
Abstract
The present study aimed to investigate the association between nutritional status with delayed tooth eruption (DTE). Oral examination was performed in schoolchildren (8-11 years old), and DTE was defined by absence of dental gingival emergence or when primary tooth was still present in the oral cavity after the expected time. BMI z-score of each child were collected and nutritional status was defined. Chi-square test and binary logistic regression adjusted by age and gender were performed. Odds ratio (OR) and 95% Confidence Interval (95% CI) were calculated. The established alpha was 5%. Among 353 included children, 247 were classified as eutrophic, 16 as underweight, 64 as overweight, and 26 as obese. Underweight was associated as a risk factor to DTE (P = .014; OR = 3.5; 95% CI = 1.3-9.8), and underweight girls had more chance to present DTE than eutrophic girls (P = .048; OR = 4.4; 95% CI = 1.1-17.2) in chi square test. In logistic regression, underweight was associated as a risk factor to DTE (OR = 4.21; CI 95% = 1.42-12.43; P = .009). Underweight children have a higher risk of DTE in permanents.
Introduction
Tooth eruption is the axial movement mechanism of the tooth germ from the alveolar bone to a functional occlusion position in the oral cavity. Many factors could affect primary and permanent tooth eruption. Some studies suggested that low birth weight and prematurity,1-4 endocrinology conditions,5-7 ethnicity, 8 socioeconomic aspects, 9 and nutritional status, such as malnourishment (underweight), and obesity,7,10-25 could affect tooth eruption leading to a delay or earlier tooth eruption and primary tooth exfoliation.
Nutrition is a fundamental factor in child’s growth and development. Child malnutrition is still a public-health problem affecting 1 in 12 children worldwide. 26 This condition increases the risk of impairing physical and cognitive development of the child, thus increasing the risk of death from infectious diseases. 26 Overweight and obesity, on the other hand, also are associated with many systemic conditions impacting the child’s health, and have become a public health issue in the past decades due to their high prevalence and comorbities. 27
The relationship between nutritional status and oral health/oral diseases has become one of the most investigated subjects in recent decades. 14 It is not a new concept that nutritional aspect could influence skeletal and dental development.28,29 Studies have shown that calcium, vitamin D, vitamin B, and ascorbic acid deficiency may be related to different forms of periodontal disease.30-33 Malnutrition/underweight can alter the tooth eruption by delaying the exfoliation of primary and the eruption of permanent teeth.10,16,18,21 Obesity can affect the child’s metabolism, leading to an earlier tooth eruption and earlier primary tooth exfoliation.14,15,17
The existing data support that tooth eruption are influenced by the child’s body mass index (BMI). 14 Although the studies demonstrated this association in children from different ethnicity, this association should be evaluated in children form different populations. Therefore, in this cross-sectional study we investigated if nutritional status was associated with delayed tooth eruption (DTE) in a group of Brazilian schoolchildren.
Material and Methods
Ethical Aspects
This cross-sectional study was approved by Human Ethics Committee of Federal University of Alfenas, Brazil (approval number of CAAE 78568217.7.0000.5142). Children’s parents and caregivers signed an informed consent after clarifications about the research. The STROBE guideline was followed to perform this article. 34
Sample Description
This project is a cross-sectional survey was designed as school-based study. The projected included school children age ranging from 8 to 11 years old from 4 public schools from a Brazilian city called Alfenas, in Minas Gerais state, which is located in the Southeast of the country. This sample collection of this project was conducted from February 2018 to May 2018 and is previously described in Barbosa et al. 35
A sample size calculation was performed using an alpha of 5% (α = .05) and a beta of 80% (β = .80) predicted a minimum of 276 children (http://clincalc.com). Only 1 child per family was included to avoid familiar cluster. Children with history of facial trauma, previous or current orthodontic appliance, syndromes, oral cleft, and/or systemic conditions such as endocrinology problems were excluded.
