
Abstract
Optimal antenatal care is an important service required by women and babies. To promote healthy motherhood and for positive pregnancy outcomes, World Health Organization recently recommended a minimum of 8 ANC contacts. We aim to explore the prevalence of 8 or more ANC contacts using multi-country data. Urban dwellers, mothers with secondary or higher education, women from high household wealth, early birth order, and older mothers at childbirth had higher prevalence of 8 or more ANC contacts respectively. The pooled prevalence of 8 or more ANC contacts was 13.0%. Jordan had the leading prevalence of 8 or more ANC contacts (74.0%), followed by Ghana (43.0%) and Albania (30.0%). On the other hand, Senegal, Uganda, and Zambia had very low prevalence of 8 or more ANC contacts. There was heterogeneity in the prevalence of 8 or more ANC contacts across countries. There was low prevalence of 8 or more ANC contacts.
Background
Antenatal care (ANC) is a forum for the delivery of vital services to reduce complications in pregnancy, provide birth and emergency preparedness counseling, and improve children’s health outcomes. The 2016 World Health Organization (WHO) prenatal care guidelines for a healthy pregnancy experience reflect a change from the centered ANC model with a prescribed minimum of 4 ANC visits (ANC4+) to a more expanded model that emphasizes contact number, timing, and services. 1 This model suggests a minimum of 8 ANC contacts, with the first contact occurring in the first trimester of gestation followed by the second and third trimesters respectively by 2 and 5 contacts.1,2 The rise from a minimum of 4 to 8 ANC contacts highlights the crucial need to further target women who are less likely to meet the new suggested level for a positive pregnancy experience.
The coverage of ANC is a significant measure reported internationally to assess maternal health. 3 Achieving the previously recommended ANC4+ has become a priority measure for global monitoring of maternal health and used in global initiatives such as the 2030 Countdown, 4 the Ending Preventable Maternal Mortality Program (EPMM),5,6 and the Global Plan for the Health of Mothers, Children, and Adolescents. 7 Albeit, several barriers exist in optimal maternal health care service utilization. The reasons associated with sub-optimal ANC visits include financial constraints, distance from health facilities, cultural and religious attitudes regarding pregnancy, gender norms, lack of knowledge of pregnancy signs and prenatal care schedules, preference for pregnancy, late ANC booking, and quality of care received.8-10
The Sustainable Development Goals (SDGs) aim to reduce maternal mortality to less than 70 per 100 000 live births by 2030. 4 Globally, complications linked to pregnancy lead to over 50% of maternal deaths annually. About 90% to 95% of these deaths come from poor-resource nations, according to the World Health Organization (WHO). 11 Moreover, about 303 000 deaths from pregnancy and childbirth occurred worldwide in 2015, with the majority of these deaths occurring in low-resource settings.12,13 This stunning estimate of maternal mortality contravenes the third objective of SDGs aimed at ensuring healthy lives and promoting well-being for all at all ages. 4 Sub-Saharan Africa (SSA) contributes disproportionately to global maternal deaths, with about 196 000 maternal deaths in 2015. 12 In resource-constrained settings, the lifetime risk of dying from pregnancy and childbirth is 1 in 37 compared to high-income nations, where the lifetime risk of maternal death is 1 in 7800.12,13
Four years after the recommendation for pregnant women to have a minimum of 8 ANC contacts with skilled healthcare providers, only about 15 countries have collected national data suitable to investigate the uptake of the new recommendation. In Africa, the prevalence of 8 or more ANC contacts varied across countries. The prevalence ranges from as low as 8.0% in Republic of Benin 2 and 17.4% in Nigeria. 14 The literature on in-country initialization of the recent recommended increased ANC contacts is practically lacking across many countries. The objective of this study is to determine the prevalence of 8 or more ANC contacts as recommended by WHO in 2016.1,3
Methods
Data Extraction
This study was conducted using the most recent Demographic and Health Survey (DHS) and Malaria Indicator Survey (MIS) multi-country data. The study sample included a total of 203 282 women of reproductive age. The selected countries include: Albania, Benin, Cameroon, Ghana, Guinea, Jordan, Mali, Mozambique, Nigeria, Pakistan, Papua New Guinea, Senegal, Sierra Leone, Uganda, and Zambia. These countries were selected because they have recent data collected after the WHO guideline of 8 or more ANC contacts was endorsed. DHS and MIS used nationally representative data, to collect information on demographic, health, and nutrition indicators. The data is publicly available and can be accessed from MEASURE DHS database at http://dhsprogram.com/data/available-datasets.cfm.
