
Abstract
Melanosis coli is a dark to brown pigmentation of the colon due to lipofuscin deposition within the cytoplasm of cells. It is a benign condition associated with excessive use of laxatives, particularly those that are anthracene derivatives and common herbal remedies like Cassia Angustifolla (senna). It is usually asymptomatic and diagnosed incidentally during colonoscopy or histopathologic evaluation. We present a case of a 56-year-old male patient who presented with diarrhea of 3 months duration, which started after he began to use California herbal tea for his constipation. Colonoscopic evaluation revealed an intense pigmentation throughout the colon suggestive of Melanosis coli, which was confirmed on histopathology. In patients with prolonged use of California herbal tea and dark to brown pigmentations of colonic mucosa on colonoscopy, there should be a high index of suspicion for Melanosis coli. And patients should be aware of the risk of developing Melanosis coli following prolonged herbal tea use. The findings presented in our case are in support of few previous literature that showed relations between chronic herbal tea use and Melanosis coli.
Introduction
Melanosis coli is an acquired benign condition, often identified incidentally during colonoscopy, characterized by dark to brown pigmentation of the colonic mucosa due to lipofuscin deposition within the cytoplasm of cells.1,2 This condition was first described by Andral and Cruveilhier in 1830.1,3 Melanosis coli usually develop in those who use laxatives chronically, particularly those containing anthracene derivatives. 1 The active ingredients having a laxative effect are also commonly present in natural herbal teas. 4 When the active forms of these laxative molecules pass into the lining of the large bowel, it results in cell damage and death. The dark pigment is then created once the macrophages in the colonic lamina propria are stained by lipofuscin pigment as a result of phagocytosis of apoptotic epithelial cells.5–7 The term “melanosis” is a misnomer as electron microscopy and X-ray analyzing methods proved that the deposited pigment is lipofuscin, not melanin. 8 The higher pigment intensity observed in the proximal colon and cecum could possibly reflect higher luminal concentrations of an offending agent in the proximal colon, differential absorptions along the length of the colon, or differences in macrophage distribution within the colon. 3 It affects both sexes equally and is typically seen in individuals over the age of 45, possibly due to the fact that older persons are more prone to chronic constipation and hence the use of laxatives.1,5
Case presentation
A 56-year-old male patient with well-controlled hypertension and type 2 diabetes mellitus on Enalapril, Galvus Met (vildagliptin + metformin) and Atorvastatin presented with 3 months of diarrhea. The patient reported a history of using California herbal tea daily for constipation and weight loss for the past 4 months. On physical examination, he had no oral mucosa or skin hyperpigmentation and the abdomen was soft and nontender. Laboratory tests revealed normal complete blood cell count, renal function tests, liver enzymes and bilirubin, and hemoglobin A1C of 6.2%. Abdominal ultrasound showed non-alcoholic fatty liver disease (NAFLD). Colonoscopy revealed intense pigmentation throughout the colon consistent with Melanosis coli (Figure 1(a) and (b)). No polyp or other mass was seen on colonoscopy. Biopsies were taken, and histopathology confirmed that there are scattered numerous pigment-laden macrophages with golden brown cytoplasm in the lamina propria but no evidence of dysplasia or malignancy (Figure 2(a)–(c)). The patient was advised to discontinue using the stimulant laxative and follow up with his primary care physician for diabetes management.
