
Abstract
Objective. To evaluate the burden of Contiguous Osteomyelitis (COM) in pediatric patients with cellulitis/abscess of hands/feet. Methods. Children aged 0-18 years, treated from 2009 to 2019 for cellulitis/abscess of hands/feet, who either had Magnetic Resonance Imaging at presentation, or Roentgenogram >10 days after symptom-onset, were included. Two-tailed T-test was used to compare patients with and without COM. P-value < .05 deemed statistically significant. Results. Twenty of forty-one patients with abscess/cellulitis of distal extremities were diagnosed with COM. Between groups, no differences identified in trauma-to-presentation time, antibiotic treatment for >48 hours before admission, abscess versus cellulitis, location of infection, presence of fever, or signs of infection. Conclusion. In our cohort, clinical presentation did not differentiate COM. Imaging helped diagnose patients with COM, who would otherwise receive a shorter antibiotic course. Hands/feet imaging in pediatric patients hospitalized with cellulitis/abscess should be considered to identify COM and customize treatment. Further research is warranted.
Introduction
In previously healthy children, most cases of osteomyelitis are hematogenous. 1 Non-hematogenous osteomyelitis can, however, occur as a result of contiguous spread of infection from soft tissue or via direct inoculation of infection into the bone from trauma, like bites or surgery. In the 2 previously reported cohorts of children with contiguous osteomyelitis,2,3 approximately 30% of patients had preceding minor trauma. Contiguous osteomyelitis in children is not studied in relation to soft tissue infection in distal extremities. We previously reported a case series of contiguous osteomyelitis in pediatric patients with soft tissue infection of hands or feet.4,5
Objective
To evaluate the burden and features of underlying osteomyelitis in hospitalized pediatric patients with cellulitis or abscess of hands or feet.
Hypothesis
Due to the close anatomical proximity of the tissue planes in hands and feet in children, there might be an increased risk of developing contiguous osteomyelitis during soft tissue infection at these anatomical sites.
Methods
Children, between the ages of 0 and 18 years, admitted to the Pediatric in-patient unit from 2009 to 2019, for treatment of cellulitis or abscess of the hands or feet were included in this retrospective pilot study, if they were evaluated with either a Magnetic Resonance Imaging (MRI) performed during admission, or a Roentgenogram (X-ray) of the affected area that was performed at least 10 days after onset of symptoms. Imaging was ordered based on the treating physician’s clinical judgment. Cases of contiguous osteomyelitis were defined based on imaging results. The MRI findings included both marrow signal hypointensity on T1-weighted images and marrow signal hyperintensity on T2-weighted images, with continuity of soft tissue abnormality. The X-ray findings included periosteal reaction, cortical erosion, or bone lucency.6-9 The variables in the 2 groups of subjects—with and without underlying contiguous osteomyelitis, were compared using a 2-tailed T-test. A P-value of <.05 was considered to be statistically significant.
Results
Twenty of forty-one patients (48.8%) were diagnosed with underlying contiguous osteomyelitis—16 by MRI, and 4 by late X-ray. Patients with osteomyelitis tended to be older (median age 15 years vs 10 years), and more often were male (80% vs 66.7%). Forty patients had preceding trauma. The most common trauma among those with osteomyelitis was contusion or crush injury (36.8%). Abrasion or laceration was the most common trauma among those without osteomyelitis (28.6%). The 2 groups of patients had no significant difference in the frequency of short (<5 days) trauma-to-presentation period (47.4% vs 52.4%, P 1.0); treatment with antibiotics for >48 hours prior to admission (21.0% vs 14.3%, P .7); presence of abscess versus cellulitis (P 1.0), or in the location of infection in the upper (55.0% vs 42.9%) or lower (45% vs 57.15%) extremity, P .5. With respect to clinical and laboratory findings, there was no significant difference between the 2 groups in presence of fever (15% vs 19%, P .5), elevated WBC count (15.8% vs 23.8%, P .7), elevated CRP (41.2% vs 9.1%, P .1), or bacteremia (6.2% vs 5%, P 1.0). Soft tissue infection of the wound with MRSA, tended to be more frequent among the patients without osteomyelitis (60% vs 27.3%, P .1), although not statistically significant as well. See Table 1.
Characteristics of the 41 Patients with Abscess/Cellulitis of the Hands or Feet.
