
Abstract
Patient referrals among health facilities are initiated to maximize receipt of quality care at a proper level within the health system. This study explored the processes, factors that influence, and strategies for referral of children from Ndirande Health Centre to Queen Elizabeth Central Hospital in Blantyre, Malawi. We drew a purposive sample comprising health care workers, mothers, fathers, ambulance drivers, and Health Center Advisory Committee (HCAC) members and held 19 in-depth interviews and 1 focus group discussion in August 2020. The referral process is influenced by the availability of motor and bicycle ambulances that are well equipped with medical equipment, delay in seeking health services, uptake of referral, and community support. Education and communication with the community and parents respectively optimize the process of referral. There is a need to improve the referral system of under-five children by instituting a policy that is functional while addressing the main barriers.
Background
The Malawian health system is 4-tiered and comprises community, primary, secondary, and tertiary levels of care and are connected by a well-established referral system.1,2 The division of the tiers is based on the type of care offered as well as the resources used at each level.1,2 Health care workers refer a patient from one level to the other and vice versa for further management, and a patient could then be referred to a lower level facility in the convalescent stage to continue with follow-up of care at that level. 3 Referral of patients has been defined as the processes by which professionals and institutions communicate and work together to protect, promote, and restore the health of an individual. 4 Referrals are initiated to maximize receipt of quality care at a proper level and guarantees continuity of care within the health system. 5 An effective referral system is facilitated in the presence of a close relationship among the existing levels of care in the health system while ensuring that people receive the best care from facilities closer to their homes.6,7 In addition, an effective health care referral system ensures that specialist care is accessed by those in need and also within the primary health care levels. 7
Referrals are common among pediatric cases and evidence suggests that between 6% and 20% of the children seeking help at primary level facilities in sub-Saharan African countries will require referral to a higher level. 8 Despite primary health care (PHC) facilities being the first platform for accessing health service, they remain under-resourced and under-equipped which necessitates referral to a higher level.9,10 Although Malawi has made steady progress in the reduction of the under-five mortality rate from 234 deaths/1000 births in 1992 to 63 deaths/1000 live births in 2015, 11 there remain gaps that can be closed if under-fives at primary level facilities received timely treatment and referral to facilities at a higher level. 12 Moreover, the fact that PHC facilities are resource-constrained contributes to the occurrence of pediatric deaths in the first 24 hours of admission.13,14 As such, timely referral provides the potential to avert mortality among children and lowers the severity of an illness.15,16
Barriers to the successful referral of sick children from the primary level of care to a referral hospital include distance and unavailability of transportation to take the child to the nearest hospital.17,18 The transportation factors coupled with stock-outs of essential drug and damaged vital equipment, makes it almost impossible to provide appropriate treatment and prevent deaths in very ill children at the primary care level.17,19,20 The lack of referral guidelines in the health facilities,19,21 and non-compliance to referral procedures by health workers 22 impedes the referral process and negatively affects the outcome of the illness. The factors that facilitate timely and appropriate referral include the competency levels of the health care workers at the primary level of care, 23 and timely availability of transport to transfer a sick child to the referral hospital.15,16,25 Furthermore, education on referral optimizes the quality of referral letters that health care works send out. 26 Caregivers compliance to the referral procedures also facilitates referral and results in a significant reduction in child morbidity and mortality. 17
An effective referral system is a key component in the management of pediatric cases in Malawi. 27 The guidelines for managing pediatric cases recommend an urgent referral for critical conditions or in circumstances where the referring facility does not have adequate resources to manage a patient. 27 There is a paucity of data in Malawi on the assessment of the pediatric referral system occurring across the different levels of care especially among facilities that are within the urban settings which are further compounded by the absence of referral guidelines and policy. Previous studies in Malawi have focused on primary health care facilities that are in rural settings and how different socio-economic, geographic locations, and decision-making power contribute to delayed health-seeking practices.28-30 Given the benefits of timely and effective referral of a child from a primary health care level facility to a higher one and the lack of data on the barriers, enablers, and processes of such in an urban facility in Malawi, this study explored the processes, barriers, and enablers that influence the referral of children from Ndirande Primary Health Centre to Queen Elizabeth Central Hospital in Blantyre, Malawi. Cognizant that half of the population in Blantyre are under the age of 15 years (NSO) and will likely use pediatric services in the primary health facilities 12 an understanding of the referral system will optimize the effectiveness of the system to achieve timely referral which can avert mortality.