DHS and MIS used a stratified multi-stage cluster random sampling technique and data was collected on vital reproductive health issues via structured interviewer administered questionnaires. The population is divided into classes using the stratification strategy. For example, all surveys use a region with urban-rural stratification. The consideration of demographic disparities in urban and rural areas supports the relatively separate designs in urban and rural areas, and thus the urban-rural region. To divide the population into first-level strata and subdivide the first-level strata into second-level strata, and so on, a multi-level stratification strategy is used. In the surveys, there are 2 levels of stratification: area and urban/rural stratification. Interviewer-administered questionnaires are used to gather the data on important sexual and reproductive health issues. The pregnancy history, in which women were asked about their birth records, was an important part of the data collection. Based on the availability of current data, fifteen (15) countries were included.
It collects a wide variety of objective and self-reported data, with a particular emphasis on measures of fertility, reproductive health, maternal and child health, mortality, diet, and adult self-reported health behaviors. National scope, high-quality interviewer preparation, standardized data collection procedures across countries, and consistent content over time are all advantages of the surveys, enabling cross-sectional and longitudinal comparisons across populations. The surveys data aid epidemiological research aimed at tracking incidence, patterns, and disparities. Cross-sectional designs, repeated cross-sectional designs, spatial and multilevel analyses, intra-household designs, and cross-comparative analyses were among the comprehensive observational data analysis approaches used. 15
Outcome Variable
The number of ANC contacts with physicians, nurses, and midwives was divided into 2 groups: those who had fewer than 8 ANC contacts and those who had 8 or more ANC contacts. A review structure for the 2016 WHO ANC model in support of a healthy pregnancy experience is presented by the WHO ANC guideline recommendations mapped to the 8 suggested contacts.1,3,16
Independent Variables
The explanatory variables included in this study are; place of residence: urban versus rural; educational attainment: no formal education or primary versus secondary or higher education; birth order: 1, 2 to 3, 4 to 5, 6+; mother’s age at child birth: <20, 20 to 34, 35 to 49 years; household wealth quintiles: The wealth indicator weights were assigned using the principal component analysis (PCA) methodology. Household assets such as wall type, floor type, roof type, water supply, sanitation facilities, radio, electricity, television, refrigerator, cooking fuel, furniture, and number of persons per household were used to assign and standardize wealth indicator variable scores. After that, the factor loadings and z-scores were calculated. The indicator values were multiplied by the factor loadings for each household and then summed to produce the household’s wealth index value. The standardized z-score was used to categorize the overall scores into wealth quintiles; poorest, poorer, middle, richest and richest. 17
Analytical Approach
Statistical analysis utilized the survey module (“svy”) command to adjust for stratification, clustering, and sampling weights. Percentage was used in univariate analysis. 18 The forest plot was used to explore the pooled prevalence of 8 or more ANC contacts across the selected countries. Statistical significance was determined at P < .05. Stata version 14 (StataCorp., College Station, TX, USA) was used for data analysis.
Ethical Consideration
This research was focused on an examination of public-domain population-based datasets that were made accessible online with all identifier information removed. MEASURE DHS/ICF International gave the authors permission to use the data. The DHS Program adheres to industry guidelines for protecting the privacy of respondents. ICF International guarantees that the survey complies with the Human Subjects Protection Act of the United States Department of Health and Human Services. Before the survey, the DHS project sought and received the required ethical approval. This research did not require any additional approvals. More information on data and ethical principles can be found at http://goo.gl/ny8T6X.
