
Abstract
Introduction. Adolescents (10-19 years) living with HIV (ALWH) face unique challenges in controlling HIV long-term, including stigma and perception of stigma within their communities. Methods. We conducted a qualitative investigation of the sources of perceived HIV-related stigma with ALWH in western Kenya. Forty-six ALWH on ART, aware of their status, and engaged in care were enrolled. Interviews explored perceived stigma by probing the individuals and experiences that adolescents identify as causing or perpetuating their ongoing fears. Results. Participants (54% male, mean age 17.4) reported ongoing fears of stigmatization related to friends and peers not living with HIV. They described previous enacted and first-hand observations of stigma, most often occurring in pre-adolescence, by age mates or peers at school as the most common cause for their ongoing fears. Conclusions. Perceived stigma is prevalent among ALWH and develops from experiences in pre-adolescence. Anti-HIV stigma interventions addressing educators and children in school settings to combat perceived stigma at its source should be investigated.
Introduction
Anti-HIV stigma is among the most complex and multi-dimensional factors impacting the continuum of HIV care and associated clinical outcomes for people living with HIV (PLWH). 1 Previous work to understand anti-HIV stigma has led to the development of the HIV Stigma Framework, which identifies enacted, anticipated and internalized stigma as 3 mechanisms affecting the HIV care cascade. 2 This framework has been validated for use in urban populations of PLWH in the US 3 and has been utilized in adult populations in Sweden. 4 Despite its lack of validation in low-and-middle-income countries (LMIC), previous research has used the HIV Stigma Framework to examine enacted, internalized, and anticipated stigma—commonly referred to as perceived stigma 5 —among adults living with HIV around the world.6,7 This work is critical, especially in LMIC, as demonstrated by a 2019 review that highlighted negative health-related stigma outcomes in these settings for “high-burden” diseases, including HIV. 8 However, neither the evaluation of stigma-related health outcomes, 8 nor qualitative examinations of anti-HIV stigma experiences, 9 have historically focused on the outcomes and perspectives of children and adolescents living with HIV (ALWH). 10 A recent systematic review of qualitative studies examining the experiences and attitudes of PLWH, where nearly half of all included studies assessed individuals’ perspectives on stigma, did not include a single study assessing this key population. 9
Worldwide, the WHO estimates that there are 2.2 million children living with HIV, 11 90% of whom reside within sub-Saharan Africa. 12 In Kenya, there are nearly 230 000 children and ALWH, only 61% of which are estimated to be on anti-retroviral therapy (ART).12,13 Importantly, ALWH represent the fastest-growing subgroup of PLWH, given both the increased incidence of new HIV infection within this age group and the growing number of perinatally-infected youth reaching adolescence and young adulthood. 14 Adolescence is a critical period of biological, psychological, and socioemotional development 15,16; for those living with HIV, this also requires significant development of autonomy and self-identification with their status.17,18 Moreover, ALWH must cope with an awareness of “difference” from their friends and peers that often leads to disruptions in their relationships with others. 19 These differences impact ALWH at a critical time in their development, especially as it relates to social cognition and their perception of others’ responses to their HIV status.20,21 Anti-HIV stigma and its perceived prevalence by ALWH, therefore, may play a significant role in their development and critically impact their long-term HIV clinical outcomes, including their persistent engagement with HIV care, their adherence to antiretroviral therapy (ART) and their subsequent viral suppression and survival.
Previous studies with PLWH have demonstrated that perceived stigma—defined as a persistent fear of stigmatization or discrimination 5 —negatively impacts their clinical outcomes.22,23 Studies have demonstrated that perceived stigma was associated with delayed initiation and presentation to HIV care and negative impacts on long-term retention in care and ART adherence.24-26 For many adults living with HIV, perceived stigma manifests as fear of accidental disclosure of their status and a secondary loss of resources. 27 Given that we know perceived stigma largely affects the interpersonal relationships of adults living with HIV and their care outcomes, it follows that perceived stigma would be a significant threat to achieving robust ART adherence for ALWH,28-32 who are already at significant risk for treatment failure, early mortality and morbidity.33-36
Therefore, a thorough exploration of perceived stigma and its impact on ALWH and their care outcomes is critically needed and should begin with understanding adolescents’ experiences with anti-HIV stigma. These experiences are difficult to measure or define given that there are few validated, quantitative tools for assessing stigma in this population 37 and no tools for qualitatively assessing perceived stigma specifically. 38 Previous work in this setting and other LMIC 16 has utilized cognitive interviewing techniques to identify a high prevalence of perceived stigma amongst parent-child dyads living with HIV, 39 but has not focused on the experiences of adolescents to ascertain the sources of their perceived stigma.