Methods
Study Design
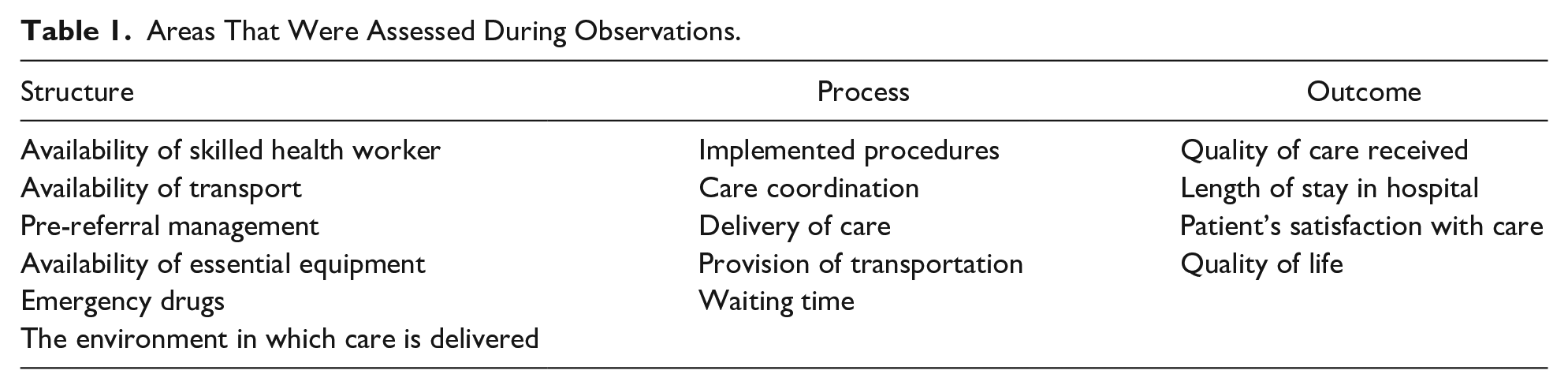
This was a qualitative descriptive study conducted at Ndirande Health Centre in urban Blantyre in August 2020. The design enabled the description of experiences with the referral of children under the age of 5 from health workers in the out-patient department (OPD) or under-five clinic, ambulance drivers, health advisory committee members, and caretakers. The study used face-to-face in-depth interviews (IDIs) and focus group discussions (FGDs). We also employed quality improvement approaches and guided by the Donabedian model on quality 31 to describe the process of referral at the facility. The Donabedian model has 3 components that are used to assess the quality of care and these include structure, process, and outcome. The model asserts that the structural components affect the process measures which later affect the outcome measures. The structural components are inputs and encompass human resources, staff ratios, and operating times of the service. Process measures reflect the way a facility’s systems and processes interact to deliver the expected outcome while outcome measures comprise the results that one gets after rendering a service such as a reduction in mortality and morbidity. 31 The description of the process entailed following 2 mothers and 2 fathers whose children were referred to QECH to understand how referral of under-five children is done at this facility.
Study Setting
Ndirande Health Centre is one of the urban health centers which operates under the Blantyre District Health Office. It has a catchment area of 143 187. 32 The services offered at this facility include Integrated Maternal and Child Health Services and Outpatient Department Services. In a day, it serves 500 patients and 80 under-five children in the out-patient department (OPD) and under-five clinic respectively. The facility has the following departments; laboratory, an antenatal clinic, outpatient department, short stay department for pre-referral case management, pharmacy, maternity, and ART department. Malaria, Pneumonia, and diarrhea are the common childhood illnesses reported at this facility. The referral hospital for this health center is Queen Elizabeth Central Hospital (QECH) which is 5 km away. The facility has 79 trained medical personnel and they include 2 Medical Officers, 7 Clinical Officers, 25 Nurses, 8 Medical Assistants, 1 Environmental Health Officer, 23 Health Surveillance Assistants (HSAs), 6 HIV Diagnostic Assistants (HDAs), 2 Health Management Information System Officers, 4 Laboratory Technicians, 1 Dental Therapist. The facility has 20 support staff who are Clerks, Patient Attendants, and Cleaners. The drivers are based at a central point which is the Blantyre District Health Office. We selected this facility because it refers a substantial number of under-five children to QECH. Of note, the facility lacks a residential ambulance such that when there is a patient at Ndirande Health Centre who needs a referral, an ambulance is called from Blantyre District Health Offices which is 5 km away from the facility.
