
Abstract
Sterile pyuria is a common finding in pediatric patients. Literature describing the diagnoses as well as clinical characteristics of children with sterile pyuria is lacking. This review was performed to establish an evidence-based approach to the differential diagnosis by way of an extensive literature search. The definition of pyuria is inconsistent. The various causes of pediatric sterile pyuria identified were classified as either Infectious or Non-Infectious. Sub-categories of Infectious causes include: Viral Infection, Bacterial Infection, Other Infections (tuberculosis, fungal, parasitic), Sexually Transmitted Infections, Recent Antibiotic Therapy. Non-Infectious causes include: Systemic Disease, Renal Disease, Drug Related, Inflammation adjacent to Genitourinary Tract. Clinicians that encounter pediatric patients with sterile pyuria and persistent symptoms should consider the substantial differential diagnosis described in this study.
Background
“Sterile pyuria should not be taken as a sole diagnostic finding but rather it should be combined with other features to make a clinical sense of diagnostic possibilities.” Cunha. 1 Sterile pyuria is defined as pyuria without bacterial infection verified by a standard quantitative urine culture. Sterile pyuria in children has been described in both healthy patients and many pathological states. Sterile pyuria occurs in normal, asymptomatic school age children with a prevalence of 9.3% in females and 1% in males. 2
Multiple systemic searches were done with Google Scholar, PubMed, and Ovid data bases using the search terms, “sterile pyuria” and “sterile pyuria, pediatric.” Exclusion criteria included: adult studies (except where pediatric evidence is lacking), animal studies, written in a language other than English, case reports, commentaries, letters to the editor, editorials, abstracts, and those felt non-germane. The initial search in 2018 identified 1124 non-duplicate references that were reviewed for relevance by the author. Only 24 references from this search were included in the review, most without large numbers of patients being retrospective case series/case control in design. Additional studies were predominantly from the reference section of identified articles. Of note, 299 (26.6%) of the 1124 non-duplicate references dealt with some aspect of Kawasaki disease (KD).
There is only 1 previous publication specifically addressing the differential diagnosis of sterile pyuria, however in adults. 3 Pryles and Lustik 4 in 1971 offered a list of 9 possible etiologies for pediatric sterile pyuria in a review of laboratory diagnosis of urinary tract infection (UTI). These included: dehydration, trauma, irritating agents, chemical inflammation, renal tuberculosis (TB), acute glomerulonephritis, after oral polio vaccine (OPV), acute gastroenteritis and respiratory infections, and hyperchloremic renal acidosis. There have been other pediatric publications describing sterile pyuria in children but as a subset of different clinical scenarios. In 1994, Hoberman et al. 5 listed 59 patients with sterile pyuria in a study of pyuria and bacteriuria in febrile children less than 2 years old. No details other than the diagnoses were given. More recently in 2014 a series of adult and pediatric hospitalized patients were reported with sterile pyuria but again did not provide any details on the diagnostic nor clinical features other than a prevalence of 24% with sterile pyuria in the 66 pediatric patients. 6
Definition of Pyuria
To consider sterile pyuria, one must first define pyuria. It has been an evolving definition dependent primarily on the technology utilized. Traditionally the determination was made either with uncentrifuged urine, reported as white blood cells (WBC)/mm3, or centrifuged urine as WBC/high power field, as well as leukocyte esterase on dipstick. 7 Currently most hospitals are using automated microscopic urinalysis (UA) on unspun urine with computer-based recognition of cellular elements. Taking into account that the concentration of WBC reflect the balance between migration of WBC into the urinary system as related to the degree of inflammation and volume of urine, Chaudhari et al. 8 and Shaikh et al. 9 investigated the effect of urine concentration (specific gravity) on the optimal urine WBC threshold for the presumptive diagnosis of UTI using automated UA systems. They found a lower threshold for pyuria in dilute urine versus concentrated. Thresholds for pyuria with the various techniques are included in Table 1.
Definition of Pyuria.