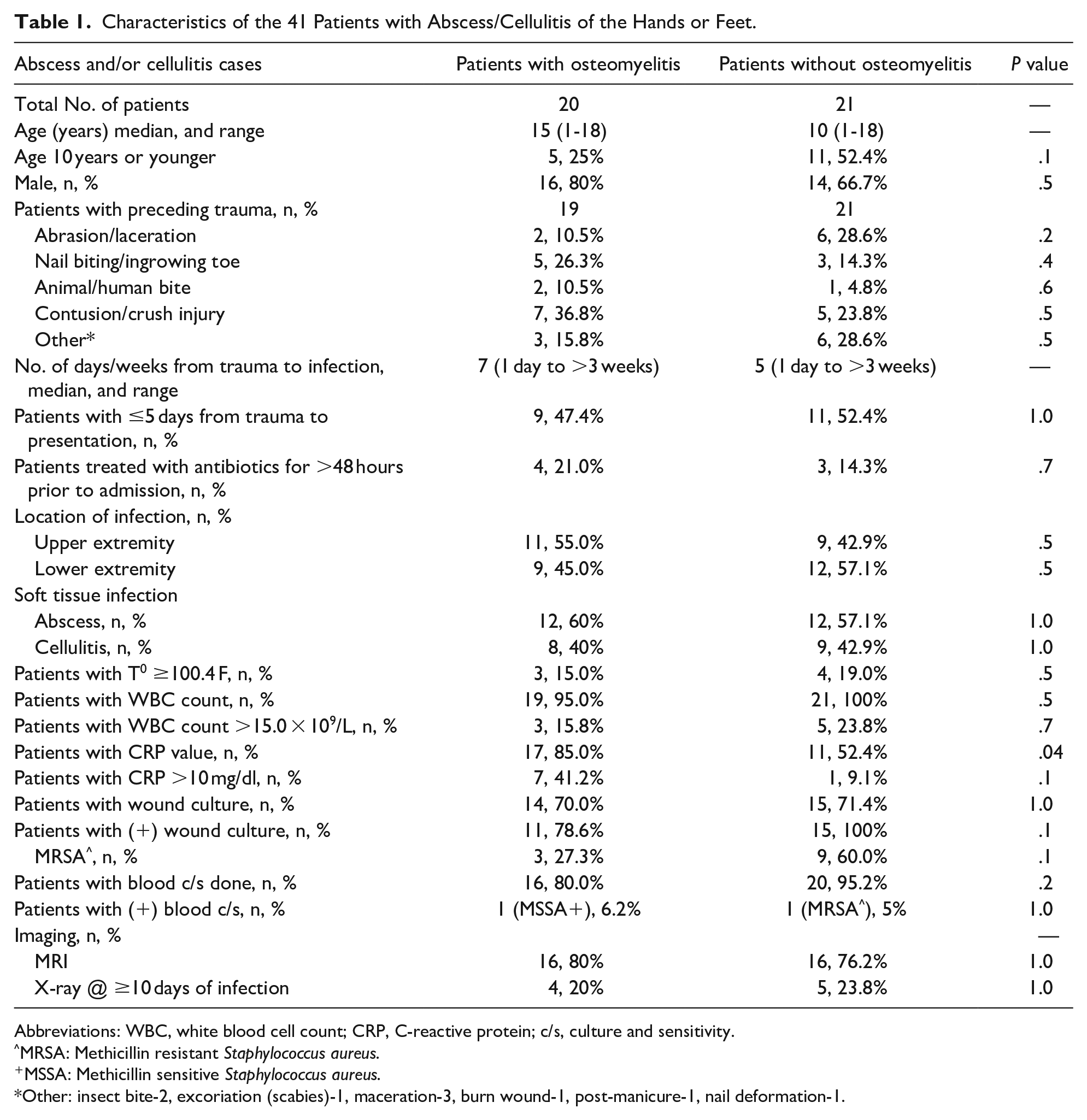
Abbreviations: WBC, white blood cell count; CRP, C-reactive protein; c/s, culture and sensitivity.
MRSA: Methicillin resistant Staphylococcus aureus.
MSSA: Methicillin sensitive Staphylococcus aureus.
Other: insect bite-2, excoriation (scabies)-1, maceration-3, burn wound-1, post-manicure-1, nail deformation-1.
