
Abstract
Chronic refractory constipation (CRC) is defined as children who are unable to pass stools in spite of being on maximum laxative therapy and require daily rectal stimulation in the form of enemas or suppositories to pass stools for >3 months. Children are often referred for treatment of refractory constipation that may result from uncontrolled underlying disease or ineffective treatment. Constipated children can be managed by a variety of medical therapeutic options that yield satisfying results in most cases. However, a subset of constipated children fails to benefit from conventional treatments. On treatment failure or on suspicion of organic disease the patient should be referred for further evaluation. Treatment options for treatment-resistant patients are presented. Pharmalogical and non-pharmalogical treatment modalities are reviewed and an algorithm for refractory constipation in children are presented.
Keywords
Introduction
Chronic constipation is one of the most common chronic disorders of childhood, affecting 1% to 30% of children worldwide. 1 Constipation is responsible for 3% of all primary care visits for children and 10% to 25% of pediatric gastroenterology visits. 2 To assist health care workers and pediatricians in the management of all of the children with constipation in primary and tertiary care, the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition NASPHGHAN and ESPGHAN elected to develop evidence-based guidelines as a joint effort. 2
This article reviews the definition, prevalence, and etiology of chronic refractory constipation in children with common pitfalls in assessment and management of refractory chronic constipation.
Definition of Chronic Refractory Constipation
There is no single accepted definition of refractory constipation, but chronic refractory constipation (CRC) is defined as children who are unable to pass stools in spite of being on maximum laxative therapy and require daily rectal stimulation in the form of enemas or suppositories to pass stools for >3 months. 2 It is not clear what is the choice of drug or combinations of drugs applied in definition of CRC. In adult refractory constipation symptoms, it is defined by a 4-week trial of pharmacologic therapy to each drug or a 3-month trial of pelvic floor behavioral therapy. 3 However, the definition for pharmacologically refractory constipation is lacking in adulthood and childhood constipation. In systemic review included 61 studies, there is no consensus on the choice of drug, order of usage, and dosage before submitting patients to invasive treatments and to evaluate new pharmacological agents. 4 Most people can be treated successively with laxatives agents, but a subgroup of patients develop severe symptoms that are refractory to conservative therapies including biofeedback and irrigation, and result in significant deterioration in quality of life. 5
Prevalence of Chronic Refractory Constipation
The prevalence of CRC ranged between 20% and 30%, but the prevalence is much higher in underdeveloped countries like India. 6 Increased prevalence of CRC could be explained by defecation symptoms resulting from long-term fecal impaction or if it is a primary alteration in colonic motility. 7 In Saudi Arabia, the importance of chronic constipation in the demographic profile of pediatric diseases is demonstrated by its prevalence 32%, observed in school-children. 8 We evaluated the knowledge and practice styles among medical providers working in Saudi Arabia regarding their approach to childhood constipation. In response to questions about strategies for the management of chronic refractory constipation, 9.8% reported that they would maximize laxative dose, 22.2% would add or change to another laxative class, 19.5% would encourage dietary changes, 39.9% would refer to a pediatric gastroenterologist, and 8.7% would refer to a pediatric surgeon. No significant differences were found between pediatricians and other physicians regarding management of refractory chronic constipation. 9
Etiology of Chronic Refractory Constipation
The most important reasons of refractoriness of constipation are the following; inadequate dose of laxatives, poor compliance to treatment, and lack of long-term follow-up of constipated children. These may be explained by the lack of awareness about optimal conventional treatment guidelines of constipation in children. However, there are some causes of refractory constipation listed in Figure 1.

Etiology of chronic refractory constipation.