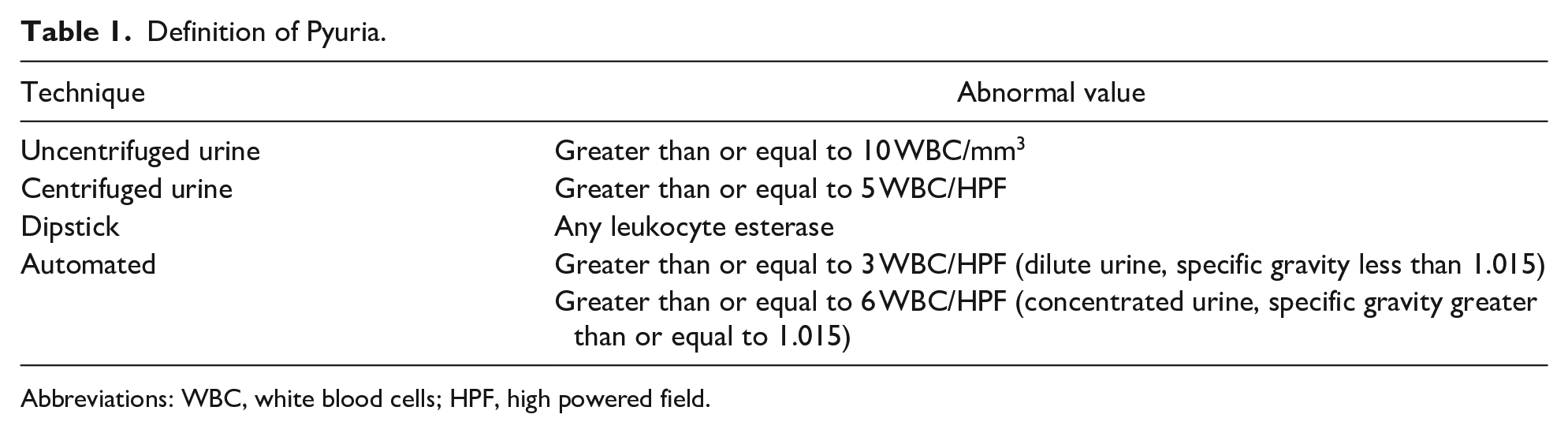
Abbreviations: WBC, white blood cells; HPF, high powered field.
Infectious Causes of Sterile Pyuria
Viral Infection
Infectious causes are a relatively common cause of sterile pyuria, see Table 2. The mechanism of the pyuria may be due to direct infection and/or a non-specific inflammatory cytokine response. Viral infection as a cause of sterile pyuria in children was first suggested by several reports in the 1960s. In 1961 a series of 41 patients with non-bacterial gastroenteritis were reported with 31.7% having sterile pyuria. 10 In 1965, Hart and Cherry 11 described 23 children who received OPV and showed a significant increase in polymorphonuclear cells in the urine on the 2nd to 13th day. More recently, 50 pediatric patients were reported with a positive polymerase chain reaction for human herpesvirus 6 (roseola), 34% of which had sterile pyuria. 12 Adenoviral infections, 13 enteroviral infections, 14 dengue fever, 15 and human immunodeficiency virus (HIV) infections 16 have also been associated with sterile pyuria in pediatric patients.
Infectious Causes of Sterile Pyuria in Childhood.

Source: Adapted from Dieter. 3
Bacterial Infection
There is less evidence for an association of sterile pyuria with bacterial infections. Wong et al. 17 reported a series of pediatric patients with leptospirosis. Sterile pyuria was present in 7 of the 9 patients. In a study of 36 pediatric patient with renal abscesses, 11% of patients with pyuria had negative urine cultures. 18 Other bacterial infections associated with sterile pyuria in childhood include: Lemierre’s syndrome, 19 tularemia, 20 brucellosis, 21 and anaerobic genitourinary infections. 22
Other Infections
Other infectious causes include TB, fungus, and parasites. Renal TB, although an established cause of extrapulmonary disease in adults, is rare in childhood. This is because renal TB is usually a late sign that does not appear for 3 to 10 years after the primary infection. In 2008, 17 pediatric patients were reported with genitourinary TB, sterile pyuria was found in 100%. 23 Carvalho et al. 24 found pyuria in 37% of 21 pediatric patients with funguria. Most of the cases had urinary tract abnormalities and/or prematurity. Ninety-seven percent grew Candida albicans from the urine. Urinary schistosomiasis is a common parasite in endemic areas of the world. In a study of 1600 school age children in Nigeria, 57.5% were positive for the ova of Schistosoma haematobium. All the patients had pyuria, 30.6% with sterile pyuria. 25
Sexually Transmitted Infections
Sexually transmitted infections (STI) are a frequent cause of sterile pyuria in adolescents. Huppert et al. 26 in 2009 reported 296 sexually active females, 14-22 years of age who presented to their emergency room or adolescent clinic. Twenty-four percent of symptomatic patients had sterile pyuria, 65% of which had STI, most commonly Trichomonas vaginalis or Neisseria gonorrhoeae. Shipman et al. 27 reported 1052 female adult and pediatric patients identified via a retrospective chart review with either Trichomonas vaginalis, Neisseria gonorrhoeae, and/or Chlamydia trachomatis. Thirty-seven percent had pyuria. Of these, 28% had sterile pyuria and 9.6% with UTI. Atypical bacteria including Mycoplasma hominis, Ureaplasma urealyticum, and Chlamydia trachomatis are also associated with sterile pyuria in children.28,29