Sampling and Selection of Participants
Participants were purposively selected with an aspect of maximum variation, 33 and we included health workers in Out Patient Department (OPD) and under-five clinics, caretakers whose children have been referred and used an ambulance, those who used their transport, and those who did not take up referral, ambulance drivers, and Health Centre Advisory Committee (HCAC) members involved in the referral of under-five children. HCACs are formally constituted under Malawi’s Health Sector Strategic Plan II. 10 The HCAC is considered an important stakeholder in the local governance of health services. They monitor the performance of health workers in their communities, in addition to assisting communities to demand the quantity and quality of services needed. 34 We selected health workers who were willing to participate in the study, were able to give informed consent, and were working in the under-five area, and included different cadres. We selected caretakers with a child who was not critically ill, willing to participate, and able to give informed consent. 35
Data Collection and Management
We conducted 1 focused group discussion among HCAC members and 19 interviews involving clinicians, nurses, drivers, mothers, and fathers. Two mothers and 1 nurse refused to participate in the study because of time constraints. Interviews and FGD guides were used to collect data from different categories of the participant. We had separate interview guides for health workers, caregivers, and ambulance drivers. All data were collected face-to-face and in Chichewa, the local language by WK and TU, We probed for more information where necessary, the researchers clarified the questions to obtain relevant information. All sessions were digitally recorded and we also captured field notes that included key findings to help with summarizing at the end of the interview for member checking purposes. 36 The average interview time was 30 minutes.
Donabedian Model
Using the Donabedian quality of care model, we assessed 3 aspects of the quality of referral care offered at the facility: structure, process, and outcome. Table 1 shows variables of interest.
Areas That Were Assessed During Observations.
Data Analysis
Data were transcribed verbatim and then translated into English by the investigators. 37 All study documents were kept in a lockable cabinet and digital ones were protected with a password as a guarantee for confidentiality. The anonymity of the participant’s identity was observed by the use of codes instead of names. We employed a thematic approach to analyze the data. Following data transcription, the researchers read and re-read each transcript to familiarize themselves with the whole body of data and they compared the transcripts to deduce and induce similar ideas and come up with a coding framework. Initial codes were generated through an inductive method which takes shape of the data and the deductive method which focuses on the objectives. Then, similar codes were collated and organized into meaningful categories and themes in tandem with the Donabedian model of quality. The generated themes were revised for completeness and overlap to ensure independence.36,37
Ethical Considerations
The research received ethics review and approval from the College of Medicine Research Ethics Committee (COMREC-Number: U2893). Institutional approval to conduct the study at Ndirande Health Centre was obtained from the Director of Health and Social Services in Blantyre. Participants voluntarily signed informed consent forms before they participated in the study. Each participant provided written consent after reading the informed consent form. Participation in the study is voluntary and that they could withdraw their participation at any point without repercussions. All participants were literate.
Results
Demographic Data of Study Participants
A total of 19 in-depth interviews were conducted, these were among health workers, caregivers (fathers and mothers), and ambulance drivers. One focused group discussion was conducted among 6 HCAC members (chairperson, secretary, treasurer, counselor, and 2 members). The age range of the caretakers who were interviewed ranged between 17 and 35 years. All health workers who were interviewed had experience with the referral of patients, the duration of experience ranged from 4 months to 3 years. The respondents of the in-depth interviews included 3 clinicians, 2 nurses, 6 mothers, 4 fathers, and 3 ambulance drivers.
