
Abstract
This study aimed to compare growth and pubertal developmental parameters among HIV-infected and uninfected adolescent girls (11-19 years) in Lagos using a cross-sectional approach. Height, weight, BMI Z-scores, sexual maturity rating by Tanner stages and age at menarche, were compared in the 2 groups. The mean age was similar in both groups (13.2 [±2.3] years and 13.6 [±1.6] years for HIV positive and negative respectively [P = .13]). Majority (66.2%) were in Junior Secondary classes and the mean socioeconomic class was 2.5 (±0.9). HIV-infected girls had significantly lower height, weight, and BMI Z scores compared to their uninfected counterparts. The proportion that had attained Tanner stages 3 to 5 were significantly lower among the HIV-positive participants. The study identified lower growth parameters and pubertal delay among HIV-infected adolescent females compared to HIV uninfected girls. Growth and sexual maturation assessment should form part of routine care of adolescents living with HIV.
Introduction
HIV/AIDS remains a major global public health challenge almost 4 decades after its emergence in the early 1980s. However, improvements in diagnosis and treatment, especially access to highly active antiretroviral therapy, have turned a once lethal disease into a chronic manageable condition, with a reasonable prospect of long healthy lives for infected persons.1,2
This success has led to increased survival of children perinatally infected with HIV into adolescence and adulthood.3,4 Horizontal transmission of HIV to adolescents also contributes to the increasing numbers of adolescents living with HIV (ALHIV), raising the population by 30% from 2005 to 2016.5-7
However, the catabolic, chronic inflammatory, and immunosuppressive nature of HIV infection have raised concerns about its impact on the skeletal growth and pubertal maturation of infected adolescents. This concern is corroborated by observations of impaired growth and sexual maturation in adolescents with other chronic diseases such as sickle cell disease, severe asthma, cystic fibrosis, and chronic kidney disease.8-12 Onset at a younger age and greater severity of chronic illness have a greater negative effect on growth and sexual maturation. 8
Several reasons are adduced for this growth and pubertal delay. The adverse effects of inflammatory markers and undernutrition on the growth hormone (GH)—insulin-like growth factor-1 (IGF-1) axis are thought to impact negatively on metabolic and endocrine functions. 12 Furthermore, low levels of the hormone leptin, resulting from poor nutrition and reduced energy reserves in chronic illness also have a negative effect on the hypothalamic-pituitary-gonadal axis, leading to reduced pulsatile release of gonadotrophin releasing hormone (GnRH) and disruptions in pubertal development.12-14
In addition to the burden of chronic illness, growth, and pubertal delay in adolescents can also be associated with some long-term negative consequences, which include reduced adult height and bone mineral density, poor psychosocial functioning, and educational attainment, as well as increased susceptibility to metabolic and cardiovascular disorders. 15 In view of this, early detection and efforts at mitigation of suboptimal growth and delayed sexual maturation should be part of the routine care of children with chronic illness.
While various studies have documented evidence of delayed growth and pubertal maturation among ALHIV,16-21 few of those studies have emanated from the West and Central Africa, which hosts the second-largest HIV epidemic, behind Southern and Eastern Africa. 22 The region is also burdened with poverty and malnutrition, thus compounding the case for poor growth and pubertal delay among HIV-infected children and adolescents. 23 Furthermore, HIV-positive adolescents (10-19-year-olds) make up 7.0% of the HIV-positive population in Nigeria. 24 Thus, there is a significant population of HIV-infected adolescents in the country but limited reports on their growth and pubertal development.
There is evidence that prompt recognition and appropriate intervention can reverse growth delays in some adolescents with chronic illness so that they eventually attain expected adult height for their sex and racial groups. 12 Several works have shown that combination antiretroviral therapy with improved nutrition among children with HIV infection is associated with positive trends with respect to growth.16,25,26 Assessment of growth and pubertal development in HIV-infected children and adolescents will help identify deficits if any, so that appropriate and timely interventions can be instituted. This study, therefore, aimed to compare growth and pubertal development among HIV infected and uninfected adolescent girls in Lagos State using anthropometric parameters and pubertal stages.