Delayed passage of meconium and refractory constipation in infancy are clinically suggestive of Hirschsprung’s disease (HD). 10 HD is common cause of lower intestinal obstruction in neonates while is a rare cause of intractable constipation in older children. 10 It occurs in 1 in 5000 live births and is characterized by absence of ganglion cells within the myenteric and submucosal plexus of the colon. 10 Delayed passage of meconium in the first 24 hours of life, bilious vomiting, abdominal distension, refusal to feed, severe constipation not responded to maximum laxative and failure to thrive are suggestive symptoms of HD. 11 Diagnosis of HD is very critical because of enterocolitis which is the serious complication of HD. 11 Recognizing of enterocolitis (fever, abdominal distension, and bloody diarrhea) would reduce the mortality of HD. Meinds et al 12 found that anorectal manometry is a viable screening tool for HD because both the sensitivity and specificity of anorectal manometry were equivalent to rectal suction biopsy with a 100% negative predictive value. However rectal biopsies demonstrating the absence of ganglion cells in the submucosal plexus are diagnostic of HD. 13 Ultra-short-segment HD should be kept in mind and may go undiagnosed until childhood. Affected children have ribbon-like stools, a distended abdomen, and failure to thrive. 13
Some studies have suggested a link between celiac disease and chronic constipation. Amanda et al found the prevalence of celiac disease in 1809 children with chronic constipation was 0.5%. It was concluded that routine testing of school-children with functional constipation for celiac disease is not indicated. 14 Another 2 studied did nor recommended to routinely test celiac disease in chronic constipation. However, all previous studied emphasized on chronic functional constipation not on refractory chronic constipation.15,16 Akman et al 17 showed that a celiac disease ratio of 1:28 was diagnosed in chronically refractory constipated children. The use of screening tests for celiac disease should be considered in children with conventional treatment-resistant constipation.
Cow milk allergy in the form of lymphoid nodular hyperplasia by endoscopic and histologic findings is related to chronic refractory constipation. 18 Histologic findings other than lymphoid accumulation and mildly increased density of eosinophils were improved during the cow’s milk challenge and elimination test. 18 A double-blind, crossover study confirmed that intolerance of cow’s milk can cause severe perianal lesions with pain on defecation and consequent chronic constipation in young children. They were also more likely to have anal fissures and erythema or edema at base line (40 of 44 vs 9 of 21, P < .001), evidence of inflammation of the rectal mucosa on biopsy (26 of 44 vs 5 of 21, P = .008), and signs of hypersensitivity, such as specific IgE antibodies to cow’s-milk antigens (31 of 44 vs 4 of 21, P < .001). 19 In contrast, Simeone et al 20 showed that 15.9% children were refractory to constipation treatment, and 27.3% of these had atopy. The 4-week trial of dietary elimination did not result in improvement in constipation. CRC does not seem to be related to cow’s milk allergy.
The importance of chronic constipation in patients with cystic fibrosis is expressed by the presence of constipation-induced rectal prolapse and distal intestinal obstruction syndrome (DIOS). 21 A recent meta-analysis showed that the prevalence constipation in patients with cystic fibrosis varied from 10% to 57%. Refractory constipation is a frequent but still insufficiently assessed complaint of cystic fibrosis patients. 22
Colon and anorectal malformations occur in approximately 1 out of every 5000 births and are slightly more common in males. 23 Anorectal malformation is a common cause of constipation in neonates and infants. Anogenital distance (AGD), the distance from the anus to the genital tubercle. The AGD measure was about 2-fold greater in males (mean, 22 mm) than in females (mean, 11 mm). Fischer et al 24 found that AGD increased from birth to 6 months of age and thereafter reached a plateau. The position of the normal anus defined by the ano-genital index must be looked for an anterior displacement of the anus. Diagnosis of anterior displacement is made by physical examination, barium enema (which reveals the rectal “cul-de-sac” and the distension of the colon). 25 Herek and Polat 26 evaluated the incidence anterior displacement of the anus and its relationship to constipation in 357 children. The incidence of constipation in children with a normal anal index and those with a low anal index indicative of an incidence anterior displacement was not significantly different.