Our study sought to understand first-hand Kenyan adolescent experiences with stigma, how they understand the stigmatizing beliefs of others, and how these experiences impact their ongoing perception of stigma. Our goal is to learn from our participants’ perspectives in order to identify targets for anti-stigma interventions and demonstrate the importance of understanding the impact of perceived stigma on the care cascade for ALWH.
Methods
Study Design
We conducted a qualitative evaluation of the prevalence and sources of perceived stigma via semi-structured interviews with a sub-set of participants enrolled in the Adolescent Sentinel Cohort (ACE), a large study of ALWH established within the East Africa International Epidemiologic Databases Evaluating AIDS (EA-IeDEA) Consortium. The objective of the ACE study is to provide in-depth characterization of a cohort of perinatally infected adolescents both engaged in and disengaged from care, by describing HIV care-related characteristics, virologic outcomes and mental and behavioral health characteristics.
Study Participants and Setting
Participants were eligible for this study if they were adolescent aged 14 to 19 years at the time of their enrollment in the parent study, aware of their HIV status, on ART, and enrolled in care at 1 of 2 clinics affiliated with the Academic Model Providing Access to Healthcare (AMPATH) partnership in Western Kenya. AMPATH is a long-standing partnership between a consortium of North American academic medical centers, Moi University, and Moi Teaching and Referral Hospital (MTRH) in Eldoret, Kenya, which provides comprehensive HIV care for more than 160 000 individuals.40-42 Participants were recruited from 1 of 2 AMPATH facilities: the Rafiki Center at MTRH, an urban clinic that provides HIV care services for more than 850 children and adolescents, and the AMPATH Kitale Clinic, a peri-urban facility serving over 600 ALWH.
Data Collection and Analysis
Participants were identified through enrollment in the parent study through convenience sampling with equal representation from the 2 identified clinics. Participants were then contacted by research assistants to inform them of the study opportunity, and if interested, were scheduled to complete the interview during their next clinic visit. Participants provided informed consent to participate in a one-time, recorded interview. Interviews were conducted in both Kiswahili and English by research assistants trained in qualitative interview techniques. A private room was used in each clinic to conduct and record interviews via handheld device.