Methods
Study Design and Setting
This was a cross-sectional comparative study among female adolescents living with HIV [ALHIV] and accessing care at the HIV Care and Treatment Centre at the Nigerian Institute of Medical Research (NIMR), Yaba, and apparently healthy HIV uninfected adolescent girls at a girls’ only secondary school also at Yaba, in Lagos State, Nigeria. The NIMR HIV Centre, established in 2002, provides comprehensive HIV care and treatment services to adults, pregnant women, and children and had a cumulative enrollment of over 25 000 by the end of 2020. The Adolescent Clinic of the Centre, which commenced operations in 2014, attends to the clinical and psychosocial needs of male and female adolescents living with HIV.
Study Population
HIV-positive and negative female adolescents aged 10 to 19 years comprised the study population. Those who were acutely ill or who could not provide consent or assent were excluded from the study. The current on-care patients attending the Adolescent HIV are 258, approximately 50.0% of whom are females. All eligible participants attending the clinic who provided consent/assent for the study were enrolled as participants. Using a 1:1 ratio of HIV positive and negative participants, the final study sample size was 115 female ALHIV and 118 apparently healthy HIV uninfected adolescents.
Study Procedure
After obtaining informed parental consent and assent from prospective participants aged <18 years and informed consent from those aged ≥18 years, socio-demographic characteristics including age, ethnicity, educational level, and parental education and occupation (used to calculate socioeconomic status according to the method by Oyedeji 27 ) was obtained with a questionnaire. Menstruation status and age at menarche, if already attained, were recorded in the questionnaire. Thereafter the height (to the nearest 0.5 cm) and weight (to the nearest 0.1 kg) were measured with the participant lightly clothed and on bare feet with the Seca weight and height meter combination (Seca GMBH & co. kg. 22089 Hamburg, Germany). The body mass index (BMI) was calculated from the weight and height values. The Z scores for age for height, weight, and BMI were obtained using the WHO growth charts and the Pedz Pediatric Body Percentile Calculator.28,29
Pubertal maturation was assessed by visual inspection using the 5 stages of breast and pubic hair development described by Marshal and Tanner (Tanner Stages). 30 Images of the different Tanner stages for breast development and pubic hair development were compared with each participant’s breast and pubic hair and used to assign the breast and pubic hair stage for that participant. Only 1 member of the study team performed the visual examination for breast and pubic hair stage to avoid inter-observer error. The observed stages were recorded in the participants’ case report form.
Data Management
Study data were entered into a Microsoft Excel spreadsheet, cleaned, and transferred to SPSS for windows (version 23) software for analysis. Student’s t-test and Chi-square test were used to compare population means and population proportions between the 2 groups respectively. The level of significance (α) was set at 0.05.
The proportion of participants that had attained menarche and the mean age at menarche was compared between the 2 groups. The effect of growth parameters on menarche status was also compared between the 2 groups.
Ethical Consideration
Ethical approval for the study was obtained from the NIMR Institutional Review Board and permission obtained from the management of the mission school.
Parents were informed about the study at a Parents/Teachers Association (PTA) meeting and students were given the parental informed consent form to take home for parental consent. Participants below 18 years of age signed an assent form in addition to parental consent.
Inability to provide parental consent/assent made the student ineligible to participate in the study. The consenting process took place at the HIV clinic for the participants living with HIV.
Privacy and confidentiality were maintained; the visual observation for the Tanner staging was conducted in the consulting room of either the mission school clinic or the HIV clinic as appropriate. Study data were de-identified as only study numbers were used to identify participants.
Results
Socio-Demographic Characteristics of Study Participants
Table 1 gives the details of the sociodemographic characteristics of the 233 study participants. The mean age of all participants was 13.4 (±2.0) years, and this was similar across the 2 groups of participants (13.2 [±2.3] years vs 13.6 [±1.6] years in the HIV infected and uninfected respectively).
Sociodemographic Characteristic of Participants.

Mean (±SD): Mean (±standard deviation).
OR [95% CI]: Odds Ratio [95% Confidence Interval].