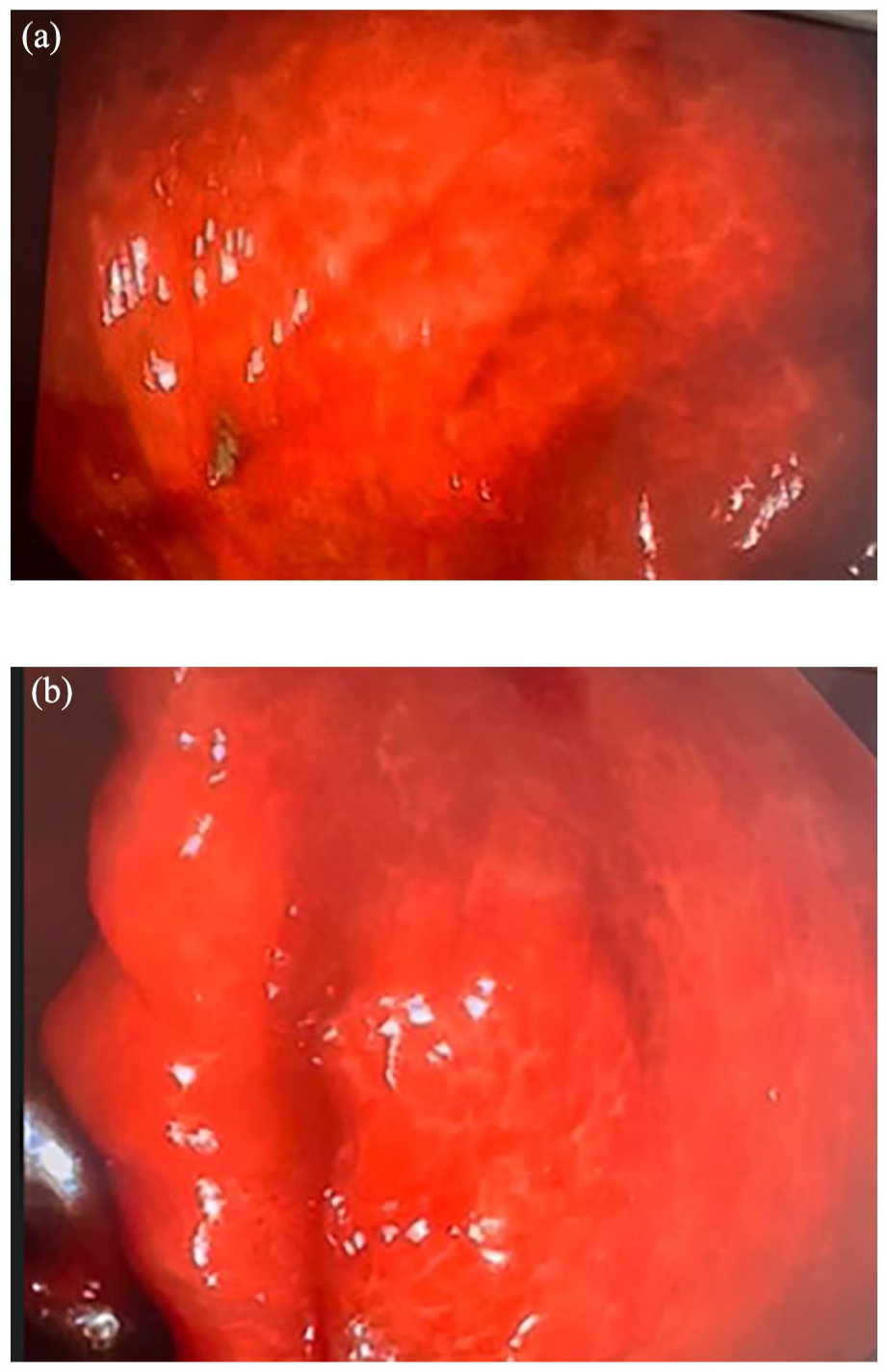
(a) and (b) Colonoscopy showing an intense pigmentations throughout the colon consistent with Melanosis coli.
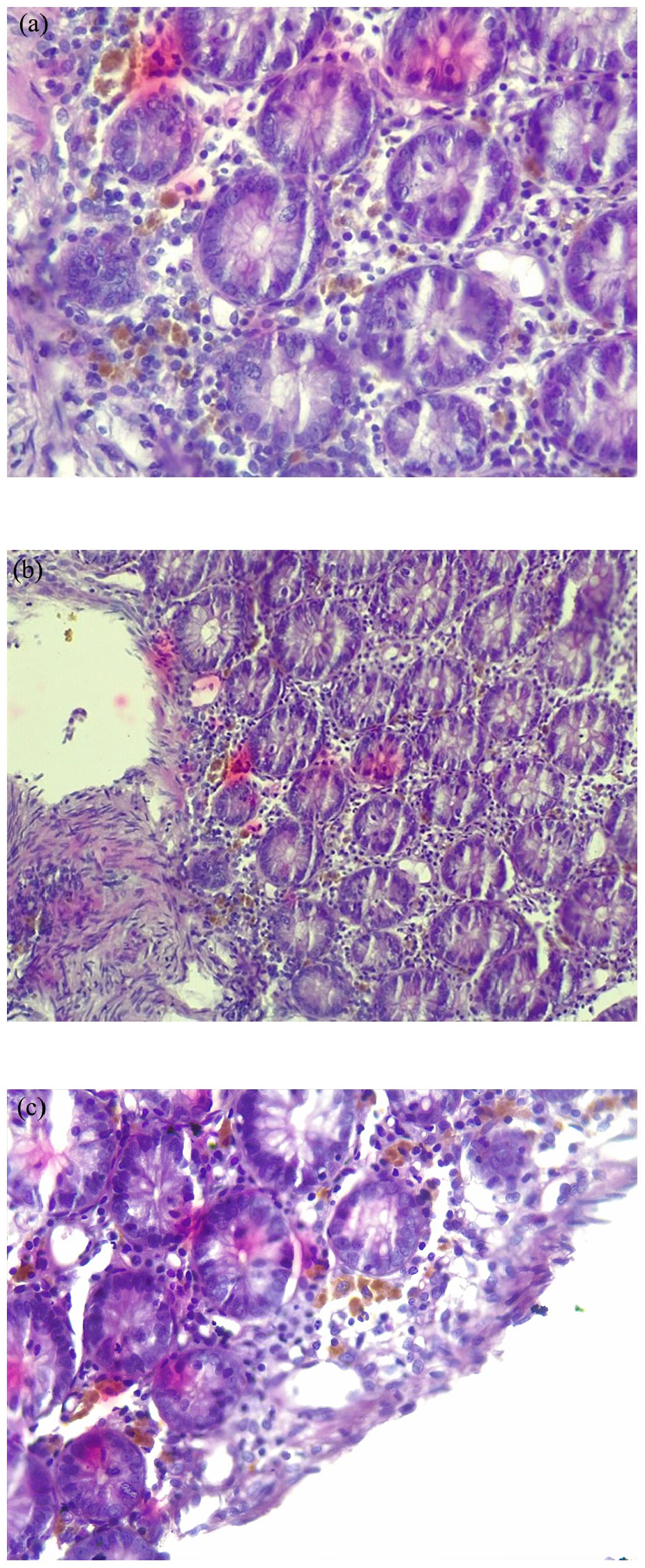
(a)–(c) H&E stain of colonic mucosal biopsy showing scattered numerous pigment laden macrophages with golden brown cytoplasm in the lamina propria but no features of dysplasia or malignancy.
Discussion
Melanosis coli develops following prolonged use of laxatives, particularly anthracene derivatives, including aloe, cascara, rhubarb, and sennosides.6,7 Sennosides A and B are also present in a popular plant drug called senna (Cassia angustifolia). 9 Herbal teas containing senna, which are commonly ingested by individuals for their laxative and weight loss effect, are reported to have associations with the development of Melanosis coli. 4 California herbal tea, which is used by our patient, is one of those teas containing senna. 10
Melanosis coli can develop 4–12 months after chronic laxative use. 7 Elderly and those with irritable bowel syndrome and constipation are at-risk groups for the development of Melanosis coli. 7 Diabetic patients are also at increased risk of chronic constipation. 11 Although both sexes are affected equally, a recent study revealed that there is a greater tendency for progression among male patients. 12 There is no documented relation between NAFLD and development of Melanosis coli. Instead, the sennosides are known for their mitochondrial protective effect and inhibition of hepatic steatosis. 13 Our patient is a diabetic elderly man who has a history of chronic constipation and the concomitant finding of NAFLD with Melanosis coli is likely incidental.
Melanosis coli has no specific symptoms or signs. Usually, it is found incidentally on endoscopic evaluation and is most commonly located in cecum and proximal colon.3,7,8 But predominant descending colon and rectum involvement as well as diffuse whole-length colonic involvements, were also reported.4,14 Our patient is also found to have diffuse colonic involvement.