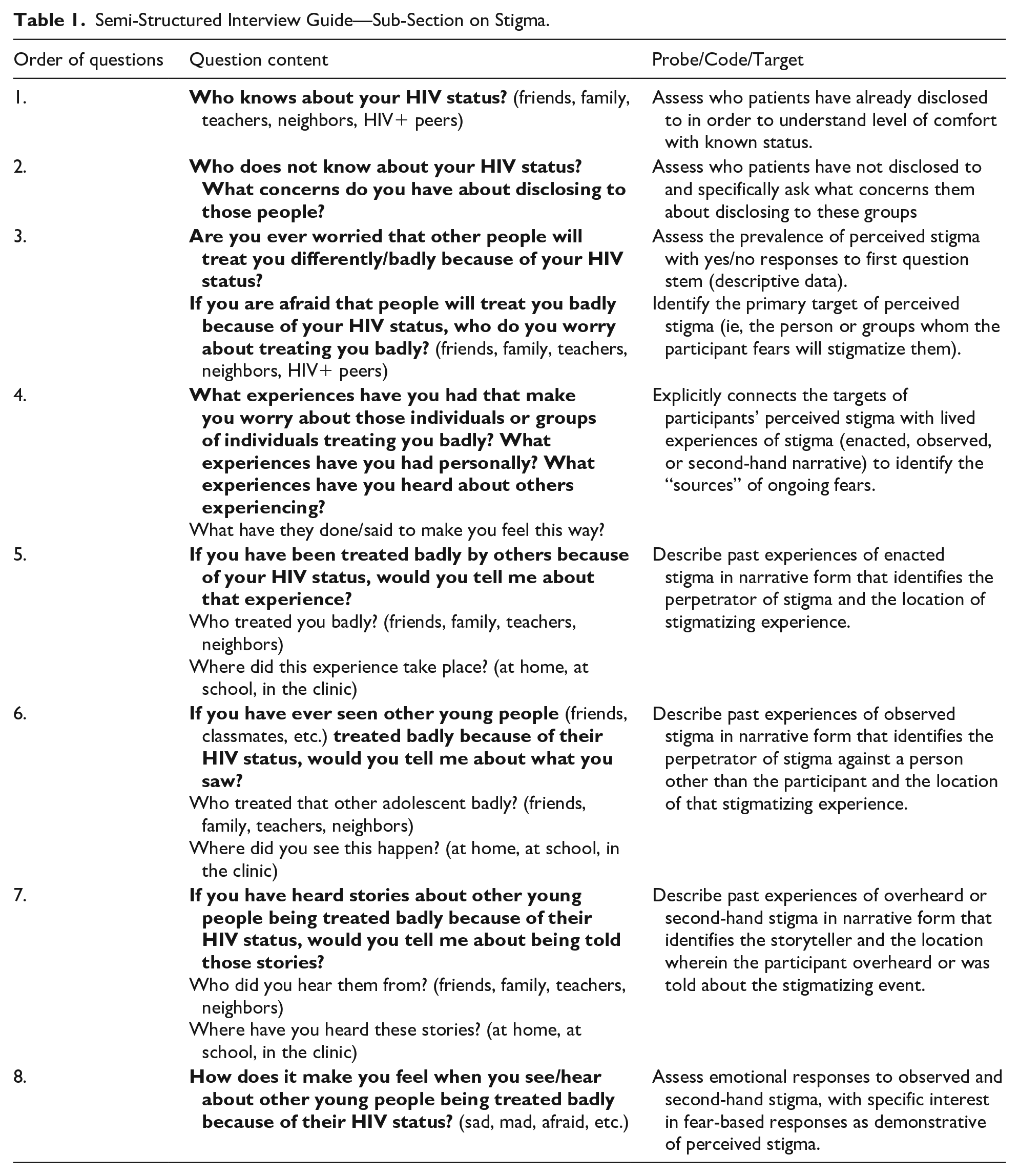
This study utilized cognitive interviewing techniques to assess adolescent sources of perceived stigma. Participants were asked explicit questions in a specific order in order to adequately frame their experiences with stigma. Table 1 includes the stigma-related interview questions in the order in which they were asked. This line of questioning allowed participants to first identify the targets of their ongoing fears of discrimination, in order to better understand the primary perceived perpetrators of that stigma. In this way, participants were primed with an emotional response (fear or worry) before being asked to recall specific previous experiences that caused the emotional response they just described.43-45 Therefore, participant experiences of stigma—either first-hand, observed, or overheard—were directly connected to their fears of stigmatization and discrimination. This emotional priming before memory acquisition identifies the source(s) of their perceived stigma.
Semi-Structured Interview Guide—Sub-Section on Stigma.
Interviews were translated into English (from Kiswahili), and transcribed for analysis. A system of manual, progressive coding of the transcripts using Dedoose software (Sociocultural Research Consultants, LLC) was utilized to identify emerging concepts. Thematic analysis was done through open coding by 2 researchers (GC and FS), involving line-by-line review of transcripts to identify meanings and processes. These researchers independently extracted and compared themes. Along with an additional analyst (AC), the research team reviewed transcripts several additional times to revise the coding structure as needed and compared and collapsed results based on consensus across the 3 analysts (GC, FS, AC). Axial coding, the process of relating categories to their subcategories and linking them together at the level of properties and dimensions, was used to organize the themes into their causal relationships. Hypotheses and concepts were developed inductively from the data. Quotes as presented here are excerpted directly from the English translations of the transcripts.
Ethical Approvals
This study was approved by the Indiana University School of Medicine’s Institutional Review Board, Indianapolis, Indiana, USA, and the Moi University / Moi Teaching and Referral Hospital’s Institutional Research and Ethics Committee in Eldoret, Kenya (approval number 0003338). All participants gave informed consent prior to enrollment in the study. Participants received a one-time reimbursement of 500ksh (5USD) for their time and participation in the study.
