
Abstract
Background. The COVID-19 pandemic has shed light on communities of racial/ethnic minority groups in the US where long-standing health issues and structural inequities are now known to have resulted in increased risk for infection, severe illness, and death from the virus. The objective of our study was to describe demographic characteristics, clinical presentations, medical interventions and outcomes of pediatric patients with COVID-19 treated at Children’s Hospital of Michigan (CHM), a tertiary care center in urban Detroit, an early hotspot during the initial surge of the SARS-CoV-2 pandemic. Methods. A retrospective chart review was performed of children ≤18 years of age who had polymerase chain reaction (RT-PCR) testing via NP swab or serum IgG antibody testing for SARS-CoV-2 during March 1, 2020–June 30, 2020. Results. Seventy-eight COVID-19 infected children were identified of whom 85.8% (67/78) were from minority populations (African American, Hispanic). Hospitalization rate was 82% (64/78). About 44% (34/78) had an associated comorbidity with asthma and obesity being most common. Although all ages were affected, infants <1 year of age had the highest hospitalization rate (19/64, 30%). In all disease severity categories, dichotomized non-whites had more severe disease by percentage within race/ethnicity than Whites, and also within percent disease severity (P-value = .197). Overall, 37% of hospitalized patients required intensive care. Conclusions. Extremely high rates of COVID-19 hospitalization and requirement of ICU care were identified in our patient population. Further studies are needed to better understand the contributing factors to this health disparity in disadvantaged communities.
Background
Severe acute respiratory syndrome coronavirus 2 (SARS CoV-2) is a respiratory virus of the coronavirus family responsible for the current ongoing global pandemic. On January 30, 2020, the World Health Organization (WHO) declared the novel coronavirus disease (COVID-19) a public health emergency of international concern. On March 30, 2020 the coronavirus outbreak was declared a pandemic. As of April 6, 2021 there were more than 132 million cases of COVID-19 reported worldwide with more than 2.8 million deaths. 1
Current data suggests that children are less affected by this viral pandemic in terms of both number of cases and severity of illness. 2 In a large case study from China (n = 72 314), 3 children <19 years accounted for 2% of cases, with 1.2% in children aged 10 to 19 years and 0.9% in children <10 years old.
According to the State-level data on child COVID-19 cases in the United States (US) provided by the American Academy of Pediatrics and the Children’s Hospital Association, as of January 7, 2021, children represented 12.5% of all COVID-19 cases. Children accounted for 1.2% to 2.8% of total hospitalization with mortality range of 0% to 0.20% of all COVID-19 deaths. 2
Our understanding of the epidemiology and outcomes of COVID-19 infections in children is still limited. A study on the epidemiology of SARS-CoV-2 infection across the US among 135 794 pediatric patients from a network of 7 children’s health systems found SARS-CoV-2 infection overall rate was low (4%), and clinical manifestations were generally mild with a hospitalization rate of 7%. However, this study revealed significant differences in testing and infection rates among children of different racial and ethnic backgrounds. Compared with White patients, minority (African Americans and Hispanics) patients had lower rates of testing; however, they were significantly more likely to have positive test results. 4
Differences in the prevalence and clinical presentation in children can vary based on the region of the country/world. Michigan was one of the nation’s top 3 hotspots for the COVID-19, following New York and New Jersey, in the beginning of the pandemic in March 2020. Nearly half of the cases and deaths in Michigan occurred in Wayne County where the city of Detroit is located. Among communities of racial/ethnic minority groups in the United States, long-standing health issues and structural inequities have resulted in increased risk for infection, severe illness, and death from COVID-19. 5
Therefore, given the extent of the current pandemic, and the regional differences in the prevalence of COVD-19 infection, determination of the number of infections among children in specific regions can add to the existing knowledge as well as reveal crucial information regarding local outbreak control, which can have implications for public health practice. Studies in minority children who are disproportionately affected by this pandemic are needed to help understand and mitigate these disparities while also helping implement outbreak control measures to limit spread of infection specific to these populations.
The objective of our study was to describe the clinical presentation, medical intervention and outcome of pediatric patients with confirmed COVID-19 treated at Children’s Hospital of Michigan (CHM), a tertiary care center in Detroit, during the current SARS-CoV-2 pandemic.