Chronic refractory constipation is commonly associated with primary hyperparathyroidism and probably attributable to hypercalcemia.27,28 The mechanism of hypercalcemia causing constipation is thought by an increase in the concentration of the calcium ions reduces the neuromuscular excitability and causes atonia in the gastrointestinal muscles. 29
Connective tissue disorders such as systemic sclerosis, sclerodermiform syndromes, juvenile dermatomyositis, eosinophilic fasciitis, and Sjogren syndrome involve gastrointestinal tract, and affecting >60% of patients.30,31 About 39 children with slow transit constipation and 41 controls were investigated whether there was a greater prevalence of generalized joint hypermobility among patients with slow transit constipation. It was suggested that a disorder of connective tissue synthesis plays a role in the etiology of slow transit constipation. 32
Slow transit constipation is a clinical syndrome predominantly affecting adults characterized by constipation and delayed colonic transit, occasionally associated with pelvic floor dysfunction. Data of slow transit constipation in children are scarce. In pediatric it is a newly described subtype of intractable refractory constipation in children which we originally identified with deficiency of substance P in axons supplying the proximal colonic muscle. 33 The etiology of slow transit constipation remains obscure and the optimal management is poorly defined. Common features of slow transit constipation include delayed passage of the first meconium stool beyond 24 hours of age, symptoms of severe constipation within a year, or treatment-resistant “encopresis” at 2 to 3 years, infrequent bowel actions, and delay in colonic transit on a transit study. 33 By contrast to functional fecal retention constipation, patients with slow transit have softer feces, respond poorly to laxatives and less commonly develop megacolon. 33
Spinal cord abnormality is one of the missed causes of refractory constipation. Pilonidal dimple covered by tuft of hair, midline pigmentary abnormalities of lower spine, and abnormal neurologic examination (absent anal wink, absent cremasteric reflex, decreased lower extremity reflexes, and/or tone) are the red flags of chronic refractory constipation. 34
Management of Chronic Refractory Constipation
At present, constipated children can be managed by a variety of medical therapeutic options that yield satisfying results in most cases. 35 However, a subset of constipated children fails to benefit from conventional and sometimes even intensive treatments. 2 In patients with true unresponsiveness to first-line osmotic laxatives, a combination (rescue agents) approach can be used, introducing stimulant laxatives such as bisacodyl and sodium picosulfate. These agents are able to elicit bowel propulsion, secretory effects on the enteric mucosa, and appear to be quite safe even in the long-term. 35 The management of refractory constipation is currently regarded as a challenging area, where the paucity of supportive clinical evidence for pediatricians and pediatric gastroenterologists. Management of chronic refractory constipation is divided into pharmacological therapy and non-pharmacological therapy.
Pharmacological Therapy
Prucalopride
Prucalopride is a potent and selective, high-affinity agonist of the 5-hydroxytryptamine (serotonin) receptor 4 that enhances motility in the gastrointestinal tract with enterokinetic properties, able to accelerate the gastrointestinal and colonic transit in constipated patients without abnormal rectal evacuatory dysfunction as a result of an increase of high-amplitude propulsive contractions. 36 Controlled studies in adult women patients unresponsive to standard medical regimens have shown that this drug at the dose of 2 mg/day can be effective in relieving constipation both in the short- and long-term.37,38
In children, Winter et al 39 showed that a single oral dose of 0.03 mg/kg prucalopride was administered to 38 children for 8 weeks duration. Prucalopride treatment resulted in a mean bowel movement frequency of 6.8/week, normal stool consistency, and reduced frequency of fecal incontinence. He concluded that prucalopride had an apparent favorable efficacy and tolerability profile in children with functional constipation. 39 In contrast, multicenter, randomized, placebo-controlled, double-blind study performed in in 213 children demonstrated that the proportion of responders was similar between groups (prucalopride, 17.0% and placebo, 17.8%) with no statistically significant differences in the primary efficacy end point. Although prucalopride generally well tolerated, was not more effective than placebo in children with refractory functional constipation. 40 There is no enough pediatric data to recommend prucalopride in refractory constipation and it is still investigational drugs in children.