S/D Orphan: Single/Double Orphan.
Majority of participants were of the age group 13 to 15 years (51.5%), in Basic classes 1 to 9 (66.2%), and from 2 major tribes in Southern Nigeria (Igbo: 41.5% and Yoruba: 34.5%). The mean socioeconomic class for all participants was 2.5 (±0.9). The mean socioeconomic class was 3.0 (±0.9) and 1.8 (±0.8) among HIV positive and negative participants respectively.
Thirty-eight (33.0%) of the HIV-infected adolescents were either single or double orphans and 3 (2.5%) of the HIV uninfected participants were single orphans. There were no double orphans among the HIV uninfected cohort.
Growth Assessment of Participants
The anthropometric parameters of height, weight, and body mass index (BMI) were used to assess growth among the participants. The mean Z scores for all the participants were −0.69 (±1.5), −0.59 (±1.69), and −0.25 (±1.4) for height, weight, and BMI respectively. The mean z scores for height, weight, and BMI were all significantly lower among the HIV-positive participants (P < .001). Significantly higher proportions of HIV positive participants had Z scores ≤ −1.0 (67.2% vs 14.4%), (59.1% vs 12.7%), (37.4% vs 5.1%) for height, weight, and BMI respectively, than their HIV negative counterparts (P < .001) as depicted in Table 2.
Anthropometric Parameters of Study Participants.

Pattern of Pubertal Development Among Study Participants
Pubertal development was assessed by breast and pubic hair development using the Tanner Staging for pubertal development. For breast development, the majority of participants were in Stage 3 (29.5% and 50.0% for the HIV positive and negative respectively) while for pubic hair development majority of HIV positive adolescents (26.1%) were in stage 2 and a majority of HIV negative adolescents (60.9%) were in stage 4. HIV-positive participants were significantly less likely to be in Tanner stages 3 to 5 for both breast and pubic hair development than HIV negative participants (50.4% vs 94.1% and 21.7% vs 93.2% respectively; P < .001).