Results
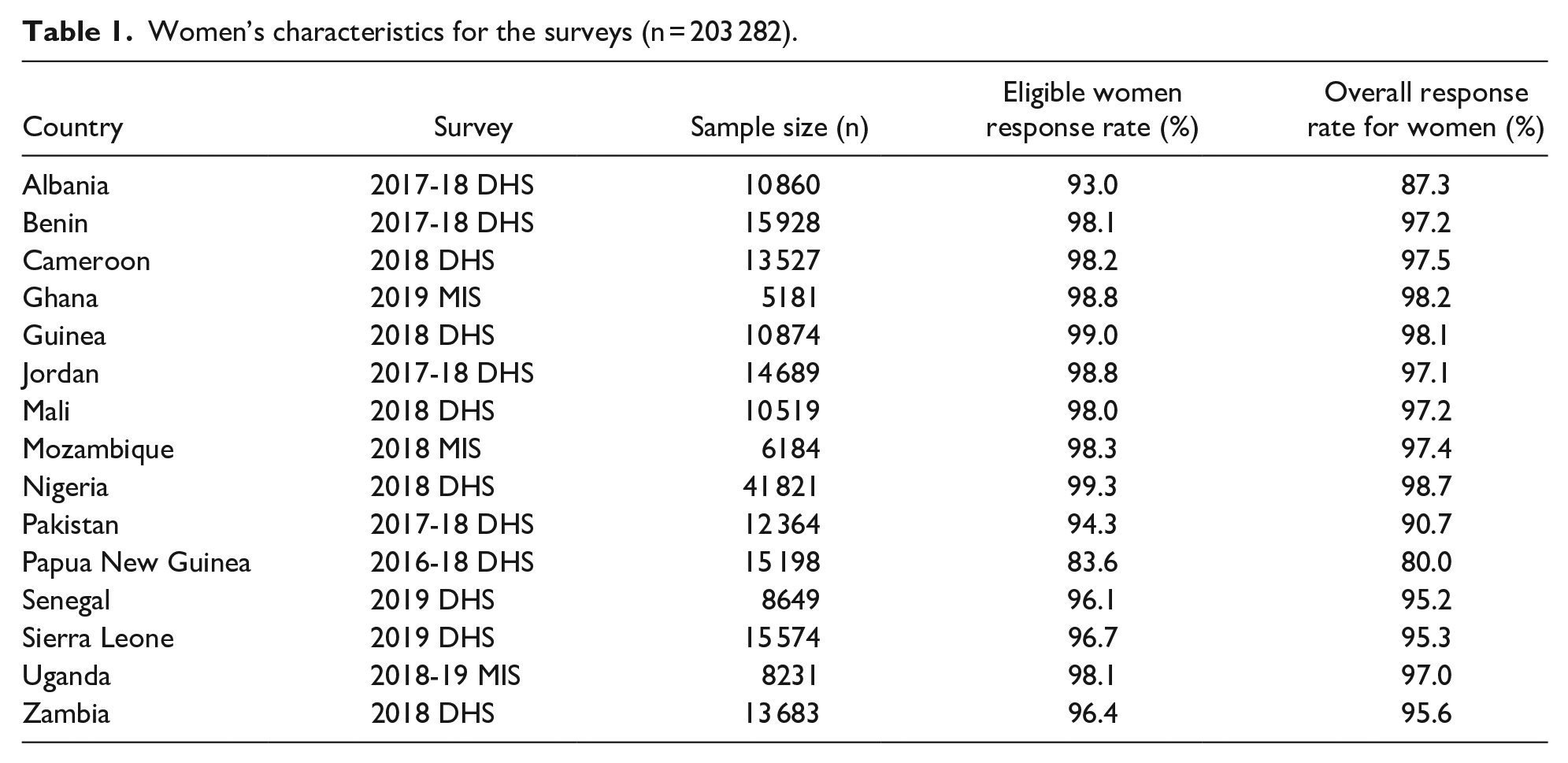
The study sample included a total of 203 282 women of reproductive age. The response rate for eligible women was high and data used were collected in very recent years. See Table 1 for the details.
Women’s characteristics for the surveys (n = 203 282).
In Table 2, we showed the prevalence of 8 or more ANC contacts across several maternal and child characteristics. For the residential status, urban dwellers had higher prevalence of 8 or more ANC contacts in all the studied countries, when compared with their rural counterparts. In addition, there was higher prevalence of 8 or more ANC contacts for mothers with secondary or higher education, when compared with those with no or primary education. Furthermore, the prevalence of 8 or more ANC contacts was greatest, for the highest wealth quintile, when compared with the lower wealth levels. Early birth order has the highest prevalence of 8 or more ANC contacts, when compared with late birth order. The prevalence of 8 or more ANC contacts was higher among older mothers at birth, when compared with those <20 years at birth across the studied countries respectively. See Table 2 for the details.