Melanosis coli is a benign lesion that has no established specific treatment. Management of symptomatic constipation with fiber-containing foods or substances with mucilage, including psyllium, along with avoidance of anthracene-derived laxatives and herbal teas, is recommended.8,14 Dis-appearance of hyperpigmentation is commonly expected after 2 years. 12 But histological findings may persist for many years. 14 Our patient was advised to stop using herbal tea and to manage his constipation with a high-fiber diet. But, subsequent follow-up colonoscopy was not done to check resolution of his lesion.
Peutz-Jeghers syndrome, a hereditary disease of skin and mucous surface pigmentation with melanin (a true melanosis) is differential for Melanosis coli. But, polyps in the digestive tract and predominant intraoral pigmentations are additional features of this syndrome. 15 Our patient has no oral mucosa or skin pigmentations and no polyps were detected on colonoscopy.
Conclusion
Patients should be aware that long-term dependence on laxative use, including herbal teas, could potentially lead to the development of Melanosis coli. Patients who take these products should be under medical supervision. Physicians should have a high index of suspicion if they find colonic hyperpigmentations on colonoscopy and should advise their patients against long-term use of herbal teas or other laxatives.
Footnotes
Acknowledgements
We are grateful to the medical personnel who were caring for the patient.
Authors contribution
All were involved in either data collection, drafting, revising, or finalizing the report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this case report.
Funding
The author(s) received no financial support for the authorship and/or publication of this case report.
Consent for publication
Written informed consent was obtained from to patient to publish his medical information in this report. A copy of the written consent was available for review by the Editor-in-Chief of this journal.