
Abstract
Objective
We aimed to explore the effect of individualized medical nutrition guidance on pregnancy outcomes among older pregnant women.
Methods
This was a prospective study using a randomized controlled trial design. We selected 820 older pregnant women and randomly divided them into a study group and control group (410 women each). The control group was given routine health education and nutrition guidance; the study group was provided individualized medical nutrition guidance. Gestational diabetes mellitus, hypertensive disorders of pregnancy, vaginal delivery rate, postpartum hemorrhage rate, gestational body weight, neonatal birth weight, and neonate transfer to the neonatal intensive care unit (NICU) were compared between the groups.
Results
The incidence of gestational diabetes in the study group was significantly lower and the rate of vaginal delivery was significantly higher than those in the control group. The incidence of macrosomia, rate of neonatal transfer to the NICU, and rate of neonatal hyperbilirubinemia were significantly lower in the study group than those in the control group.
Conclusions
Individualized nutritional intervention for older pregnant women can effectively reduce the incidence of complications during pregnancy and childbirth and improve maternal and child outcomes.
Keywords
Introduction
The term “older parturient women” refers to women whose maternal age is ≥35 years. With higher educational backgrounds, economic pressure, and for other reasons, the number of older pregnant women has increased each year. Studies have shown that compared with younger women, the incidence of severe pregnancy comorbidities and complications in older women is significantly higher than that in younger women. 1 The risk of adverse pregnancy outcomes for mothers and infants is also significantly higher. 2 At the same time, owing to their older age, older pregnant women attach great importance to fetal health. However, many pregnant women lack knowledge regarding nutrition during pregnancy and often mistakenly believe that the more nutrient intake, the better. As a result, the number of pregnant women with high body mass index (BMI) during pregnancy increases each year, which also increases the incidence of pregnancy complications, such as gestational diabetes mellitus (GDM), 3 pregnancy-induced hypertension, 4 and the rates of cesarean delivery, 5 postpartum hemorrhage (PPH), and macrosomia. 6 Therefore, individualized medical nutrition guidance during pregnancy, particularly for older pregnant women, can improve awareness regarding nutrition during pregnancy by establishing a reasonable dietary structure and behavioral habits to lay a good foundation for the normal growth and development of the fetus. Under the above background, we aimed to provide individualized medical nutrition guidance during pregnancy for older pregnant women and explore the characteristics of pregnancy outcomes among older pregnant women through individualized management, thus providing a basis for nutritional guidance in this population of pregnant women.
Methods
Patients and methods
This was a prospective study using a randomized controlled trial design. Older pregnant women admitted to our hospital from August 2017 to May 2018 were randomly divided into a study group and control group (410 women in each group) using a central stochastic system. The control group was given routine pregnancy health education and nutrition guidance; the study group was provided with individualized medical nutrition guidance. We followed the CONSORT Statement (parallel group randomized trials) guidelines for reporting randomized trial studies. All patients signed informed consent forms before enrolling in the study. This study was conducted in accordance with the Declaration of Helsinki and was approved by the ethics committee of Hebei Cangzhou Women and Children’s Health on 20 July 2017 in Cangzhou, Hebei, China.
We erroneously did not prospectively register this trial. However, it is registered retrospectively at the Research Registry (https://www.researchregistry.com/, registration number researchregistry6901).
Individualized medical nutrition guidance during pregnancy
We calculated the total energy intake of each pregnant woman according to their pre-pregnancy BMI. 7 We increased the average daily energy intake by 200 kcal on this basis during the second and third trimester of pregnancy, including 50% to 55% carbohydrate, 25% to 30% fat, and 15% to 20% protein.