Current Referral Systems Among Under-Five Children
According to this study, the current referral of under-five children begins from the community, where an HSA at the Village Clinic, using Emergency Triage Assessment and Treatment (ETAT), identifies a child presenting with danger signs. Such children are given an initial treatment before they are referred to a health center for further assessment and treatment, for example, rectal artesunate is administered in case of severe malaria. If the condition does not improve at the health center, the clinician who assessed the child calls for an ambulance and refers the child to a higher level facility like Queen Elizabeth Central Hospital (QECH). However, the system is compromised because of inadequate emergency equipment like oxygen cylinders, drugs, and medical supplies, lack of proper transport facilities such as standardized ambulances, including trio cycles and motorcycle ambulances in the community.
Factors and Strategies Influencing Referral Among Children
The factors that influence and strategies for optimizing referral encompassed both structural and process components of the Donabedian model intending to improve the outcomes of the process. These are discussed under the overarching themes deduced from the Donabedian model of quality.
Structural Factors and Strategies in the Referral Process
This theme covers the structural factors that influence and strategies for improving the process of referral among under-five children.
Actors in and resources for referral
According to caregivers, mothers were the primary caretakers of the children and were responsible for all their needs. When asked how they know that their child is sick, some caregivers cited:
“I usually know when she is just crying but also when she is refusing to eat.” Mother 1
“Most of the time it is the mother who says that the child is sick because she is the one who is always with the child. As today it is her mother who said the child is sick but I have come with it because the mother has just delivered.”Father1
Our observations highlighted other actors in the structural components of referral and noted the following inputs: The facility had inadequate emergency medical supplies and equipment and standardized ambulances. The facility did not have a stationed ambulance to necessitate timely referral and quality of care of under-five children instead they asked for 1 from the Blantyre District Hospital when they needed 1. The ambulance which the facility used to transfer sick children to QECH lacked emergency equipment such as oxygen concentrators, siren, and beckons, and of note, there was no care provided whilst in transit to the main hospital. Additionally, of the 4 children who were followed from Ndirande Health Centre to QECH, 2 used an ambulance from Blantyre DHO as means of transport and reached QECH after 2 hours from the time referral was initiated. The other 2 found their means of transport as the ambulance delayed and it took them 8 hours.
Structural factors that influence the referral of under-five children
The unavailability of resources triggered the need for a referral of under-five children in this study. It was revealed that most of the referrals that are done at the facility are due to the unavailability of or inadequate resources such as medications and oxygen cylinders at the facility. One health care worker and a guardian narrated “Lack of medications, we sometimes don’t have drugs to give these children so we refer a child due to lack of medication.”—Nurse1 “I think the problem is having no drugs at the facility to treat other children.” Father3
The study revealed that the availability of a functional transportation facility with emergency equipment makes it easier to refer children to a higher level facility on time for further management. This further encourages caretakers to make decisions to go to the referral hospital. However, using the Donabedian model, it was found that the health facility did not have a stationed ambulance, they used 1 from DHO and it was not fully equipped, as it lacked sirens and oxygen concentrators, the only thing that was available in the ambulance was a mattress for the patient.
“As I have already said that it depends on the availability of transport because we do not have a static ambulance here we depend on DHO ambulance. When an ambulance is called and they say it has gone to other places then, that child will delay unless if they can manage to find their means of transport. But when an ambulance is called and it comes immediately then that child will reach referral site on time.”—DR3
In other instances, the available ambulances are rarely in good condition and lack basic requirements like a siren that is used to signal the need for access while on the road and also announcing arrival at the other facility to highlight an emergency.
“As of now (pause) other ambulances are not in good working condition because they have overstayed and have been over-working being forced to work while they need to be maintained. Most of the time there is delayed maintenance. Most of these ambulances don’t have sirens and beckons only new ambulances to have these things.”—DR2
The absence of a resident ambulance entails that the caretakers are sometimes advised to find their means of transport especially if the health workers know that it will be a while before an ambulance is available “I have been told that transport has gone to Madziabango so I have to find my transport. I cannot wait for an ambulance because it will take time.”—Mother4
“The causes could be lack of transport. Most of the time the community is poor so whenever there is no ambulance the child delays in reaching the referral facility to receive treatment as is required. Clinicians can also be blamed for negligence. We need to assess whether the child needs to be referred or should go home. We need to do a full assessment.” DR2
Furthermore, distance to the health facility influenced referral. Participants admitted that for a successful referral, there must be geographical access to referral care facilities, long distances to health facilities were mentioned as a setback to referral. Participants bemoaned the higher costs in transport.