Patients and Methods
We conducted a retrospective chart review of children ≤18 years of age who had a polymerase chain reaction (RT-PCR) testing via nasopharyngeal (NP) swab (Cepheid Inc. Sunnyvale, CA, USA) or serum Immunoglobulin G (IgG) antibody testing for SARS CoV-2 (Abbott Laboratories, Lake Bluff, IL, USA) performed at our institution during March 1st 2020–June 30th, 2020.
Our hospital is an inner city, freestanding children’s hospital with 228 inpatient beds. The Pediatric Emergency Department (ED) is a level 1 trauma center with approximately 85 000 visits annually.
For those patients who had serial laboratory testing and radiographic studies performed, only the first set of test results was included. Testing for viral co-infections was performed at the discretion of the treating physician. For this study, hospitalized children were categorized as COVID-19- hospitalized (children who were admitted to the observation unit or inpatient floor), COVID-19-ICU (children who required intensive care) and Multisystem Inflammatory Syndrome in Children (MIS-C) (children who were treated for MIS-C at our institution whether they were admitted to an inpatient unit or intensive care unit).
Study Definitions
COVID-19 infection: Any patient who tested positive by PCR or IgG antibody for SARS-CoV-2.
Multisystem Inflammatory Syndrome in Children (MIS-C) associated with COVID-19: Centers for Disease Control and Prevention (CDC) case definition 7 was used for categorization of patients as MIS-C.
Severity of Illness: This was categorized based on criteria published by Dong et al 8 as asymptomatic, mild, moderate, severe and critical.
We classified significant interventions as respiratory, cardiovascular and others. Respiratory: high flow oxygen or heliox administration, chest tube placement, positive pressure ventilation, endotracheal intubation Cardiovascular: requirement of ≥3 normal saline boluses, inotropic support, intravenous vasopressors or antiarrhythmic administration, cardiopulmonary resuscitation, cardioversion, need for Extracorporeal Membrane Oxygenation (ECMO) Others: blood product transfusion
Statistical Analyses
Data abstraction was performed by a trained research assistant, systematically coded and entered into a REDCap database. Patient demographic (gender, age), race, clinical data were reported descriptively with proportions, ratios, medians, interquartile ranges, and tables. Where statistical comparisons could be performed on lab value comparisons between groups (acute COVID-19 Pediatric Floor Unit, acute COVID-19 ICU, MIS-C) a non-parametric Kruskal-Wallis test was performed, with pair-wise comparisons utilizing a non-parametric Mann-Whitney U procedure. Statistical significance was considered achieved at a P-value of .05, two-tailed. All statistical procedures were conducted using SPSS Version 26 IBM Inc.
Ethical Approval and Informed Consent
This study was approved by the Wayne State University Institutional Review Board (IRB) with a waiver of informed consent, IRB number 20-04-2115.
Results
During the study period, 1 514 children underwent testing for SARS-CoV-2 of whom 80 (5.3%) tested positive. Of these, 2 patients were over the study age range and hence 78 patients were analyzed. Forty six patients were SARS-CoV-2 PCR positive, 23 had positive SARS-CoV-2 IgG and 9 tested positive for both. The breakdown of the positive test results by week is shown in Figure 1. The highest frequency of positive test results was during the first week in April (22%) which correlated with the peak COVID activity in the community.