Distribution of 8 or more antenatal care contacts.

In Figure 1, the pooled prevalence of 8 or more ANC contacts was 13.0%. The percentage of women who had 8 or more contacts ranged from 1% in Senegal, Uganda, and Zambia to 74.0% in Jordan. Specifically, Jordan had the leading 8 or more prevalence of ANC contacts (74.0%), followed by Ghana (43.0%) and Albania (30.0%). On the other hand, several countries including Senegal, Uganda, Zambia, Mozambique, Mali, Guinea, Cameroon, and Benin have very low prevalence of 8 or more ANC contacts. However, there was a significant heterogeneity in 8 or more ANC contacts across the study countries (P < .001). See Figure 1 for the details.
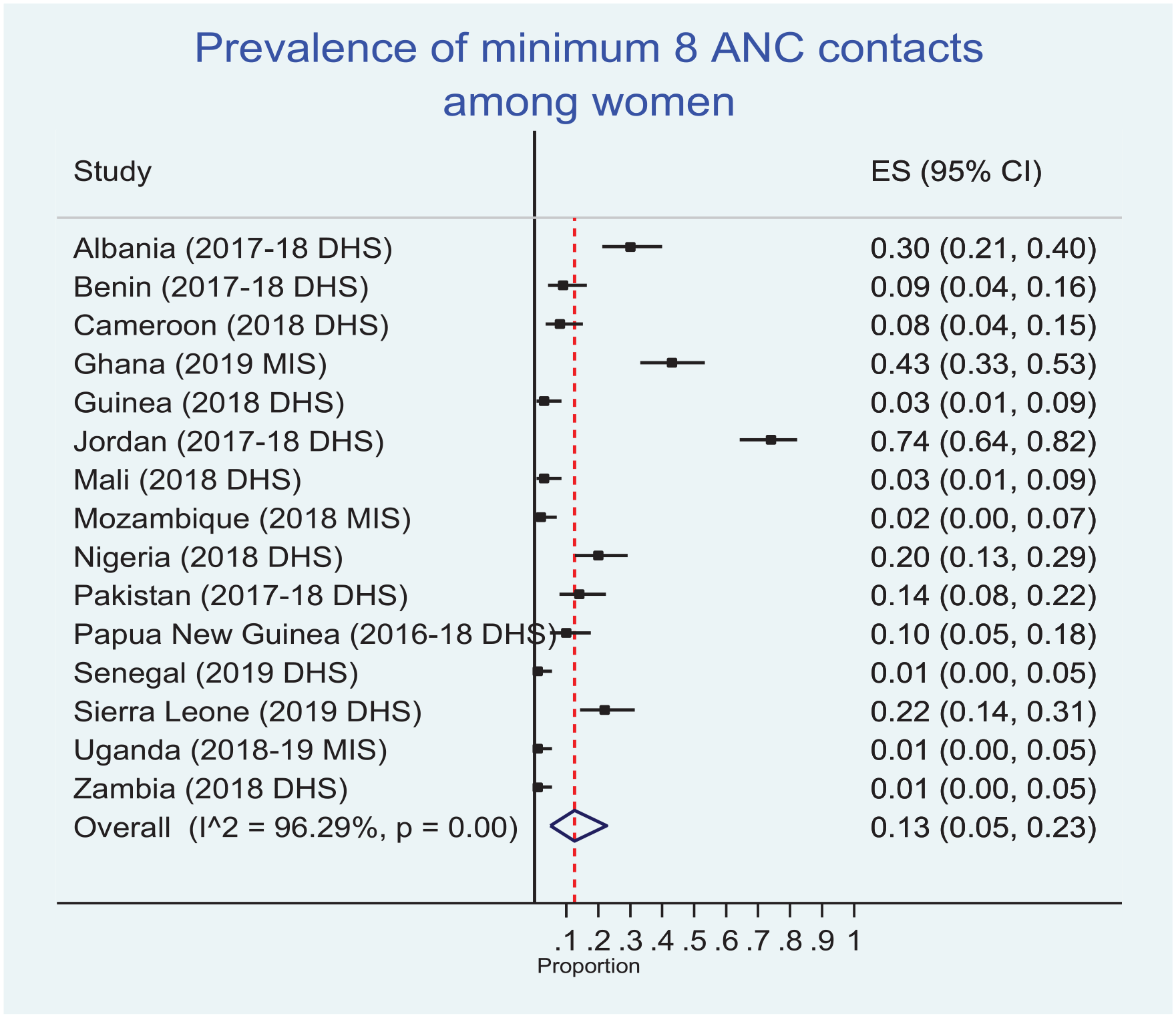
Forest plot on the prevalence of 8 or more ANC contacts.