Results
Participant Demographics
We enrolled 46 participants in the study; 20 participants were recruited from the urban site, Rafiki Center, and the other 26 from the peri-urban site in Kitale. The majority (54.3%) of participants were male, with an average age of 17.4 years.
Adolescents identify sources of perceived stigma
Identified sources were initially defined by the groups or individuals whom participants described as being primarily responsible for informing their ongoing fears. Table 2 stratifies sources of perceived stigma based on the relationship between the participant and the identified source.
Participant Relationship to Sources of HIV-Related Perceived Stigma.

Adolescents describe experiences with HIV-related stigma
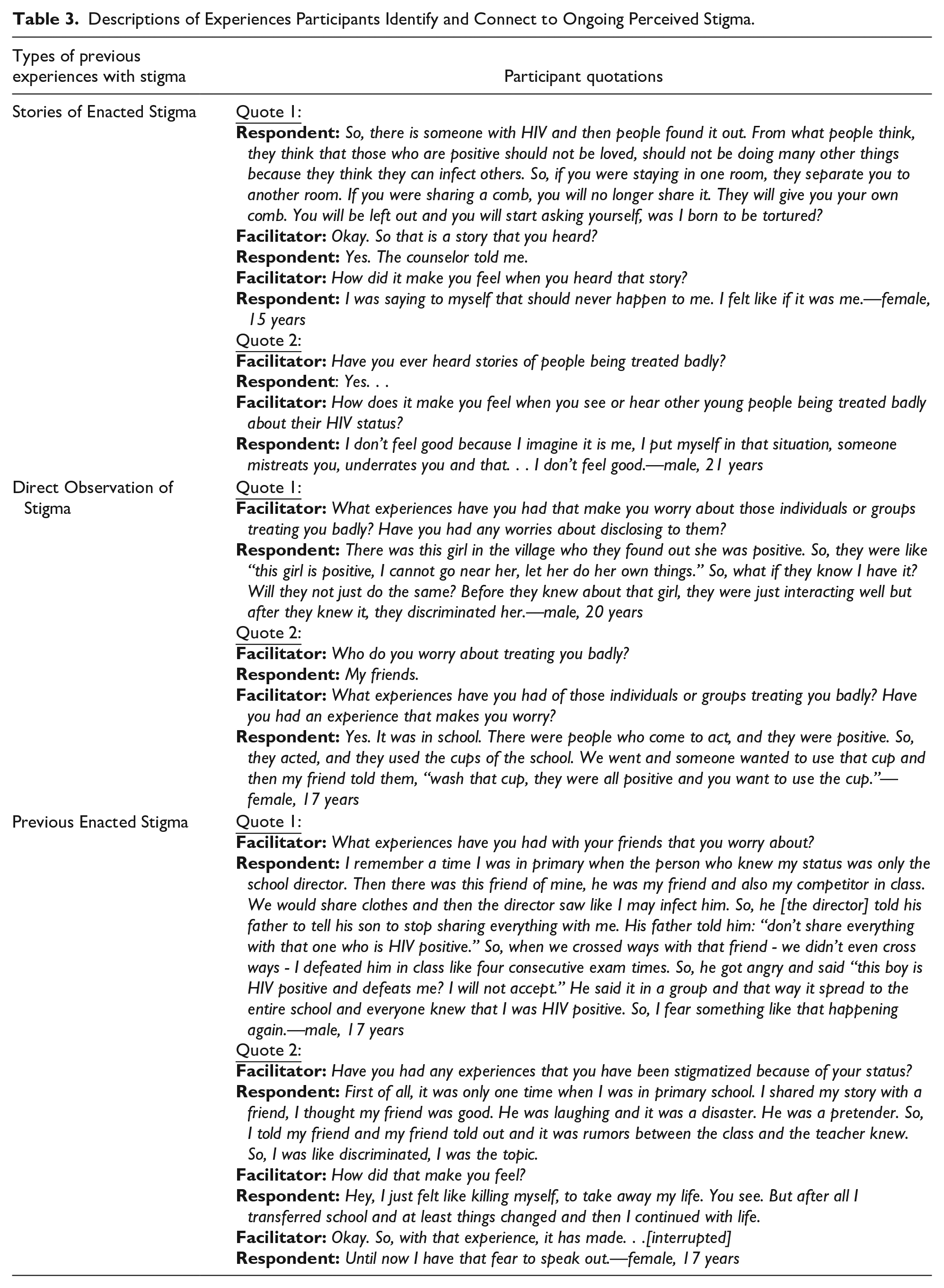
Once defined by the identity of perceived stigma’s informants, sources were then defined by specific experiences of anti-HIV stigma that inform participant fears. These experiences were divided into 3 categories: stories of stigma, observed stigma, and previously enacted stigma. These categorizations were made based on the relationship of the participant to the individual experiencing discrimination and are differentiated from one another based on the proximity of the participant to the specific discriminatory act. Table 3 includes descriptions of these experiences.