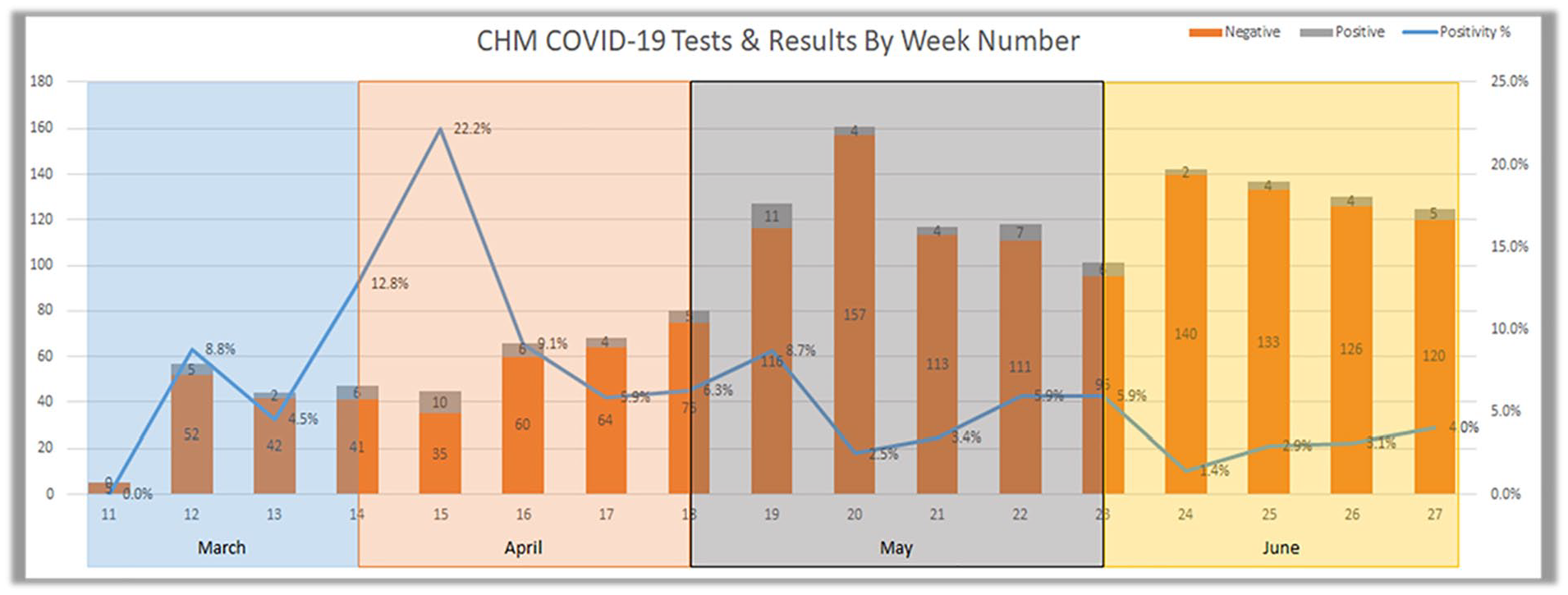
COVID-19 tests and results by week number at our institution (March 1-June 30, 2020).
Clinical characteristics of COVID-19 patients are shown in Table 1. Patients ≤1 year of age (n = 23) accounted for 26.9% of patients, 53.8% were females (n = 42) and majority of our patients were African Americans (57/78; 73%) and 12.8% (10/78) were of Hispanic ethnicity. About 44% of the study cohort (34/78) had an associated comorbidity with asthma and obesity being most common. Fever, cough and vomiting and diarrhea were the most common presenting complaints. There were 7 patients transferred into our center during this time, 4 of these patients were diagnosed with COVID-19 and 4 were diagnosed with MIS-C.
Patient Demographics, Signs and Symptoms of COVID-19 Infection in 78 Children.

The majority (n = 64/78; 82%) required hospital admission with just over one-third (n = 23/64; 36%) of all hospitalized patients requiring Intensive Care Unit (ICU) admission. Among all hospitalized children (n = 64), infants <1 year of age had the highest number of hospitalization (19/64, 30%) followed by children aged 10 to 14 year old (17/64, 27%), then children 5 to 9 year of age (12/64, 19%). The highest proportions of ICU admission was among children 5 to 9 years (7/12; 58.3%) followed by infants (7/19; 36.8%) (Figure 2). Disease Severity in the 78 COVID-19 cases is shown in Figure 3. Though a majority of patients had asymptomatic (23%) or mild to moderate disease (57%), a high proportion (20%) had severe or critical illness. In additional analysis, dichotomized categories of disease severity showed non-whites (Black, Hispanic, Middle Eastern) had more overall severe disease by percentage within race/ethnicity than whites, and also within percent disease severity (P-value = .197) (Figure 4).

COVID 19 disease in children by age group and ED disposition.

Disease severity of 78 COVID-19 cases.