Lubiprostone
Lubiprostone is an oral chloride channel protein-2 activator in enteric epithelial cells that stimulates gastrointestinal fluid secretion, softens stools, and facilitates bowel movements. 41
Several studies in adults have been shown that lubiprostone improve constipation at a dose of 24 μg twice a day. Stool consistency, frequency, straining, and constipation severity were significantly improved with lubiprostone compared with placebo.42-45 In children, Hyman et al 46 enrolled 124 children treated with lubiprostone at doses of 12 μg once daily, 12 μg twice daily, or 24 μg twice daily based on age and weight. Mean spontaneous bowel movements (SBMs) frequency significantly increased compared with baseline at week 1 (3.1 vs 1.5 SBMs/week, P < .0001). SBM frequency was improved significantly from baseline overall (P < .0001) and for individual dose groups (P ≤ .0062) during weeks 2, 3, and 4. This study showed that lubiprostone was efficacious and well tolerated in children and adolescents with functional constipation. 46 A multicenter, randomized, double-blind, placebo-controlled is recently published and showed that 606 children were evaluated for the efficacy and safety of lubiprostone 12 μg twice daily (BID) and 24 μg BID. Lubiprostone did not demonstrate statistically significant effectiveness over placebo in children and adolescents with chronic constipation. 47 There is no enough pediatric data to consider lubiprostone it in the clinical practice in chronic refractory constipation in addition that it is of limited use for treatment of cystic fibrosis -related intestinal disease. 48
Other Pharmacological Therapies
Other pharmacological therapies including bisacodyl used infrequently in childhood refractory constipation. Bonilla et al 49 recently reported that bisacodyl is effective and well tolerated in the long-term treatment of childhood constipation refractory to conventional therapy. Most of patients (57%) had a favorable response were successfully weaned off the medication with little side effects. 49 More recently, linaclotide, a guanylate cyclase-C agonist, has been approved for treatment of patients with chronic constipation. 50 This drug at a dose of 145 μg once daily has been found to be effective in the short-term for treatment of chronic constipation in a recent meta-analysis. 51 However, linaclotide data in children are lacking. A retrospective study performed recently in 93 children treated with linaclotide. About 45% of patients with functional constipation and 42% with irritable bowel syndrome with constipation had a positive clinical response at first follow-up a median of 2.5 and 2.4 months after starting linaclotide, respectively. Approximately a third of patients experienced adverse events and eventually 27% stopped using linaclotide due to adverse events. The most common adverse events were diarrhea, abdominal pain, nausea, and bloating. 52 Although colchicine has a narrow therapeutic index which is associated with underestimated toxicity and frequent and serious adverse effects, it has been tested in randomized, double-blind, placebo-controlled, crossover trial which increases the frequency of bowel movements and hastens colonic transit in patients with chronic refractory constipation. This drug was not tested in children.53,54