Descriptions of Experiences Participants Identify and Connect to Ongoing Perceived Stigma.
In this study, participants’ caregivers, their fellow ALWH, and their schoolmates were identified most often. While other individuals (schoolmates, peers, etc.) often contributed to more concrete experiences of discrimination, participants’ caregivers were associated with a more general sense of stigma’s prevalence—highlighted by quotations advising against HIV disclosure and the importance of secrecy to “protect” oneself from stigmatization. Importantly, these individuals inform participant fears through their words and actions but are not necessarily the perceived potential perpetrators of discrimination. Moreover, many of these individuals who contribute to participants’ perceived stigma continue to play ongoing, important roles in participants’ lives.
Participants frequently reported having previously heard stories of stigma occurring, with storytellers representing myriad areas of participants lives—from parents and friends to teachers and healthcare staff. These stories were most often primary accounts of previously enacted stigma that participants had heard from friends and peers living with HIV. Other times the stories were second-hand accounts shared by adults whose intentions cannot be known.
When asked about previously observed discrimination, participants most often identified their friends, schoolmates, and community/village peers as perpetrators of stigma. Respondents described discriminatory beliefs or actions that their peers had expressed or undertaken in their presence and directly connected those experiences to their own ongoing fear of disclosure and subsequent isolation from their school-based peers. It follows that participants were most often concerned with being stigmatized by their friends and schoolmates, and specifically concerned about being socially isolated because of their HIV status. In fact, schoolmates—largely believed by participants to be adolescents not living with HIV—were the most commonly reported group to act as both a source and as perceived perpetrators of stigma.
Finally, participants described their own experiences as the direct targets of enacted stigma. The most common form of enacted stigma our participants had experienced was vengeful or purposeful disclosure by their peers. Participants often described being young and socially close to the perpetrators of discrimination in their stories, which led to very deep emotional responses to being stigmatized. Moreover, participants readily connect these specific experiences with their ongoing fears of stigma and cite them as reasons for their purposeful non-disclosure as adolescents.
Discussion
HIV-related stigma remains a prominent source of fear and influence among ALWH. In order to differentiate sources of perceived stigma from the individuals whom participants perceive as potential perpetrators of stigma, we sought to facilitate the connection between ongoing fears of stigmatization and specific actions or experiences that inform those fears. Participants were primed to focus on the identities of perceived potential perpetrators before being asked to describe specific past experiences that made them “worry” about being stigmatized by these individuals or groups in the future.46,47 The dialog between the facilitator and the respondent in several quotations throughout Tables 2 and 3 demonstrates participants’ understanding of the relationship between these experiences and their enduring concerns. From this line of questioning, we extrapolate that the experiences participants cite are some of the most salient in relation to their ongoing perception of stigma and therefore function as the sources of their fear. 48
Our data demonstrate that for many ALWH, the fear of stigmatization based on one’s status is rooted in childhood experiences with anti-HIV stigma, often perpetrated by age mates and peers. These fears are then reinforced by observations of stigmatizing beliefs and discriminatory practices amongst their friends and schoolmates. Other times, they are reinforced by the stories these adolescents hear from their peers living with HIV and from trusted adults, including caregivers and educators. The relationship between individuals as sources of perceived stigma and as perceived potential perpetrators is complex. For example, participants frequently identified their caregivers’ perceptions of stigma to express how it informs their own fears of discrimination without identifying their caregivers as individuals whom they feared. On the other hand, participants often cited their schoolmates as perpetrators of anti-HIV stigma whose stigmatizing statements and discriminatory beliefs inform participant perceptions of the prevalence of stigma among this group and lead to very specific fears of vengeful disclosure and social isolation. 51 These findings are consistent with previous literature addressing the concerns of adults living with HIV, as well as parent-child dyads.39,52