Clinical Examination
All children underwent a clinical oral examination. The oral examinations were inside the schools, under natural light, using cotton rollers, gauze, standard mouth mirrors, and ballpoint probe, according to World Health Organization. 36 The DTE was defined by absence of dental gingival emergence or when primary tooth was still present in the oral cavity after the expected time according to age of teeth exfoliation presented in the “Global child dental fund.” 37 Gingival emergence was defined when any dental face was presented in the alveolar mucosa. 21 Children that presented at least 1 delayed permanent tooth were considered children with DTE. Intra-examiner training and calibration were conducted before the study for clinical parameters. The kappa coefficient was .87. A single trained dentist examined all children while an assistant recorded the clinical findings.
The anthropometric data, height (m), and weight (kg) were recorded on the same day of the oral examination. The heights were assessed and determined in meters and the weights were assessed and determined in kilograms using a weighing machine. The children were wearing light clothes and no shoes. To determine the nutritional status a calculation using the Body Mass Index (BMI) z-score calculator available on line (http://zscore.research.chop.edu/index.php) was performed. The individual children’s height, weight, age, and gender were used as variables in the BMI z-score formula. The classifications were performed according to the World Health Organization 38 as follow: underweight (<3 percentiles), eutrophic (normal weight) (≥3 and ≤85th percentiles), overweight (85th and ≤97th percentiles), and obese (97th percentiles).
Statistical analysis
GraphPad Prism 5.0 (Graph-Pad, San Diego, CA, EUA) was used for statistical analysis and graphical presentation. T-test was used to compare means among “no DTE” and “DTE.” Chi-square were used to compare gender distribution and nutritional status distribution among groups. Odds ratio was also calculated. The analysis of DTE and nutritional status groups was also performed stratified according to the gender. Means and standard deviations (SD) of the number of DTE were compared using 1-way ANOVA with Tukey’s post-test. Binary Logistic Regression adjusted by age in months and gender was also performed. The alpha was 5%.
Results
In this study, 353 children were included, in which 170 (48.16%) were boys and 188 (51.84%) were girls. Girls was associated with higher chance to present DTE in comparison with boys (OR = 1.7; CI 95% 1.1-2.7; P = .015). Mean age was similar among groups (P = .958). Sixteen children (4.53%) were classified as underweight children, 64 (18.13%) as overweight children and 26 (7.36%) as obesity children. The characteristics distribution according to the groups are presented in the Table 1.
Sample Characteristics According to the Groups.

Bold forms means statistical significance difference.
t-test was used.
Chi-square was used.
Underweight children had more than 3 times higher chance to present DTE than normal weight children (P = .014). Underweight girls had more than 4 times higher chance to present DTE than eutrophic girls (P = .048) (Table 2).
Nutritional Status Distribution Among the Groups.