The mean age at menarche was also significantly higher among the HIV-positive participants (13.2 [±1.7] years vs 11.8 [±1.1] years; P = .002). The proportion of participants that had attained menarche was significantly lower in the HIV-positive participants (41.7% vs 83.1%; P < .001).
The proportion that had attained menarche increased with increasing age in the 2 groups. However, the proportion that had attained menarche was significantly lower in the HIV-positive participants in the 10 to 12-year and 13 to 15-year age groups (P < .001). All HIV-negative participants in the 16 to 19-year age group had attained menarche, compared to 77.8% in the HIV-positive participants.
The pattern of pubertal development among the study participants is shown in Table 3.
Pattern of Pubertal Development Among Study Participants.
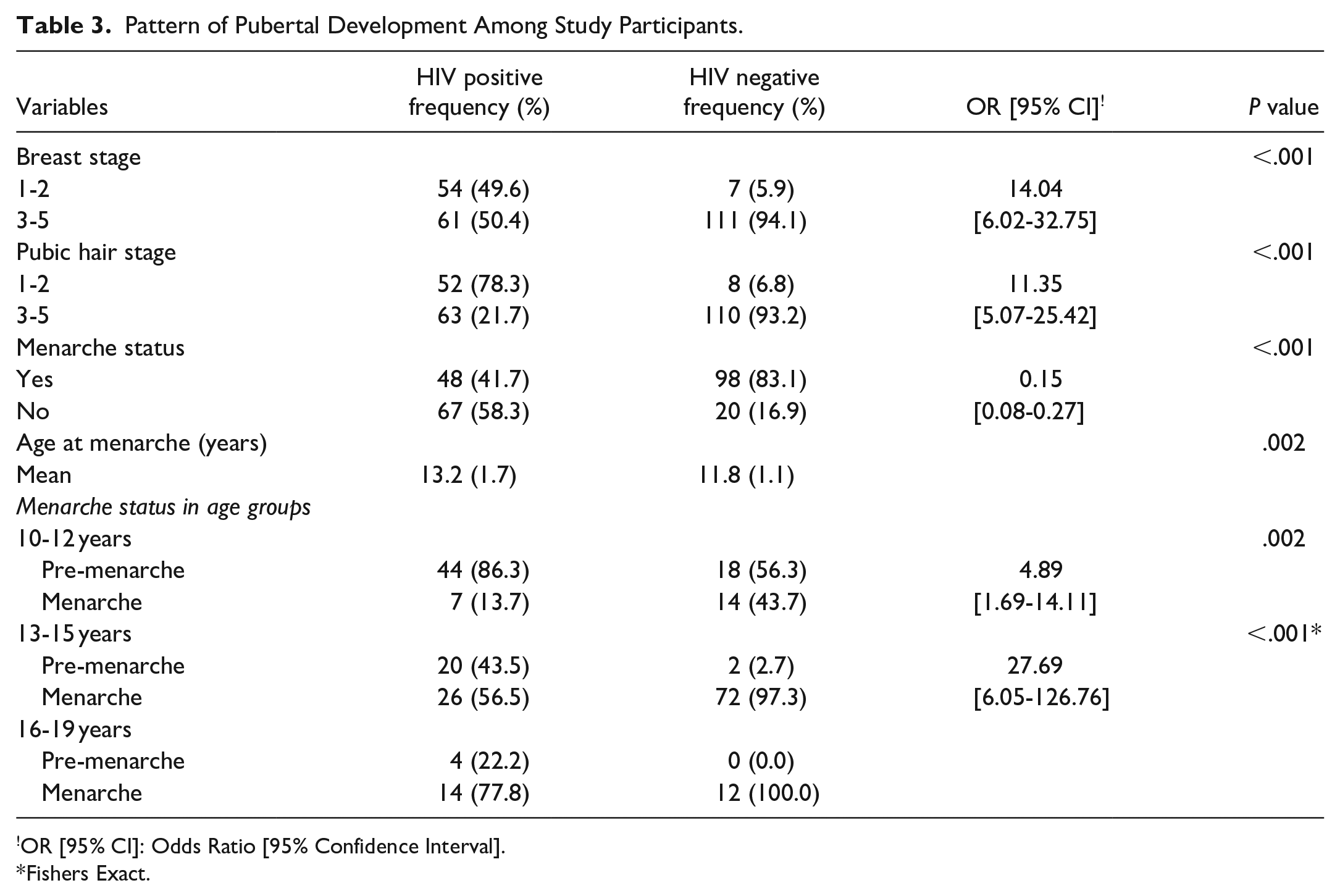
OR [95% CI]: Odds Ratio [95% Confidence Interval].
Fishers Exact.
Menarche Status and Anthropometric Parameters in ALHIV
We compared the proportion of adolescent participants living with HIV who had attained menarche and the mean age at menarche at Z scores ≤ −1 and >−1 for height, weight, and body mass index parameters.
Participants with BMI Z scores ≤ −1 had significantly lower proportion who had attained menarche (23.8% vs 52.1%, OR [95% CI]: 0.29 [0.12-0.67], P = .009) and a higher mean age at menarche compared to those with Z scores > −1 (14.3 [1.8] years vs 13.0 [±1.5] years, P = .021).
For height and weight Z scores, while the proportion with menarche was significantly lower in those with weight Z scores ≤ −1 (P = .001), there was no significant difference for those with height Z scores ≤ −1 or >−1 (P = .491).
Similarly, while the mean age at menarche was significantly higher in those with height Z scores ≤ −1 (13.7 [±1.5] years vs 12.6 [±1.6] years; P = .026), there was no significant difference in those with weight Z scores ≤ −1 or >−1 (P = .151). This is described in Table 4.
Menarche Status and Anthropometric Parameters in ALHIV.

OR [95% CI]: Odds Ratio [95% Confidence Interval].
SD: standard deviation.
