
Abstract
A preadolescent female presented to the emergency department with an acute asthma exacerbation. Chest radiograph and computed tomography scan showed extensive pneumomediastinum with a small pneumopericardium without a distinct source for this air leak. The patient was admitted for noninvasive monitoring, analgesia, and high concentration oxygen. Serial chest radiographs showed marked improvement following high concentration oxygen, and she was discharged on hospital day 3. Spontaneous pneumomediastinum and pneumopericardium are rare complications of asthma that can often be managed conservatively but should be considered on the differential for this patient population, and may be a complication of COVID-19.
Case
A 10-year-old female with a strong family history of asthma and recurrent wheezing following a COVID infection 5 months earlier presented to the emergency department (ED) with cough, wheezing, and respiratory distress. Upon presentation, she was treated for an acute asthma exacerbation with continuous nebulized albuterol and intravenous corticosteroids. Chest radiograph showed extensive pneumomediastinum with possible pneumopericardium (Figure 1A, B). Chest computed tomography (CT) confirmed a small amount of pneumopericardium with air extending into the soft tissues of the lower neck, and no obvious source of the air leak. Despite the pneumopericardium, she showed no signs of pericardial tamponade and cardiac deterioration. The patient was admitted and received noninvasive monitoring, analgesia, and high concentration oxygen to promote nitrogen clearance. Serial chest X-rays showed marked improvement following high concentration oxygen, and she was discharged on hospital day 3 (Figure 1C).
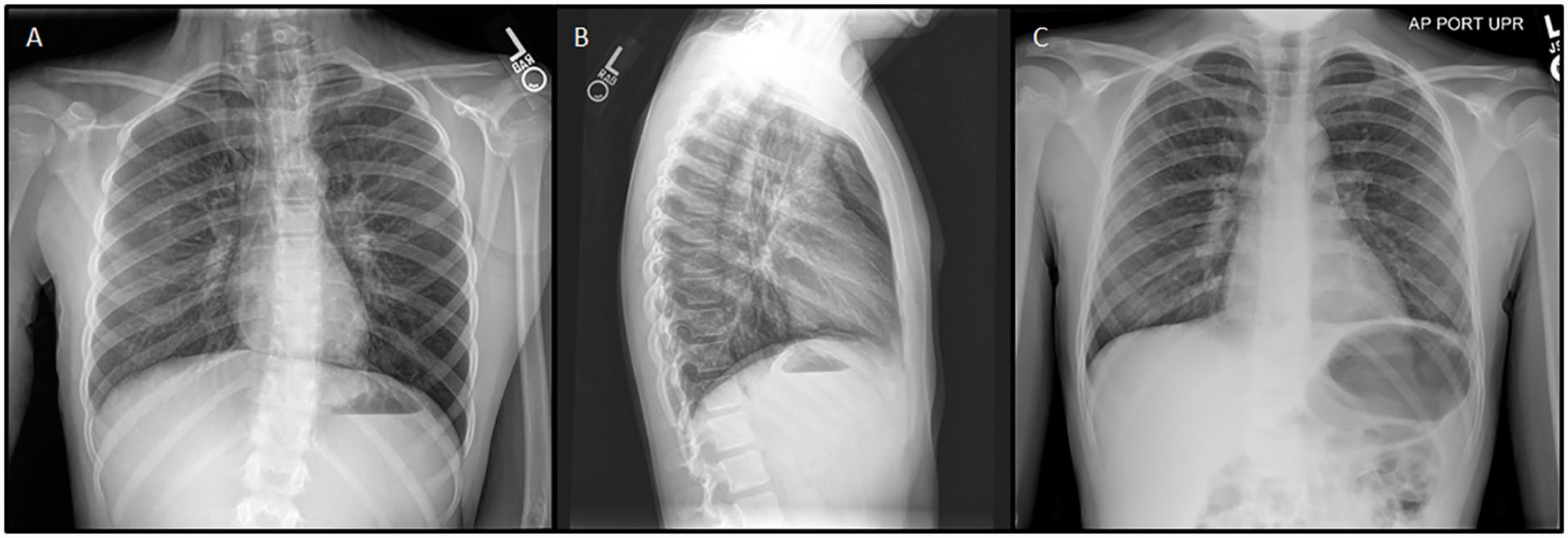
(A) Anteriorposterior chest radiograph and (B) lateral chest radiograph showing extensive pneumomediastinum and a small pneumopericardium from day of admission. (C) Anteriorposterior Chest radiograph showing resolution on hospital day 2.
Discussion
Spontaneous pneumomediastinum (SPM) and pneumopericardium are rare conditions in which there is an abnormal presence of air in the mediastinum and pericardial cavity. The incidence of SPM has been reported at 0.0025% among emergency room visits. 1 In most cases, it is a self-limiting condition that can be managed conservatively and does not always require hospitalization. Asthma appears to be the most frequent predisposing risk factor in children likely due to forced valsalva leading to alveolar rupture that then allows the bubbles of gas to disseminate along the pulmonary vasculature to the soft tissue of the cervical region through fascial planes connecting these areas.2-4
It has been well documented that COVID-19 can lead to significant IL-4 induced airway remodeling. 5 This patient had been experiencing intermittent wheezing the previous 5 months only after an episode of COVID-19. Given the absence of major triggers (eg, forceful coughing and vomiting), it is likely that what lead to her SPM was the mild cough/wheeze in an already compromised lung. This may be an additional complication of COVID-19 and warrants further investigation.
Thorough clinical history, physical examination, and chest radiographs are most often diagnostic, and there is rarely a need for further investigation. 6 Lateral neck radiograph has a higher sensitivity for the demonstration of subcutaneous emphysema specifically. 6 Chest CT has fallen out of favor to confirm the diagnosis and should only be considered if the patient shows any signs of deterioration, or if there is any uncertainty with respect to the diagnoses.1,7 Treatment is generally conservative, consisting of analgesics, oxygen therapy, and treatment of any underlying conditions (ie, asthma exacerbation). Breathing high concentration oxygen has been advocated to reduce the partial pressure of nitrogen in the subcutaneous air, which allows acceleration of its resorption. 3 Clinically stable SPM can be managed outpatient with observation. 8 However, according to a meta-analysis, 25.8% of patients required transfer to the intensive care unit. 2 This demonstrates that although supportive therapy is sufficient in most cases, close follow-up is crucial as there is a substantial risk of clinical decline. Although there is a risk of superimposed bacterial infection, complications are rare, and prophylactic antibiotics are unnecessary in the majority of cases. 9 Recurrent SPM may occur in children with underlying asthma, and care should be taken to assure these children remain well controlled in terms of their symptomology. 1 Recommendation should be made that physical activities associated with the development of pneumomediastinum (eg, weight lifting, scuba diving, playing wind instruments) should be minimized for at least 6 months.
Footnotes
Author Contributions
All of the authors contributed equally to the preparation and editing of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent
Patient consent was obtained for publication of patient information. Ethical approval was not sought as no interventions took place, and patient anonymity and confidentiality were maintained.