As for energy distribution, eating less at each meal and more frequent meals is recommended, that is, three main meals and three additional meals. The recommended energy distribution of six daily meals is 15% to 20% for breakfast, 20% to 30% for lunch, 20% to 30% for dinner, and 15% to 30% for extra meals. 7 The dietary habits and compliance of pregnant women should be fully considered when formulating a diet. Daily total calories = [actual height (cm) − 105] × (2540) kcal/(kg × d). According to the food exchange method, pregnant women in our study were instructed to choose appropriate foods and preparation methods for each meal (including vegetables, fruits, and meat). Pregnant women were instructed to record the foods and food intake at each meal. The volume of foods consumed at each meal, in ascending order, was soup, vegetables, meat, and staple foods. Body weight was measured and recorded each week, and the rate of weight gain and total weight gain during pregnancy were controlled to within a reasonable range. Patients who consumed less than 80% or more than 120% of the prescribed intake were considered to be non-compliant.
Exercise guidance
Appropriate physical activity was to be carried out 15 to 20 minutes after meals, usually involving taking a walk. If women engaged in aerobic activities such as swimming or yoga before pregnancy, it was suggested that these activities can be continued during pregnancy according to their wishes and physical condition. The duration of such activities was to be controlled to within 30 to 40 minutes.
Observation of statistical indicators
Regular check-ups were conducted during pregnancy, with regular measurement of body weight and blood pressure. Weight gain was categorized in the following groups: ≥12 kg, ≥15 kg, and ≥17.5 kg. We compared pregnancy weight gain between the two groups of pregnant women in each trimester. Complications during pregnancy and childbirth included GDM, gestational hypertension, PPH, cesarean delivery, incident macrosomia, newborn birth weight, incident neonatal asphyxia, and neonatal transfer to the neonatal intensive care unit.
In the diagnostic criteria for GDM, we adopted the 2018 American College of Obstetricians and Gynecologists Practice Bulletin. 8 The diagnostic criteria for hypertension during pregnancy followed the 2018 New Zealand Ministry of Health Guidelines for the diagnosis and treatment of hypertension and preeclampsia in pregnancy. 9 The diagnostic criteria for PPH was as follows: within 24 hours after delivery, bleeding volume ≥500 mL with vaginal delivery and ≥1000 mL with cesarean delivery; severe PPH refers to bleeding volume ≥1500 mL within 24 hours after delivery. 10 The diagnostic criteria for macrosomia was a fetus weighing more than 4000 g, regardless of gestational age. 11 We adopted the 2016 expert consensus on the diagnosis of neonatal asphyxia of the Neonatal Resuscitation Group of the Perinatal Medicine Branch of the Chinese Medical Association. 12
Weight gain in the first trimester of pregnancy refers to weight gain from pre-pregnancy to the end of week 13 of pregnancy; weight gain in the second trimester refers to weight gain from the end of the 13th week to the end of week 27 of pregnancy; and weight gain in the third trimester refers to weight gain from the end of week 27 to the end of pregnancy.
Statistical analysis
The data were collected from the hospital information system and sorted using Microsoft Excel 2016. All analyses were performed using SPSS 18.0 (SPSS Inc., Chicago, IL, USA). Measurement data conforming to a normal distribution were analyzed using the χ 2 test. Comparisons between groups were conducted using an independent samples t-test and expressed as mean and standard deviation. Count data were expressed as n (%), and comparisons between groups was conducted using χ2 tests. Statistical significance was set to P < 0.05.
Results
We collected the basic information of 820 older pregnant women and their infants. Maternal age (mean±standard deviation) was 37.5±3.5 years in the intervention group and 38±2.5 years in the control group. There were no differences in basic characteristics between the groups (Table 1). Compared with controls, women in the study group had significantly lower weight gain ≥12.5 kg, ≥15 kg, and ≥17.5 kg, as well as weight gain in the first, second trimester, and third trimester (all P < 0.05) (Table 2).
Basic information of pregnant women and infants.