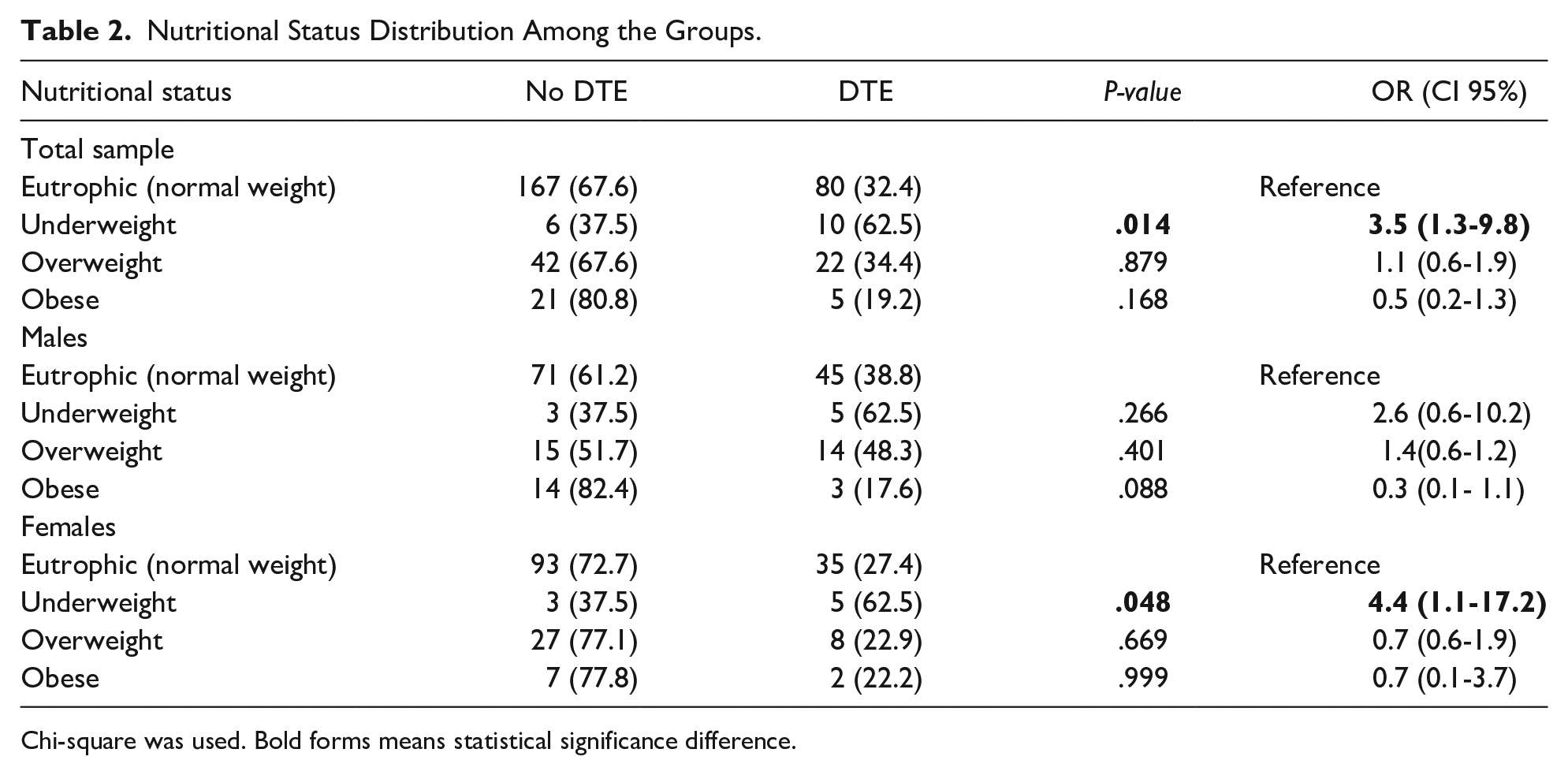
Chi-square was used. Bold forms means statistical significance difference.
Figure 1 presented of mean number of DTE according to the nutritional status. In the eutrophic group, the mean number was 0.89 (SD = 1.64); in the underweight group, the mean number was 1.66 (SD = 1.54); in the overweight group, the mean was 1.14 (SD = 2.0); and in the obese group, the mean was 0.53 (SD = 1.2). A statistically significant difference among the groups were not observed (P = .153).

Number of delayed teeth according to the group.
In the binary logistic regression adjusted by age and gender (Table 3), underweight was associated as a risk factor to DTE (OR = 4.21; CI 95% = 1.42 - 12.43; P = .009).
Binary Logistic Regression.

The model was adjusted by gender and age in months. Bold forms mean statistical significance difference.