“I think the other thing is that I stay far from the facility so I can delay reaching the facility.”—Father 1 “I use a motorcycle to reach here, so, it is far, we pay k1000 from home to here.”—Mother 4
Structural Strategies for Optimizing the Referral Process
Participants highlighted that presence of a designated ambulance for the facility would promote timely referral. They stated that timely referral would be easier because the facility would be able to control and decide when to send the ambulance at the time they need to. It was recommended that ambulances should be maintained in good condition and have all necessary supplies within them if a referral has to be effective and timely.
“Government hospitals should have enough ambulances, the ambulances should be in good working condition, the drivers should be enough, fuel should always be available, there should be good communication (health centers and referral hospitals should communicate properly) but also it could be good if each health center has its ambulance.” Volunteer 2
Participants were aware that currently, it is the DHO who has the authority of assigning ambulances and acknowledged that ambulances are at times used for other activities than transporting patients.
“I think the allocation of ambulances is there but because at DHO if you go outside you will see that there are many ambulances, other activities at the office are being done using the same ambulances, so if there were other vehicles that could be used to use for office work and ambulances should be used specifically for patients that could be better.” Driver 1
Participants recommended the resumption of bicycle ambulances in the communities as a measure of accelerating timely referrals from the communities.
“As they used to do earlier they should provide us with a bicycle ambulance because it is useful when there is no ambulance. Even Machira (man-made stretcher) our men can run with them and the community can be assisted.” Volunteer 3
Process Factors and Strategies in the Referral Process
Actors in the process of referral
Participants stated that the one who has noticed that a child is sick or sources transport is the one who makes decisions to take a sick child to the hospital. In most cases, a husband is the one who finances the costs associated with the hospital hence decides on visiting the facility or taking up the referral.
“I am the one who decided to come to the hospital because I realized that the child is sick. Last time it was the father who came with her and I was just called when she was referred. So whoever sees that the child is sick decides.”—Mother2 “My husband is the one who decides because it is he who sources transport. I do not do any business so I depend on my husband.”—Mother1
At the facility level, it is the health care worker who assessed the child that decides to refer or not, sometimes referral decisions are made due to drugs stock out.
“Most of the time it is the clinician who was assessing the child who decides to refer a child.” Nurse 2
Factors That Influence the Process of Referral of Under-Fives
Delay in seeking medical help by parents or guardians may contribute to the deterioration of a child’s condition which triggers a referral. The health workers implied that if health services were sought in time, referral “Most of the time I think a person is not always prepared that the child will be sick. Maybe you were doing other things before the Childs got sick so you may think of finishing what you were doing before taking the child to the hospital.”Mother1
“The problem that we find in the community is that when parents see that the child is sick, they say they will go to the hospital later in the day. When it is evening it is when you see them put the child at the back and go with it to the hospital but the Child’s illness started in the morning.” Volunteer1
Parents’ response or reaction when a child has been referred to a higher facility plays a role in the success or failure of referral. This study revealed that most parents or guardians had positively responded to the news, 2 guardians narrated; “I will go, this is the only child that I have, I want him to get well.” Father 3 “It is painful because when you come to the hospital you believe that you will be assisted. Going to another facility is expensive. However I understand that the doctors have seen a need for me to go to queens with my child, I will go because I have been told to go so that my child can receive the required treatment they are saying.” Mother 1
However, some participants cited that other people do not take up referrals; “Three-quarters of the parents accept referral but there are a few who do not take up a referral.”Volunteer1 “The Apostolic faith people are the ones who are giving us problems, they say they don’t go to the hospital] they care for their patients in a tabernacle. I remember some time ago the health workers after we informed them that the (apostolic) are keeping a very sick man who had cholera in a tabernacle they went and brought that person to the hospital and that man is alive today but other people have died there because of their faith. That is how it is.” Volunteer 2
Study participants mentioned that the community plays an important role in the referral of under-five children by supporting one another in terms of transportation, as well as psychological support.