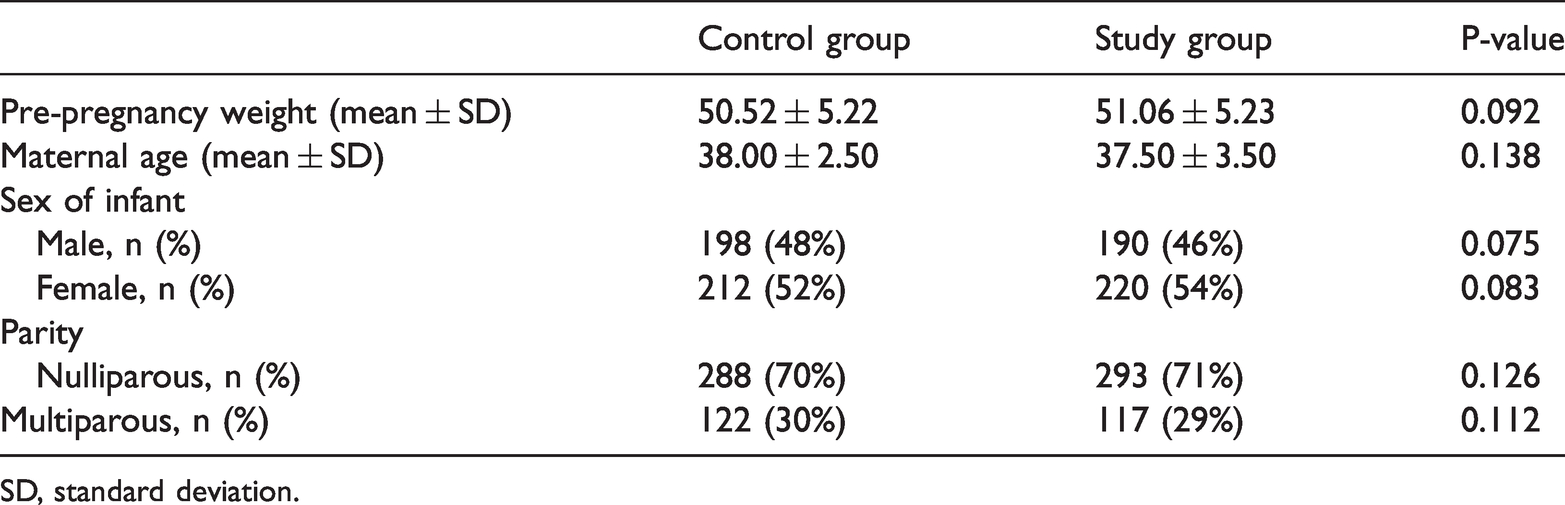
SD, standard deviation.
Changes in weight gain among pregnant women during different pregnancy periods.

SD, standard deviation.
In comparisons of common comorbidities and complications in the perinatal period between the two groups, the incidences of GDM and macrosomia and the rate of vaginal delivery were significantly improved in the study group over those in the control group (all P < 0.05). The incidence of PPH and hypertension showed no significant difference between the two groups (Table 3).
Comparison of the incidence of complications during pregnancy and delivery between groups.

Values in the table are n (%).
GDM, gestational diabetes mellitus.
In a comparison of neonatal complications between the two groups, there was no significant difference in neonatal asphyxia and preterm infants between the groups. However, we found significantly lower incidence of transfer to neonatal intensive care and neonatal hyperbilirubinemia (P < 0.05) in the group that received the intervention (Table 4).
Comparison of neonatal complications between the groups.

NICU, neonatal intensive care unit.