Recent Antibiotic Therapy
A proposed mechanism for unexplained sterile pyuria is current or recent antibiotic therapy.3,30 In 1985, Millar and Langdale 31 utilized a simple microbiological method to identify antimicrobial agents in the urine. Of 1514 consecutive urine specimens received for culture, 302 (19.9%) contained antimicrobial activity. Smyth et al. 32 using a microtiter assay studied 527 clinical urine samples, adult and pediatric. In 63 patients <16 years old, the prevalence of inhibitory substances (antimicrobial activity) was 32%. Furthermore, an even higher prevalence of prior antibiotic usage, 46%, occurred in hospitalized patients. As the above studies suggest, some pediatric patients without an obvious source of sterile pyuria may have received recent antibiotic therapy not apparent or revealed to the clinician.
Possible Association of Sterile Pyuria and Fever
Sterile pyuria has previously been non-specifically attributed to fever. 33 Others have countered that if fever causes pyuria, the prevalence in males and females should be equal and the majority of febrile non-bacteriuric infants should have pyuria. Neither statement is valid.2,34
Non-Infectious Causes of Sterile Pyuria
Systemic Disease
The non-infectious causes of sterile pyuria in children are categorized in Table 3. Of the various systemic disease causes, KD is the most common in children. Sterile pyuria is a frequently reported feature of KD and is a supplemental laboratory criteria for the diagnosis. 35 Shike et al. 36 reported on 135 patients with KD, 83% with voided specimens and sterile pyuria was found in 79%. Pyuria in systemic lupus erythematosus (SLE) is frequent and often asymptomatic. It can occur with proteinuria and hematuria but also in isolation. Rahman et al. 37 found that 23% of 946 adult and pediatric patients with SLE had experienced at least 1 episode of sterile pyuria over the study period of 30 years. Sule et al. 38 reported on 47 pediatric patients with SLE. Isolated sterile pyuria along with low serum albumin was found to be predictive of future kidney involvement by longitudinal analysis. Sterile pyuria has also been noted in other polyarthritis syndromes in children including: reactive arthritis, juvenile idiopathic arthritis, polyarteritis nodosa and Henoch Schonlein purpura. 39 Adegoke and Adegun 40 in a study of asymptomatic bacteriuria in children with sickle cell anemia found a prevalence of 18.2% of sterile pyuria. This was thought to be due to repeated infarction and papillary necrosis. Toxic shock syndrome, 41 Sarcoidosis, 42 and hyperchloremic renal acidosis 43 have also been reported with sterile pyuria in children.
Non-Infectious Causes of Sterile Pyuria in Childhood.