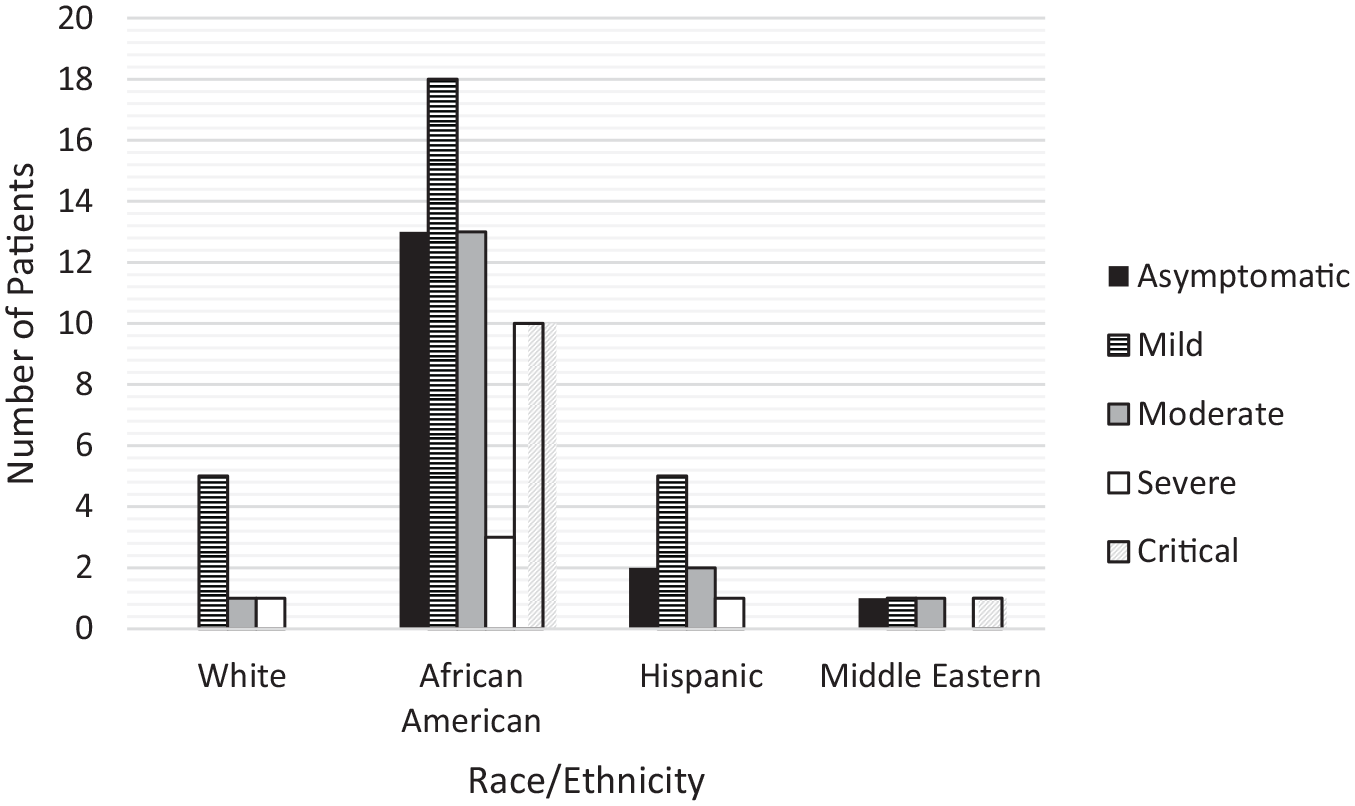
Disease severity of COVID-19 cases by race/ethnicity.
Zip codes were tracked for all participants in the study based on their home address recorded in the EMR. Figure 5a and b show the infection case count (a) and ethnicity/race (b) by zip code, with the Detroit city limits outlined in red.