In patients with osteomyelitis, the most common location of infection was in the phalanx bone (75%): 9 and 6 in the upper and lower extremity respectively. In the remainder of cases, 2 had an infection of the metacarpal bone and 3 had an infection of the metatarsal bone. See Table 2. In the group of patients with osteomyelitis, the most common causative organism was Staphylococcus aureus (N = 7, including 1 with bacteremia), followed by β hemolytic streptococci Group A and G (N = 3). In this group of subjects, the cultures also grew: Coagulase-negative Staphylococcus spp. (1), Streptococcus viridians (1), Gram-negative bacilli (2), and anaerobe (1). Mixed flora infection was identified in 41.7% of subjects with osteomyelitis. Interestingly, among those with osteomyelitis, Eikenella and Group G β hemolytic streptococci grew in a mixed wound culture from a patient with crush injury of the finger and Arcanobacterium grew in a culture from a nail biter with digital osteomyelitis. See Table 3. With regards to treatment, 12 out of the 20 patients with osteomyelitis were treated based on the antimicrobial sensitivities. The remaining 8 patients who had no positive culture, were treated with 5-7 days of empirical parenteral broad-spectrum antibiotics, followed by oral Cephalosporin and/or Clindamycin; with Fluoroquinolone (2 cases) or Linezolid (1 case), for the total duration of 3 - 4 weeks. 14 patients had surgical debridement. At follow up, all patients showed resolution of symptoms.
Location of Infection in Patients with Contiguous Osteomyelitis.

Causative Agents in 12 Patients with Contiguous Osteomyelitis of the Hand or Foot and Positive Wound or Blood Culture.

+MSSA - Methicillin Sensitive Staphylococcus aureus, ⋀MRSA - Methicillin Resistant Staphylococcus aureus.
GNB - Gram-Negative Bacilli.
CoNS - Coagulase negative Staphylococcus.
Includes one case of bacteremia with negative wound culture.
Includes one case of bacteremia with positive wound culture growing the same organism.
Discussion
Upon introduction of a pathogen into the soft tissue, it may spread along the path of least resistance, that is, along anatomical planes. Therefore, likely due to the close anatomical proximity of the bone, especially in the phalanges, sometimes there is a continuation of the soft tissue infection to the bone. 2 Also, preceding trauma in the distal extremity leading to osteomyelitis has been reported in the past. 10 Our study has demonstrated that in pediatric patients with significant soft tissue infection of distal extremities requiring hospitalization, in association with preceding trauma, even minimal, underlying contiguous osteomyelitis was detected by imaging in almost every other case.
In our small cohort, there was no difference in clinical presentation or laboratory findings which could tip towards identifying the presence or absence of underlying contiguous osteomyelitis. Our findings are concordant with previous reports on contiguous osteomyelitis: it was rarely associated with systemic symptoms or leukocytosis, and only less than half of the patients had elevated inflammatory markers.2,3,11
Though imaging is not a standard practice in managing cellulitis, 12 a physician’s decision to order imaging had enabled detection of osteomyelitis in 20 of our patients. It prompted the institution of an appropriate duration of treatment that prevented potential complications of undertreated osteomyelitis. 13
In our cohort of patients with contiguous osteomyelitis, 41.7% of wound cultures grew a mixture of microorganisms, which was consistent with previous reports on osteomyelitis by continuation.2,3,10,14 In concordance with 2 previous reports,2,3 among our group of subjects with contiguous osteomyelitis, the most common causative organism was Staphylococcus aureus. However, none of our subjects had Pseudomonas infection, which commonly causes contiguous osteomyelitis in children and adults.2,3,10,15-20 In the few cases of digital osteomyelitis, the causative organisms clearly represented oropharyngeal flora (like Arcanobacterium, Eikenella among others).
The limitations of this study are its small sample size and retrospective nature. Ordering imaging was just an arbitrary decision on behalf of the treating physician. A larger prospective study is necessary to establish a true incidence of contiguous osteomyelitis in hospitalized pediatric patients with cellulitis or abscess of hands or feet.
Conclusion
An association of the soft tissue infection of distal extremities with osteomyelitis of the underlying bone is a novel phenomenon not previously described in a pediatric cohort study. Currently, a physician should at least consider imaging when evaluating a patient with abscess/cellulitis of hands or feet. The finding of underlying bone involvement will guide the appropriate duration of treatment. Further research is warranted to formulate recommendations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
All work has been approved by the Lincoln Institutional Review Board and complies with the Journal of Ethical Consent.
File Number: IRB
PI: Yekaterina Sitnitskaya, MD
Protocol Title: Contiguous osteomyelitis of distal extremities in children
Continuing Approval effective from 12/20/2019 to 12/19/2020
Name of approving IRB: Lincoln Institutional Review Board, 234 E, 149st St, Bronx, NY 10451, USA.