“As they have already said they help each other with transport even when the child has been referred and an ambulance is not available they assist each other.”Volunteer1
“They escort each other; you see a group of villagers coming with a sick child even carrying a child for their friend. You see even those that have the potential to help with transport if a friend cannot afford it. They hire a vehicle or a taxi.”Nurse1
Strategies for Optimizing the Process of Referral Among Under-Fives
Participants recommended that communities should be educated on the importance of timely referral so that they heed if referred. This will promote timely decision making and positive perception toward referral.
“Civic education- teaching people can assist. For example, people used to deliver at the TBAs but through civic education, they are now coming to the hospital to deliver.” Volunteer 1
“Most of the times when these children come at under-five we have health talk, we choose a topic like Malaria, signs of malaria and dangers of malaria or else diarrhea. Through health talk when they go home these people tell each other.” Driver 2
Participants recommended that there should be effective communication between health facilities regarding referral activities as poor communication contributes to the delay of patient transfer as the ambulance tended to come late.
“Good communication between health centers and referral hospitals such that the drivers should come quickly when an ambulance has been called. Ambulances should be close to the health centers for example cluster facilities should have one ambulance.” Driver 2
Outcome-Related Factors in the Referral Process
Perceived adverse events of untimely referral trigger referral of under-five children at the health facility. Health workers reported that under-five children are at risk of developing serious complications and dying if the referral system is compromised. The quest to have a positive outcome triggers a health care worker to initiate the referral process.
“My thinking is that they might develop other problems which were not there when they were coming. They can also die while waiting for an ambulance. They can also die on the way to the hospital because of the way I have seen the ambulances most of them don’t have emergency equipment. That is all I can say.” Nurse1
“I think they are at risk of developing anemia for example if the child is suffering from malaria when they delay in treating them could develop anemia. I think they could die prematurely since they are not treated as quickly as it is needed.” Nurse2
Participants stated that a good previous experience following referral influences caretakers to adhere to and take up a referral, unlike when the experience was bad.
“I feel very bad because of the bad experience that I had last time when I was referred with this child. I reached the hospital at night and for me to be assisted it took time”—Mother 2. “She said she was lucky because when she arrived at the hospital she met a friend who assisted her to see a doctor quickly.” Father 2
Health care works corroborated the other participant’s responses and stated that their previous experience also helps them decide whether to refer a client or not depending on the condition of the child and availability of resources.
“We start by assessing the child than the way we have seen the child it is when we decide whether we should refer or we should not refer but assist the child at this facility. We have the experiences that first we assess the child whether she needs to be treated at this facility or else the child has to be referred.”Dr1
Discussion
This study explored the processes, factors that influence, and strategies for referral of children from Ndirande Health Centre to Queen Elizabeth Central Hospital in Blantyre, Malawi. The factors that influenced and strategies for optimizing referral are classified under the tenets of the Donabedian model of quality and these include structural, process, and outcomes aspects. The structural factors included the availability of resources like ambulances that are well equipped with medical equipment for use while in transit, the resumption of bicycle ambulances. The process factors that influence referral include the delay in seeking health services by parents of sick children, the uptake of referral, and community support while education and communication with the community and parents respectively optimize the process of referral. The quest for positive outcomes and a positive previous experience with referral facilitates the referral process. There is an interaction between the structures and processes as asserted by Donabedian to yield a better outcome of the referral.
The majority of the participants are aware of factors influencing referral of under-five children which cements earlier findings that revealed that health workers knew challenges with referral.15,23 This implies that if the known factors are addressed then implementation of an effective referral system would be possible. Implementation of an effective referral system is critical as it has the potential to minimize rates of mortality among children particularly those that occur in the first 24 hours following admission.13,14 Evidence suggests that the lack of logistical support delays referral processes which has the potential of delayed receipt of appropriate care 40 and exposes the fragility of the referral system which threatens the reduction of mortality rates.38,39
Our findings that the unavailability of resources triggers a referral is consistent with earlier findings in Malawi and other settings that showed that shortage of health workers, lack of essential equipment, and medicine stock-outs influences referrals.17,28,41 This may mean that some of the cases being referred could have been managed at the primary facility if resources were available while the act of referral, in this case, burdens the next level of care unnecessarily. 40 The lack of resources like diagnostic equipment, drugs, health care workers, in health services is a major problem across several LMICs.20,42,43 An analysis on the availability of drugs in Malawi showed that there are fewer drugs in public facilities when compared with private and faith-based facilities and there were more drugs available for adults than there were for pediatric cases 44 which may lead to more referrals among the pediatric patients. Of the drugs available antimalarial, were commonly available compared to antibiotics 44 and this is likely to lead to unnecessary referrals to allow the children to access medications.