Discussion
In recent years, the number of older pregnant women has increased each year. A large number of studies have shown that the incidence of perinatal complications, delivery risks, and rate of PPH among older women are higher than those of younger women. 13 Vascular endothelial damage during pregnancy becomes aggravated with increased age, resulting in decreased vascular elasticity and increased blood pressure. 14 At the same time, with older maternal age, the body's sensitivity to insulin is also reduced, resulting in glucose metabolism disorders, 15 which can further develop into diabetes. Additionally, with increased maternal age, the function of the pelvis and ligaments is degraded, leading to loss of elasticity in the soft birth canal. These factors all increase the risk of premature rupture of membranes and PPH. 16 In addition to the decline in physical function among older women and increased perinatal complications, many women lack knowledge of nutrition during pregnancy and consume too much food, leading to excessive weight gain during pregnancy, which also increases the incidence of perinatal complications. At present, many hospitals in China have implemented guidelines for proper weight gain during pregnancy. 17 Although the importance of proper weight and weight gain during pregnancy has been recognized, many women are overweight at conception, and many women gain excessive weight during pregnancy.18–20
Complications during pregnancy and childbirth can also lead to various complications in the newborn. Among them, GDM can lead to fetal overnutrition and the occurrence of macrosomia, which increases the incidence of PPH. At the same time, high blood glucose concentrations can increase the body's oxygen consumption and increase the incidence of neonatal asphyxia. Additionally, high blood glucose levels can cause hypoxia, destroy the structure of red blood cells, release a large amount of bilirubin, and cause neonatal jaundice.
In our research, we found that after receiving individualized pregnancy nutrition guidance for older women, weight gain ≥12.5 kg, ≥15 kg, and ≥17.5 kg, as well as weight gain in the first, second, and third trimester of pregnancy and weight gain at delivery in the study group were significantly reduced compared with the control group (P < 0.05). These findings indicate that weight gain can be effectively controlled by providing guidance on diet and exercise for older pregnant women. Further comparative analysis showed that by controlling weight in older pregnant women, the incidence of GDM and macrosomia in the two groups was significantly reduced (P < 0.05). This finding further confirmed that weight gain during pregnancy is related to the incidence of pregnancy complications. 21 A lower incidence of GDM will reduce the incidence of macrosomia; thus, personalized nutrition guidance can significantly reduce the rate of fetal macrosomia. 22 Our study showed that nutritional guidance can reduce the incidence of pregnancy complications. Parity is a known factor in pregnancy complications; the incidence of complications is higher in multiparous woman. In this study, there were more nulliparous than multiparous women, which might be the reason for there being fewer complications and no bleeding complications in our study. However, the difference in parity between the groups was not significant.
In the present study, individualized nutritional interventions for older women reduced the incidence of maternal and neonatal comorbidities and complications to a certain extent; nevertheless, nutritional guidance alone may not be sufficient. It is necessary to strengthen many aspects of monitoring and intervention at the same time. It is recommended that women self-monitor their weight during the entire pregnancy and that clinicians regularly monitor women’s weight during each checkup to detect insufficient or excessive weight gain during pregnancy and take measures to correct it. At the diagnosis of pregnancy or during the first checkup, it should be explained to women that there is no need to increase caloric intake because weekly weight gain in early pregnancy should be minimal. In the second and third trimesters, women who are underweight and normal weight need only gain approximately 300 kcal per day to achieve a weekly weight gain of 500 g. For overweight and obese women, the increase in energy intake should be lower because weight should increase by approximately 250 g each week.
A limitation of this study was that we did not assess the impact of nutritional guidance on other pregnancy complications; further research is needed to explore this issue. The sample size was not calculated in this study; however, we believe that the number of included pregnant women was sufficiently large.
Conclusion
The incidence of perinatal complications and neonatal complications in older pregnant women were significantly higher than those in younger pregnant women. Among the causes of complications in older women, weight gain during pregnancy is relatively easy to control. Studies have shown 15 that personalized nutrition guidance can significantly reduce the rate of macrosomia and improve pregnancy outcomes. Controlling weight gain during pregnancy to within a reasonable range among older parturient women through individualized nutrition guidance can reduce the occurrence of complications during pregnancy and postpartum by promoting feasible and scientifically based dietary structure and standards during pregnancy. This study provides a basis for nutritional guidance during pregnancy targeting older pregnant women.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Medical Science Research Project Plan of Hebei Provincial Health Commission (no. 20181537).