Discussion
Our study found a pooled prevalence of 8 or more ANC contacts in the 15 studied countries as 13.0%. This prevalence is very poor considering the time lag since the recommendation was made. The prevalence of 8 or more ANC contacts in each of the studied countries ranged from 1% in Senegal, Uganda, and Zambia to 74.0% in Jordan. Specifically, Jordan had the leading prevalence of 8 or more ANC contacts (74.0%), followed by Ghana (43.0%) and Albania (30.0%). On the other hand, several countries including Senegal, Uganda, Zambia, Mozambique, Mali, Guinea, Cameroon, and Benin have very low prevalence of 8 or more ANC contacts. Moreover, our study observed a significant heterogeneity in the prevalence of 8 or more ANC contacts across the study countries. Several factors may have contributed to this low coverage. The 15 countries in this study are practically among the low-and-medium income countries and it has been observed that health care services in these poor-resource countries are inadequate, poor, or non-existent. Several studies have reported that maternal and child health care services are poorly provided in low-and-middle income countries, due to inadequate infrastructure, poor levels of education, poor or low enlightenment, poverty, and when the services are available, women are made to pay out-of-their pocket,19-22 as most women in these poor countries do not have health insurance coverage.2,9,14,23-25 Improved infrastructure, policy formulation in the areas of maternal and child health, women empowerment, comprehensive health insurance coverage especially for reproductive age women are needed to increase of maternal health care utilization.
We compared the prevalence of 8 or more ANC contacts between the rural women versus their urban counterparts. We observed a uniform increase in 8 or more ANC contacts among the urban dwellers in all the 15 studied countries, compared to their rural counterparts. This disparity observed in rural-urban dwellers shows inequality among these women. Rural location has negatively affected the use of ANC as well as use of other maternal care services. Some studies have reported how residing in urban area is advantageous on ANC utilization 14 ; for example, a previous study reported that being an urban resident increases one chances of ANC utilization. 26 In most developing countries, this finding is not unexpected as inequity in the location and distribution of health care facilities are in favor of urban areas, hence women in urban areas have an increased access to quality health care services compared to their rural counterparts.
Our study also found that women with higher educational attainment had increased prevalence of 8 or more ANC contacts. Those with secondary or higher level of education were found to have increased prevalence of 8 or more ANC contacts, when compared to those with no formal or primary education. It is understood that poor access to good and functional health facilities, proximity to health facility, and poor infrastructure are also barriers of getting proper pregnancy care.26-29 Other studies have reported similar findings proving that higher educational status in women promotes greater maternal health care services uptake, when compared with the less educated women.2,8,14,23,24,30 For women to have improved enlightenment level, they need to be exposed to reading educational materials, watching television and listening to news, also be involved in reading newspapers or magazine, and going through formal education. Having these exposures may have been associated to these women’s awareness that early registration and completion of 8 or more ANC is important for positive pregnancy outcomes. These factors have been adjoined to influence maximum maternal health care use.31,32 Higher educational attainment can increase women’s autonomy, enhance healthcare information access, and can support economic independence. 33 This showed the importance of educating the girl-child to at least secondary level of education and empowering her for greater independence such that the issues concerning her health needs especially the reproductive aspect will be decisively taken by her. 34 Higher education or enlightenment are protective factors that enhance women’s health care services utilization and also enhance their reproductive health decision-making.35,36
Our findings showed that non-poor households (ie, those from the highest wealth quintiles) had higher prevalence of 8 or more ANC contacts, when compared with those from poorer households. A previous study has shown that women from the rich households have greater odds to obtain and use maternal health care services than those from the poor households. 37 The rich have the privilege to live in the highbrow areas where adequate facilities including modern facilities are available. The well-off environments often do not lack in these infrastructure, and majorly have access to them. Moreover, the individuals have the resources to pay for health care services and are also better disposed to access health insurance than those from poor households. The SDG-3 is known to advocate for universal health for all by removing inequalities that exist in health care services accessibility. This worthwhile intention may never be achieved if disadvantaged women and poor and rural environment remain hard-to-reach for health care services. It therefore implies that beyond advocacy for utilization of 8 or more ANC, proper strategic plans and effort must be put in place to reach these most disadvantaged group of women in the society. Consolidation on health care programs and policies are important to enhance optimal uptake of ANC contacts among women of reproductive age. It can also improve the utilization of maternal care services, particularly for the uneducated, low household wealth quintiles, and those who live in hard-to-reach rural residence. Due to the fact that household wealth quintile plays important role in women’s ability to obtain maternal health care services, it means that providing women with free maternal and child health care may greatly improve their attendance of ANC. 23 Out-of-pocket payment for maternal health is a major reason that hinders poor and rural women from accessing maternal health services, and this may not stop if free maternal health care services is not made available, particularly for women.