Source: Adapted from Dieter. 3
Renal Disease
Renal conditions are a common cause of sterile pyuria. In chronic renal disease there is a question as to the relevance of pyuria. This has been studied in adult dialysis patients but not in pediatric patients. Vij et al. 44 showed the prevalence of pyuria in 97 adult dialysis patients was 51% and sterile pyuria in 31.6%. Pyuria by itself had too low a specificity and positive predictive value and therefore urine cultures recommended. In a study of 100 adult renal transplant candidates, 18% were found to have sterile pyuria. 45 In a series of pediatric patients, 35 with acute glomerulonephritis and 32 with nephrotic syndrome, the prevalence of sterile pyuria was 17.1% and 15.6% respectively. 46
Other renal diseases associated with sterile pyuria include nephrolithiasis/nephrocalcinosis, renal vein thrombosis, and hypercalciuria. In a series of 184 pediatric patients with urolithiasis, sterile pyuria was found in 18.5%. Unexplained sterile pyuria should raise the level of suspicion for nephrolithiasis or nephrocalcinosis, especially in the younger child. 47 In a series of 28 patients (adult and pediatric) with chronic renal vein thrombosis, 96% had sterile pyuria. 48 In a study of idiopathic hypercalciuria in 1984, 20% of fifteen pediatric patients had sterile pyuria, all with hematuria. 49
Instrumentation of the genitourinary tract by way of clean intermittent catheterization (CIC), indwelling catheters, and ureteral stents are all a source of pyuria. Forster et al. 50 studied 133 children who required CIC. Of the 111 patients designated as “non-UTI” (asymptomatic with a positive urine culture or those with a negative urine culture), 66% had pyuria. From the available data it was not possible to determine the prevalence of sterile pyuria although they stated, “Nearly all of the patients with a negative urine culture had pyuria.” They felt the basis of the pyuria seen in the patients without UTI was multifactorial due to chronic inflammation from repeated catheterization and the underlying etiology of their neurogenic bladder. Su et al. 51 reported 50 pediatric patients with neurogenic bladder, 25% with sterile pyuria. Pyuria was increased with a history of prior bladder surgery and catheterization. In contrast, indwelling urinary catheters usually have bacteriuria with pyuria, irrespective of symptoms, but also can have pyuria without bacteriuria for similar reasons as the above. 52 Ureteral stents have also been reported with sterile pyuria. In an adult study of 20 patients, pyuria was noted in 90%, 17% being sterile pyuria. 53
Drug Related
Complications of therapeutic drug administration can lead to sterile pyuria. Tubulointerstitial nephritis (TIN) in children is a frequent cause of acute kidney injury and can lead to chronic kidney disease. Implicated drugs were: antimicrobials, nonsteroidal anti-inflammatory drugs (NSAID), 54 diuretics, anticonvulsants, proton pump inhibitors, H-2 blockers, 55 etc. All can lead to hematuria, proteinuria, glucosuria as well as sterile pyuria. A renal biopsy is needed to confirm the diagnosis, therefore cases of drug, as well as, infectious induced TIN probably far exceed the reported numbers. 56 Drug induced (hemorrhagic) cystitis has also been associated with sterile pyuria, most commonly seen with cyclophosphamide, tiaprofenic acid, and other NSAID. 57
Inflammation Adjacent to Genitourinary Tract
Inflammation adjacent to the genitourinary tract can be caused from pathology of the appendix, adnexa, colon, or peritoneum and is a mechanism for sterile pyuria. Scott et al. 58 reported 50 pediatric patients with acute appendicitis. Pyuria was found in 18% of the patients with no mention of urine cultures. Fifty percent of these patients had a retrocecal or pelvic inflamed appendix, 40% with appendiceal perforation. Sterile pyuria has been also reported with pediatric ovarian torsion. 59 Pelvic inflammatory disease has been associated with sterile pyuria in adolescent patients. 26 McKinley et al. 60 reported on 20 adult patients with antibiotic-associated colitis, 30% with sterile pyuria. The etiology was not clear but was thought to be due to pelvic inflammation. Although it is likely that inflammatory bowel disease plays a role in this category, there was no evidence in the literature to justify inclusion.
Conclusion
Clinicians that encounter pediatric patients with sterile pyuria and persistent symptoms should consider the extensive differential diagnosis described in this review, see Tables 2 and 3. Important issues in sterile pyuria include undertreatment (ignoring the finding) and overtreatment (unnecessary antibiotics). Another consideration is the clinical relevance of sterile pyuria. Repeat urinalyses in a series of hospitalized adult and pediatric patients revealed resolution of pyuria in 50%. 6 Often the findings will be benign and self-limited, especially in the infectious category. In chronic renal disease it is almost expected. It is in the systemic, acute renal, and specifically the inflammation adjacent to the genitourinary tract group where patients will have persistent, unexplained symptoms, and sterile pyuria may be an important clue, worthy of a differential diagnosis. Having a commercially available screening test for antibiotic content in urine cultures would be helpful in identifying those patients with pre-treatment, possibly the most common cause of sterile pyuria in pediatric patients.31,32 Further studies of sterile pyuria involving prevalence data of the major diagnoses including a denominator for each, are indicated. This would allow estimates of disease probability and ultimately pre-test probability of the differential diagnosis. 61
Footnotes
Author Contributions
Dr. Bendig conceptualized and designed the study and drafted the entire manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.