Our study showed that referral is initiated to avert a negative health outcome that may occur if there is a delay in referring a child for advanced care which is consistent with guidelines for the management of childhood illnesses. 27 Previous research reported that health care workers refer seriously ill children the most 41 and this may result in delayed referral of other children that are not in a serious condition which may deteriorate their health. Health care workers in our study make efforts to provide pre-referral treatment within the facility before referring the patient for further management which is consistent with previous studies where health workers administered artesunate and paracetamol before referring a patient.45,46 On the contrary, the administration of pre-referral treatment has to be accompanied by counseling that emphasizes the temporal relief it offers and the need for caregivers to comply with the referral process for the child to access comprehensive care. 46 Similarly, our findings that caretakers support the referral process to avert negative health outcomes by sourcing transportation cement what was earlier observed in another study in Malawi where caregivers sought taxis, public transport to get a patient to the hospital and would go by foot if they cannot afford the other means. 47 Notably, caregivers heed referral protocol once they understand the severity of the condition of their child to prevent adverse outcomes. 46
Our findings that the condition of a child deteriorates when medical care is sought late were reported earlier in a Peruvian study where it was noted that parents or caregivers that delayed in reporting to a health facility with their children diagnosed with pneumonia resulted in presenting at the facility with a child with severe symptoms. 48 In other instances, the cause of the delay could be an administration of over-the-counter drugs by the parents or guardians and would only report to the health facility when the condition worsens. 49
Despite the ability of a mother to recognize when her child is sick, she sometimes fails to seek medical care timely because she would be dependent on her partner for costs associated with the visitor referral. This finding resonates with previous studies conducted in Malawi, Uganda, and Nigeria that revealed that mothers delayed in seeking medical attention for their infants because they had to wait for permission and financial support from their partners.26,47,48 We recommend continued counseling on immediate uptake of referral protocols for Malawi to sustain the gains in the reduction of infant mortality rates. Our findings that mothers were able to recognize when a child is sick are different from another Malawian study that showed that guardians were unable to quickly recognize symptoms or they had perceived the illness as not severe. 28 The same perception was observed in studies in Uganda and Gambia where caretakers delayed in seeking treatment because some had rated the illness as mild and others were practicing home treatment.47,49 The difference in the ability to recognize whether a child is sick could be explained because of the differences in settings of the study and the occupational status of caregivers. Our study was conducted in an urban setting where most people are literate unlike in the rural areas where the other studies were based.
Our findings on the lack of a designated ambulance at the facility resonate with findings from a Tanzanian study where women were advised to find their means of transportation.1,50 Similarly, a study done in Afghanistan on compliance with referral in sick children found that children who were referred used a different mode of transportation; some walked because the referral facility was proximal to where they stay, while others used hospital ambulance and others paid for vehicles as means of transport since the referring facility did not provide transport.18,23 The lack of transport remains a deterrent to the uptake of referrals.29,51 Although bicycle ambulances offer a solution to this problem as stated in this study and previous studies, they are more ideal for rural facilities,25,30 because they may not be easier to maneuver in a city considering the high traffic.
The lack of optimal equipment in the ambulances as stated in our study is consistent with findings from previous studies that reported that ambulances were not used because they were few and at times would lack fuel.1,50 Evidence suggests that proximity to health facilities influences compliance with the referral process as was stated in this study.17,18,23,24,52,53 One area that may be strengthened in Malawi, cognizant of the limited facilities within reach of people in the implementation of community case management (CCM) by health surveillance assistants (HSAs) at the community level which has increased geographic access for underserved areas.14,52 We argue that strengthening the role of HSAs with proper training and support will facilitate referral at the community level.