Discussion
The complex relationships between systemic health, body composition, BMI, and oral health has been widely explored in dental research in the past years. 14 The current evidence supports that the disturbance in tooth eruption is directly related to the child’s growth, development and nutritional status and should be considered in pediatric patients during dental treatment.10-25 Although the association between permanent tooth eruption (or delayed exfoliation of the primary tooth) was previously investigated in other Brazilian populations,19,20 we also decided to explore the impact of the nutritional status on tooth eruption time in School children from Alfenas, which is a medium size city located in Minas Gerais state. It is important to emphasize that Brazil is a country with a continental size with a different ethnic composition ranging according to the state, 2 as well as socioeconomic and cultural differences. The influence of ethnicity 8 and socioeconomic aspects 9 on tooth eruption have already been documented and suggested. 5
Nutritional status can alter the eruption timing of permanent teeth, which is a highly important process in pediatric dentistry due to its influence on occlusion, caries risk, and timing of preventive and orthodontic intervention. 14 These dental diseases are a costly burden to health care services. Therefore, studies aiming to understand the modifying factors of eruption timing of permanent teeth are of great relevance for the clinicians and public health strategies.
The impact on permanent tooth eruption for children in the extremes of the spectrum of BMI z-scores was noticed by different studies in many populations.10-25 In our study, the logistic regression adjusted by gender and age demonstrate that underweight children had more than 4 times higher chance to present DTE. Underweight and malnourishment were already associated with permanent DTE in children from Cambodia, 10 in Filipino teenagers 21 and was also associated with delayed tooth formation in children and teenagers from South Africa. 12 The affected tooth formation in underweight children due to lack of essential nutrients and the decreased growth hormones can delay the tooth eruption. 39
Adipose tissue is involved in regulating metabolic processes and hormonal regulation. Increase of adipose tissue leads to hormonal changes in obese individuals, increasing secretion of growth factors accelerating tooth eruption. 40 Thus, childhood obesity can change the chronology and time of tooth eruption, causing physical, and psychosocial changes. 22 A study performed in United States of America, teeth of obese children erupted earlier than eutrophic children, 22 a similar result was observed in overweight Mexican children who also had more erupted teeth. 17 Sindelarova et al. 23 observed that specific types of teeth were reported to emerge earlier in obese Czech children. The association between overweight/obesity with tooth eruption was also previously performed in Brazilian children. Evangelista et al. 20 observed that permanent tooth emergence is associated with overweight and obesity in children from the Brazilian Amazon area. Arid et al. 19 also observed similar results in children from São Paulo state, however, in our study, only a borderline result was observed in boys. It is possible that this is a type II error due to the small sample size of obese children. In our sample, 70% of the children eutrophic.
DTE analysis according to gender by chi-square test showed differences among males and females, corroborating with previous studies.1,23,41,42 In addition, in our study, when evaluating the nutritional status impact on the DTE in male and female separately by the chi-square test, we observed an association with underweight and DTE only in females. However, the logistic regression adjusted by gender and age, a multivariate analysis, indicated the impact of the underweight on the DTE regardless of gender, indicate the relevant impact of underweight in both of sexes.
A recent study evaluated panoramic radiographs of Black South African children and teenagers to assess the stages of permanent tooth formation. The authors observed that variations in tooth formation were associated with in the extremes of the spectrum of BMI z-scores. 12 In fact, the lack of radiographic exam is a limitation of our study. Image exams allowed the identification of tooth development stages and possible developmental alterations.
Conclusion
Although the association between DTE and nutritional status was not evidenced in this sample, our results state that girls are at higher risk of DTE compared to boys. In addition, underweight children have a higher risk of DTE in permanents compared to eutrophic children. Such findings suggest further research on nutritional status and its significant effect on DTE.
Footnotes
Authors’ Note
Isabela R. Madalena is also now affiliated to Department of Restorative Dentistry, Federal University of Juiz de Fora, Juiz de Fora, Brazil.
Author Contributions
CR: contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. MB: contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. SH: contributed to interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. IM: drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. DdL: contributed to conception and design; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. MO: contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. EK: contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. DdO: contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Council for Scientific and Technological Development (CNPq).