bland–Altman method for rectal and axillary temperatures measurements in pediatric emergency department triage. The solid line illustrates the mean difference of both rectal and axillary and the dashed lines illustrate the 95% agreement limits.
The sensitivity, specificity, PPV and NPV of the AT for fever > 37.4 were 79.34% (95% CI [73-84.9]), 14.3% (95% CI [0.36-57.9]), 96.2% (95% CI [95-97.2]), and 2.4% (95% CI [0.4-13.5]), respectively. Some of the diagnostic parameters for the axillary methods based on different age groups are shown in Table 2.
Sensitivity and PPV of the axillary method according to different age groups.

Discussion
Fever is a very common complaint that is encountered almost daily in any emergency department. 20 Accurate temperature measurement is crucial in order to minimize risk of sepsis in infancy. Despite explicit research about the safety and accuracy of AT measurement method, conflicting published data about how accurate the AT method compared to RT in detecting fever is available for infants. Moreover, AT has been widely used for fever screening in pediatric emergency departments due to safety, hygiene and convenience for patients, families and the nursing staff. However, a concern regarding high false-negative rates 21 especially when the heart rate is elevated renders pediatricians to doubt the accuracy of AT and require the use of core temperature measurement such as the rectal method. The sensitivity of the AT compared to RT has not been investigated extensively in the infants age group. In addition, information about the association between infant age groups and level of AT sensitivity is minimal. Most published data were merely on newborns and neonates.6,10,22-25 Our study explicitly investigates the accuracy of AT measurement compared to the gold standard RT in the context of different infantile age groups.
The relationship between the RT and AT was assessed using the Bland–Altman analysis. It shows a mean difference of 0.8°C with a 95% CI range of ±1.5°C which indicates a large difference between the 2 methods. The difference is considered significant due to a narrow range of normal temperature between 36.5°C and 37.5°C. 18 The febrile infants would be more likely to be missed if the difference was up to 1.5°C with such a narrow normal range for AT allowing them to succumb to complications. The first to show poor agreements between AT and RT was a meta-analysis done by Craig et al, pooled mean rectal-axillary temperature measurements difference was 0.25°C for mercury thermometers (95% CI, −1.5 to 0.65) and 0.85 °C (95% CI, 0.19 to 1.9) for the electronic thermometer. The latter reflects a similar result found in our study for the electronic thermometer. The majority of studies included in the pooled analysis of the electronic thermometer were performed on young children other than neonates allowing for more consistency to our findings. Although the mercury thermometer seems to provide a more accurate agreement between the 2 methods, it’s no longer being used due to fear of mercury toxicity and has been replaced by a more convenient and safer digital thermometer. 8 Furthermore, a recent study by Teller et al 26 performed on children <24 months presenting with fever also discovered a rectal-axillary mean difference of 1.1°C with 95% limit of agreement between 0.32°C and 1.98°C which confirm our findings.
Jones et al 27 conducted a study on 573 children under the age of 5 on Gambia, West Africa. They found 98% sensitivity of AT for the detection of fever. Although the sensitivity is extremely high, the authors argues that the reason for is due to the high prevalence of tropical infectious diseases such as malaria in Africa. Tropical infectious diseases are well known to present with a high-grade fever allowing for a higher likelihood of detection by the axillary method. On the contrary, several other studies performed on infants report a various sensitivity to our study (73%, 2 81%, 28 64%, 29 62%, 30 and 49% 21 ). The reason for this variation might be attributed to the measurement device that has been used, the different age groups enrolled, different ambient temperatures or children weight difference for height. It has been shown in multiple subgroup analysis that neonatal fever was detected with a high sensitivity by the axillary method resembling similar findings to our study.8,30 Thus, a potential effect on accuracy is possible when considering the age factor.
Our analysis suggests that AT is less sensitive at detecting fever >37.4°C upon patient triage in the emergency department. It may miss approximately 20% of infants with rectal hyperthermia. Shine et al 31 performed a comparison analysis exactly similar to our study and found nearly comparable results (29% false negative rate using AT). Subgroup analysis suggests that the AT is quite sensitive for infants <3 months as opposed to markedly decreasing sensitivity for infants in the older age groups. The latter finding was also reported in another studies.8,31 An explanation for this difference may be related to body weight. Children with a low weight for height seems to have less wider range between the 2 methods compared to children with an average weight for height. Another explanation is a possible difference in the physiological mechanisms of thermoregulation for each age groups. Further investigation into this aspect should be sought for future studies.
To allow for a more convenient temperature measurement for families and healthcare providers, several lower than the normal cut-off value may be considered for AT measurement ranging from 37.2°C to 37.4/37.5°C. Lowering the cut-off value for the diagnosis of fever would substantially decrease the false negative rate. AT of 37.4/ 37.5°C, 37.3°C, 37.2°C showed a sensitivity of 79%, 83%, and 86%, respectively.
Limitations
Several limitations in our study should be taken into consideration. The design of the study is cross-sectional comparative study. It may have an impact on increasing the sensitivity level. However, that was not observed in our analysis and the result reflects similar findings from other studies. Furthermore, the measurement of temperature may be affected by subjective techniques performed by the nursing staff. Some patients were excluded from the study due to a lack of rectal temperature readings.
In conclusion, the axillary temperature measurement represents a poor screening method and should not be considered accurate enough as an alternative to the rectal temperature method for the detection of fever in infants older than 3 months with a recent history of fever. The rectal method remains highly important for accurate and early diagnosis in the clinical context of suspected underlying infectious or inflammatory processes for this age group.
Footnotes
Authors’ Contributions
Authors testify that all persons designated as authors qualify for authorship and have checked the article for plagiarism. If plagiarism is detected, all authors will be held equally responsible and will bear the resulting sanctions imposed by the journal thereafter.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Individual Contribution: Quantitative Analysis
Ethics Approval and Consent to Participate
Approval from the institutional review board (IRB) of King Fahad Medical City (KFMC) was obtained [1RB00010471]. Informed consent was also waived by the institutional review board (IRB) of King Fahad Medical City (KFMC) research center due to nature of the study. All procedures performed in studies involving human participants were in accordance with ICH GCP guidelines and ethical standards of the institutional research committee in King Fahad Medical City (KFMC), Riyadh, Saudi Arabia as well as with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. IRB [1-056C]. IRB registration Number with KACST, KSA: H-01-R-012. IRB registration number U.S. Department of HHS IORG: 1RB0001047.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.