Although our study showed that a previous positive or negative experience with referral influenced referral, previous studies showed contrary results where mothers with a previous bad experience following referral would blame themselves for the outcome and still reported to the facility, 50 and others reported being satisfied with the referral process and the services received at the referral hospital. 54 The inclusion and strengthening of ETAT guidelines, would assist with fast examination and treatment of the most severely ill children to minimize negative outcomes and experiences. ETAT guidelines were developed in Malawi to complement IMCI guidelines, by guiding non-clinical health workers on the immediate identification of children with life-threatening conditions and expected management.14,55 Furthermore our study showed that health workers’ experience with referral also influenced referral of under-five children in this study. This finding builds on what was reported in Iran that noncompliance with referral among health care workers stemmed from inadequate knowledge on the referral process. 18 Therefore, we argue that there is a need to train health workers on the importance of the relevance of referral as well as establishing the guidelines in Malawi to assist health workers in making evidence-based decisions.
The involvement of the community through the provision of transport and psychological support as illustrated in our study resonates with a Nigerian study where families and communities were responsible for supporting the patient through the provision of transportation means or fares. 22 In Ghana, this support was in the form of community members volunteering to provide care to patients and accompanying them to the health facilities for skilled attendance. 56 We argue that community members should actively be involved in activities happening in their setting by using the principle of solidarity to ensure that they offer assistance to one another when need be. 57
For a referral to be effective, there is a need for reliable transportation for the patients such that having designated ambulances that are functional within the health facilities does not only reduce the time taken to get to the referral hospital but also helps to reduce costs on the health system that may come due to complications if referrals are delayed. 25 Health facilities facing transportation challenges should partner with the communities, make efforts to lobby the government for the provision of an ambulance, these can be bi/tricycle ambulances or the standard ones.
Implementation of community education programs on the reasons and importance of referral, and highlighting the community’s role as the main stakeholders have potential in timely referral because they will be well informed to recognize an emergency within their setting and provide prompt assistance within the community such as transport. 58 Those in a good position to help with such programs are the community health workers or volunteer community workers since they are within the communities and they understand their communities. 59
Facilities need to have a constant means of communication during referrals, like cell phones or radio communication gadgets, starting from the referring to the receiving hospital to help reduce delays. This communication will enhance proper and prompt preparation of the receiving hospital when a case is referred, the same communication should continue even when the patient has been discharged from the main hospital back to the referring, for continuity of care through follow-ups and to guide each other to prevent future mistakes within the referral system.60-62 In resource-limited settings like Malawi, implementing communication gadgets that are user-friendly like radio communication gadgets would be a good initiative to help reduce the burden that comes with untimely referrals, staff members would be trained on how to operate such in all health facilities so that communication among them is timely and directed to the right department.60,61
Strengths and Limitations of the Study
The main strength of this study lies in the use of different methods of drawing information to maximize the depth of the findings and also the use of various stakeholders involved in the referral process. Although our study provides insights on the referral process that exists between primary and tertiary facilities, there is a need for a much broader study that explores the different referral pathways that also include the community level of care and private facilities. Future studies should focus on the pre-referral and during referral treatment that a child receives as well as the establishment of referral strategy, policies, and documents to ensure that the process is well structured.
Conclusion
Several factors influence the referral process such that interventions to strengthen the process should focus on each level to achieve an uninterrupted referral process. There is a need to establish referral guidelines in tandem with the context where referral takes place so that health care workers and caregivers know what to do when a referral is delayed. The systems within a community can be leveraged to support both civic education and also structural support for the referral process.
Footnotes
Acknowledgements
We would like to express our gratitude to health care providers who took part in the study especially those who work at OPD and under-five clinic for their support and the director of health and social service who allowed us to conduct our study at Ndirande Health Centre. We also appreciate the caretakers who took part in the study.
Author Contributions
The study was conceptualized developed and conducted by WK and TU under the supervision of ALNM. WK, TU and MEC drafted the initial manuscript and the manuscript was further reviewed and edited by ALNM. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.