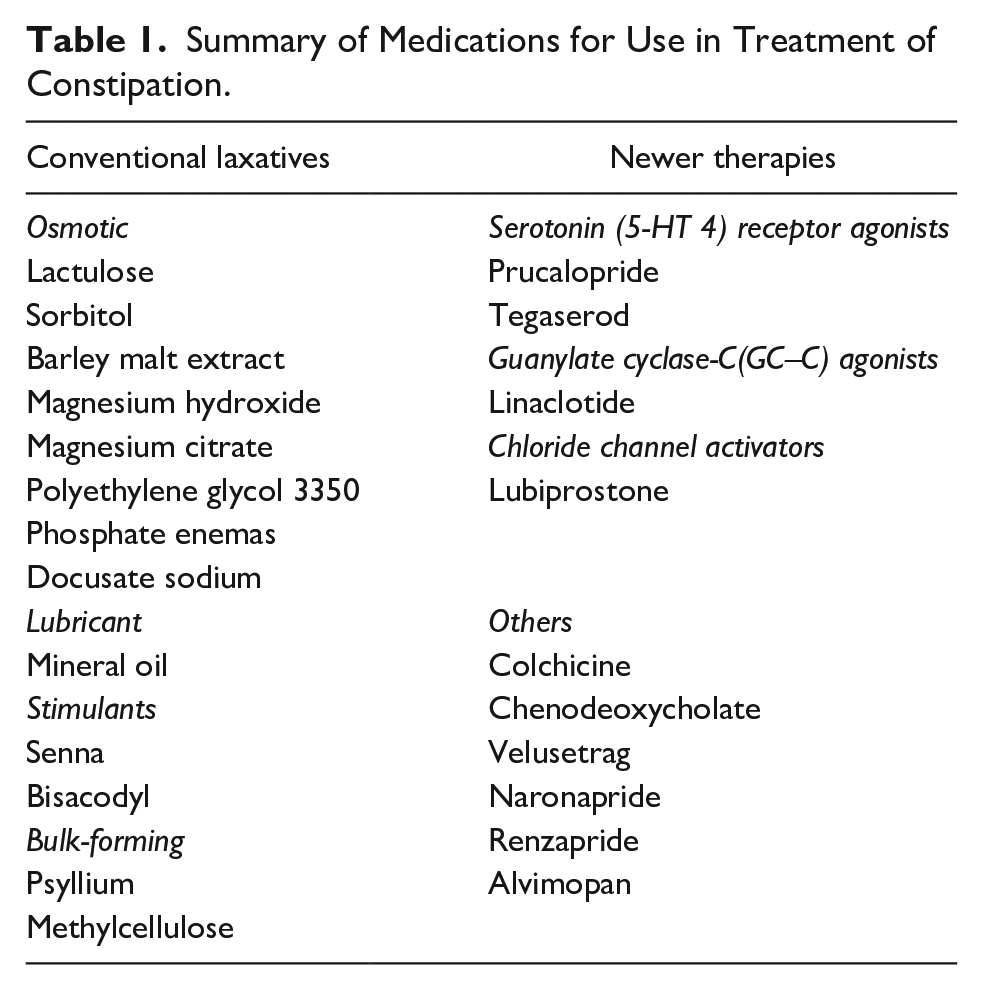
Inhibitors of the ileal bile acid transporter is aimed to reduce the absorption of bile acids in the ileum resulting in an increased entrance of bile acids into the colon, thereby stimulating colonic motility and intracolonic secretion. 55 Recently A3309 is a minimally absorbed ileal bile acid (BA) transporter (IBAT) inhibitor increased stool frequency and improved constipation; effects were maintained over 8 weeks of treatment. 56 Other new medications such as renzapride, chenodeoxycholate, velusetrag, naronapride, and plecanatide for treatment of refractory constipation remain under evaluation. 57 Summary of medications for use in treatment of constipation is shown in Table 1.
Summary of Medications for Use in Treatment of Constipation.
Non-Pharmacological Therapy
Antegrade continence enema (ACE) is a proximal colonic stoma that allows antegrade lavage of the colon for the treatment of fecal incontinence and refractory constipation. In systemic review, ACE has been reported as an acceptable treatment of both functional constipation and fecal incontinence in adults. 58 In children, appendix is used as conduit to insert cecostomy button (Chait trapdoor button) to give enema. 59 It has minimal scar and just a button at right iliac fossa which is used in the morning to give antegrade enema and the whole day patient remains dry (no soiling). In a recent study on 203 cases (median age 10 years, follow up 5.5 years, 62% due to refractory chronic idiopathic constipation) of this modality, Randall et al 60 showed good result in 93%, soiling prevented in 75% and symptoms resolved (no longer on ACE) in 26% (81% of them were chronic idiopathic constipation). A recent study compared ACE treatment and sacral nerve stimulation (SNS) in children with intractable constipation (IC) and fecal incontinence (FI). 61 The study included 23 patients treated with ACE and 19 patients treated with SNS. Improvement in FI was greater with SNS than ACE at 12 months (92.9% vs 57.1%, P = .03) and 24 months (100% vs 57.1%, P = .02). Improvement in bowel movement frequency was greater with ACE, and children were more likely to discontinue laxatives at all follow-up time points (all P < .05). It was concluded that SNS appears more effective for FI and ACE more effective in improving BM frequency and abdominal pain and in discontinuation of laxatives. 61
It sounds that ACE helps in some types of constipation such as slow transit constipation and spinal cord defects. However, ACE has common complications like stoma stenosis, leakage, prolapse, adhesive obstruction and the difficulty in catheterization.