We also observed that women with early birth order had the highest prevalence of 8 or more ANC contacts, than those with late birth order. It is normal to say that women of early birth order are first-timers and inexperience when the matter of child birth is concerned. This may warrant them to make sure that they register and attend adequate ANC visits recommended by their health care providers. It is also assumed that since these women have not experienced childbirth as compared with those who have had previous pregnancies and childbirths, they tend to take ANC services very seriously. Studies have also shown that women of early birth order, often have higher ANC visits when compared with the late birth order women.38-41 It has also been observed that higher birth order is associated with lower ANC visits. That is to say, as the birth order increases, there is the tendency that ANC visits will decrease. 40
This study also found that older women at childbirth had higher prevalence of 8 or more ANC contacts across all the studied countries when compared with women who were 20 years old and less. It has been reported that the older a woman is at the point of childbirth, the tendency for her to have complications is increased. By implication, older women at childbirth are often more predisposed to pregnancy related complications compared with the younger folks. The prone to pregnancy-related complications among older women have been linked to weak body functions at older age. It has been recommended that women that have gotten to the age of 35 years and above at first ever pregnancy should not go for vaginal delivery, rather they should go for elective cesarean section. This recommendation is due to the fact that many physiological activities have taken place and the organs especially those responsible for reproductive activities have at this time becoming weak.
Strengths and Limitations
One of the key strengths of the study lies in the use of the most recent nationally representative datasets of women of reproductive age to examine the WHO recommendation of 8 or more ANC contacts. Moreover, the sample size used in this study supports the generalizability of the findings to all women of reproductive age in the study countries. Nonetheless, one of the paper’s major limitations is the possibility of recall bias, which may result in an over- or underestimation of 8 or more ANC contacts.
Conclusion
This study reveals an unsatisfactory degree of adherence to the WHO’s recommendation of 8 or more ANC contacts. Despite the government’s and non-government organizations’ large focus on ANC contacts as part of healthy motherhood policies and programs, the results of this study show that various countries are still far from achieving universal coverage of the recommended ANC contacts. Women from rural areas, less educated, poor families or socioeconomically disadvantaged, higher birth orders, and young age at childbirth had less coverage of 8 or more ANC contacts. It’s critical that the government and other stakeholders in the health-care delivery system improve the availability, efficiency, cost, and communication about skilled pregnancy care. Moreover, for long-term change, emphasis on improving women’s socioeconomic status and access to high-quality ANC services is recommended. Promoting female education will have a significant impact on women’s health-care behavior. Strengthening the mass-media campaign on the advantages of having an adequate number of ANC contacts would help to improve 8 or more ANC contacts further.
Footnotes
Acknowledgements
The authors appreciate the MEASURE DHS project for the approval and access to the original data.
Author Contributions
ME contributed to the conceptualization, review of literature, initial manuscript preparation, study design, data analysis, wrote the results, and discussed the findings. ME read and approved the final manuscript.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study is a secondary data analysis, which is publicly available, approval was sought from MEASURE DHS/ICF International and permission was granted for this use. The original DHS data were collected in conformity with international and national ethical guidelines. Written consent was obtained from mothers/caregivers and data were recorded anonymously at the time of data collection during the data collection. More details regarding DHS data and ethical standards are available at: ![]()