Discussion
Growth and pubertal development are an important index of health among the adolescents that requires close attention especially among individuals with chronic illnesses such as HIV infection. The study compared the growth and pubertal development of adolescent girls living with HIV and age-matched HIV uninfected girls in Lagos, Nigeria. Findings showed significantly lower growth parameters (height, weight, and BMI Z scores) among the HIV-infected participants. HIV-positive participants were also significantly more likely to be in lower Tanner stages (1 and 2) for both breast and pubic hair development than HIV-negative participants (49.6% and 48.7% compared to 5.9% and 7.3% respectively; P < .001). Furthermore, HIV-infected participants attained menarche significantly later than their HIV-negative counterparts (13.2 [±1.7] years vs 11.8 [±1.1] years; P = .002). The proportion of HIV-positive participants that had attained menarche was also significantly lower. For HIV-infected participants, height, weight, and BMI Z score ≤ −1 scores were all associated with higher age at menarche.
The poor growth pattern among adolescents living with HIV in our study is similar to findings from sub-Saharan Africa, Europe, and the USA.31-33 However, the marked difference between our 2 cohorts could be attributed to the poorer socioeconomic status and higher orphan status of the HIV-positive cohort, with consequent poorer nutritional intake, as well as the malabsorption, and recurrent infections associated with HIV infection.
While the early institution of antiretroviral therapy is one of the strategies to prevent or mitigate growth impairment in HIV-positive children and adolescents, studies have shown that already established growth impairment can persist despite the commencement of antiretroviral drugs. 31 Our findings buttress this observation, as all our HIV participants were on antiretroviral drugs and still showed significantly reduced growth parameters compared with their HIV-negative counterparts.
The delayed pubertal development (as demonstrated by breast and pubic hair stages of sexual maturation) and increase in mean age at menarche of 1.4 years (from 11.8 years in the HIV uninfected to 13.2 years) among the HIV infected participants in our study is per findings from similar studies from within and outside the African continent.16-21,31-33 Reasons for this delay could be the lowering effect of poor nutrition and proinflammatory cytokines on leptin hormone levels and pulsatile release of gonadotrophin releasing hormone (GnRH) leading to disruptions in pubertal development as described by other workers.12-14
In the current study, among the HIV-infected cohort, lower height, and BMI z scores were significantly associated with delayed age at menarche, while the proportion of participants that had attained menarche were all significantly less among those with height, weight, and BMI z score less than −1.0. This finding affirms the complex interplay between growth parameters, especially height and BMI, and onset of puberty. 33
In conclusion, the findings buttress the need for continued close monitoring, evaluation, and prompt management of the adolescent living HIV by the primary caregiver and healthcare providers to enable early detection of poor growth and delayed sexual maturation and institution of appropriate management strategies to optimize survival and quality of life.
Limitation
The study did not include male HIV positive and HIV negative adolescents so the effect of HIV on growth and pubertal development among male adolescents could not be assessed. This will be addressed in future studies.
Footnotes
Acknowledgements
The authors acknowledge the help of Oba Abdulrasheed with the statistical analysis.
Author Contributions
David Nkiru: Conception of study, developed and supervised data extraction and findings, and wrote the manuscript.
Gbaja-biamila Titilola: Conception of study, developed and supervised data extraction and findings, and wrote the manuscript.
Salako Abideen: Conception of study, developed and supervised data extraction and findings, and wrote the manuscript.
Odubela Oluwatosin: Conception of study, developed and supervised data extraction and findings, and wrote the manuscript.
Wapmuk Agatha: Carried out the study, analysis of work, helped shape the research findings, provided critical feedback and wrote the manuscript.
Ekama Sabdat: Carried out the study, analysis of work, helped shape the research findings, provided critical feedback and wrote the manuscript.
Musari-Martins Tomilola: Carried out the study, analysis of work, helped shape the research findings, provided feedback and wrote the manuscript.
Ezemelue Priscilla: Carried out the study, analysis of work, helped shape the research findings, provided feedback and wrote the manuscript.
Hebertson Ebiere: Supervised and reviewed the findings of the study, provided critical feedback and helped shape the research, analysis, and manuscript.
Ezechi Oliver: Supervised and reviewed the findings of the study, provided critical feedback and helped shape the research, analysis, and manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for the study was obtained from the NIMR Institutional Review Board and permission obtained from the management of the mission school.