Conclusions
Perceived stigma is a common issue affecting ALWH and may exacerbate existing mental health challenges for this group. Given the pervasiveness of ongoing fears of discrimination, it is critical to understand the way that these fears impact ALWH and their engagement in the HIV care cascade. Our data demonstrate how participants connect previous anti-HIV stigma with their understanding of themselves and their own HIV status—often highlighting how these experiences made them feel badly about themselves and worry about being stigmatized in the future. Therefore, anti-HIV stigma interventions remain a critical component of successful long-term HIV care for children and adolescents living with HIV49,50. Our results suggest that anti-stigma interventions meant to target the sources of perceived stigma should begin with primary school-aged children and not be delayed until adolescence. Furthermore, our participants identify the school environment as a critical setting for anti-HIV stigma interventions—particularly for faculty, staff, and students who perpetuate stigmatizing beliefs and discriminatory behaviors. Ongoing work with education stakeholders in this setting has demonstrated strong acceptability and desirability for anti-HIV stigma training and support for expansion of resources to local educators and other community groups. 53 Although not specifically probed, school-based anti-stigma interventions were suggested by several participants. One young woman, when asked how we should use the data collected in this study to better care for ALWH, plainly said: “You need to visit schools and teach these other students that we are not different from them.”
Limitations
There are several limitations to this study. The perspectives gathered in this study are from a specific population in western Kenya and may not be generalizable to other regions in SSA or resource-limited settings. Moreover, inclusion criteria for this study required adolescent to be between the ages of 14 and 19 at the time of enrollment in the parent study, which may limit generalizability to other age groups. Lastly, participants were recruited from 2 HIV clinics within the same care system (AMPATH). Despite adolescent services being differently organized at both sites, their affiliation with the same care system may limit their generalizability to other ALWH and their experiences, especially in more rural communities.
Footnotes
Acknowledgements
We thank the NIH-funded East Africa International epidemiology Databases to Evaluate AIDS Consortium (EA-IeDEA), U01 AIO699111, for providing access to its study cohort. Research reported in this publication was supported by the National Institute Of Allergy And Infectious Diseases (NIAID), Eunice Kennedy Shriver National Institute Of Child Health & Human Development (NICHD), National Institute On Drug Abuse (NIDA), National Cancer Institute (NCI), and the National Institute of Mental Health (NIMH), National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), Fogarty International Center (FIC), National Heart, Lung, and Blood Institute (NHLBI), in accordance with the regulatory requirements of the National Institutes of Health under Award Number U01AI069911East Africa IeDEA Consortium. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Contributions
Grant Callen and Rachel Vreeman led study design. Edith Apondi, Leslie Enane, Megan McHenry, and Kara Wools-Kaloustian contributed expert opinions to study design and implementation. Rachel Vreeman and Edith Apondi provided scientific oversight for the study. Material preparation, data collection, and analysis were performed by Grant Callen, Ashley Chory, Festus Sang, Dennis Munyoro, Josephine Aluoch. The first draft of the manuscript was written by Grant Callen and all authors reviewed and contributed to subsequent versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Fogarty International Center (FIC) of the National Institutes of Health and the Office of The Director, National Institutes of Health (OD) and the Office of Behavioral and Social Sciences Research (OBSSR) under grant#3D43TW009345-08S2 awarded to the Northern Pacific Global Health Fellows Program. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical Approval
This study was approved by the Indiana University School of Medicine’s Institutional Review Board, Indianapolis, Indiana, USA, and the Moi University/Moi Teaching and Referral Hospital’s Institutional Research and Ethics Committee in Eldoret, Kenya (approval number 0003338). All participants gave informed consent prior to enrollment in the study. Participants received a one-time reimbursement of 500ksh (5USD) for their time and participation in the study.
Consent to Participate and for Publication
Informed consent was obtained from all individual participants included in the study.