Botulinum toxin (BT) is a new treatment in CRC. BT injection in internal sphincter can improve the obstructed defecation by relaxing the anal sphincter and reducing the required force to propel the stool. 62 A retrospective study of 164 children by Zar-Kessler et al 62 showed that BT is effective in chronic refractory constipation, regardless of anal sphincter dynamics. A meta-analysis on different treatment strategies for obstructive symptoms showed short-term improvement after BT injections in 77% of patients and decreased to 43% of patients in the long-term. This systematic review indicates that BT injection is effective in treating chronic refractory constipation. 63
In children with refractory constipation due to neurogenic bowel, conservative, trans-anal irrigation such a Peristeen® trans-anal enema was effective to improve bowel symptoms and had the greater the reduction in the severity of constipation. 64 86% of the parents were satisfied with the result of trans-anal irrigation and 67% reported that they would continue using trans-anal irrigation for the treatment of intractable functional constipation. 65
Pelvic floor physical therapy (PFPT) is a novel treatment in pediatrics for the treatment of chronic constipation with dyssynergic defecation and can be diagnosed using anorectal manometry. Zar-Kessler et al 66 showed that 76% of the patients who received physical therapy had improvement in constipation symptoms, compared to 25% of the patients on conservative treatment (P < .01). Multiple studies on the use of PFPT and biofeedback have proven efficacious in the adult population. However, based on the negative results from these long-term studies, the current standard of care in pediatric constipation does not include biofeedback or PFPT as treatment of any form of pelvic outlet obstruction.2,67
A suggested algorithm for management of refractory constipation is shown in Figure 2. The most useful test for the evaluation CRC is the CTT with radiopaque markers (sitz). CTT via ingestion of radiopaque markers followed by a plain abdominal x-ray is simpler and more palatable to many patients; thus, CTT is likely more frequently performed in the community prior to anorectal manometry. 68 It is useful in establishing the diagnosis of childhood slow transit constipation with soiling and it has been standardized in both normal children, and those with constipation. Bautista Casasnovas et al 69 chowed that CTT in healthy non-constipated children found segmental and total colon transit times was 29 ± 4 and 37.8 ± 6.2 hours, respectively. Benninga et al 70 defined slow transit time as a total colonic transit time of >100 hours (mean + 2SD). CTT is useful for diagnosis of HD, childhood visceral myopathy type II, pseudo-obstruction, and cystic fibrosis. 71 A multicenter, retrospective cohort study demonstrated that there is no association between rectosigmoid location of markers and prolonged balloon expulsion, even it does not correlate with measures of symptom severity. 72

Suggested algorithm for refractory constipation in children.
Whether to use biofeedback or newer drugs like colon-specific prokinetics, it depends on abnormalities detected on colonic transit time (CTT) and anorectal manometry. If refractory constipation is due to dyssynergic defecation, biofeedback (to restore the normal pattern of defecation) will be the best choice. If refractory constipation is due to slow transit constipation, the management will be quite difficult as they do not respond to conventional laxative therapy and the main concern is soiling.
Conclusion
Refractoriness of childhood constipation to medical treatments is still a significant issue. Children are often referred for treatment of refractory constipation that may result from uncontrolled underlying disease or ineffective treatment. Based on preliminary evidence and experience in clinical practice in adulthood constipation, enterokinetics, secretagogues, and non-pharmacological interventions might be worthy of validation by clinical research in children. Further studies are warranted to explore its suitability in chronic refractory constipation in children.
Footnotes
Author Contributions
MH searched and selected the studies, and wrote the first draft of paper. He reviewed and edited the manuscript before submission. He approved the final submitted version.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
The ethics committees did not require ethical approval and informed consent because the study based on review of published literature.