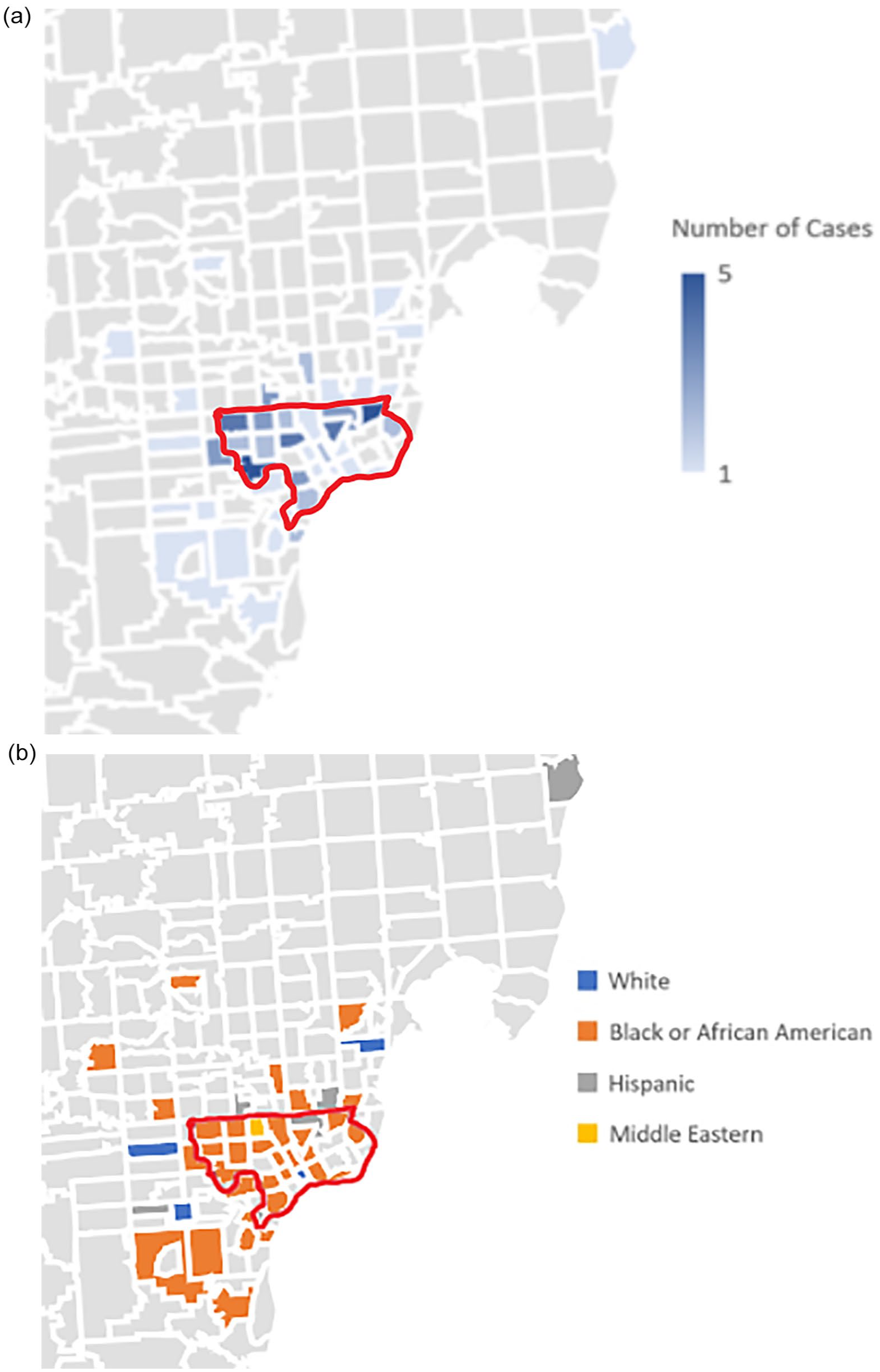
(a) COVID-19 infection cases by zip code and(b) ethnicity/race by zip code.
Pertinent laboratory data based on clinical presentation are shown in Supplemental Table 1: 29 patients had acute COVID-19 with mild presentation; 11 patients had acute COVID-19 disease and were critically ill and needed ICU care; and 21 patients had MIS-C of whom 18 required ICU care.
Patients with MIS-C had a significantly lower absolute lymphocyte count and evidence of systemic inflammation with lower serum sodium and elevated levels of markers of inflammation including fibrinogen, D-dimer, C-Reactive Protein (CRP), ferritin, and Erythrocyte Sedimentation Rate (ESR); they also had evidence of multi-organ involvement (including kidney, heart) with higher serum creatinine and cardiac enzymes (Brain Natriuretic Peptide (BNP), troponin levels) compared to children with acute COVID-19 illness.
Chest radiograph was the most common imaging study performed and the most common abnormalities noted were focal consolidation/opacity (11/53; 20.8%) and pleural effusion (3/53; 5.7%) (Supplemental Table 2). Radiographic abnormalities were more commonly seen in children with COVID-19 compared to those with MIS-C. Computerized Tomography (CT) abdomen was performed and was unremarkable in 3 study patients. No chest CT was performed. Ultrasound of the abdomen was performed in 7 patients with MIS-C and 2 patients with acute COVID-19. Splenomegaly, hepatomegaly and mesenteric lymphadenopathy were noted in 1 patient each, respectively.
Respiratory viral PCR panel was performed in 30 (39%) patients; RSV testing in 11(14.1%) patients; and Influenza A and B testing in 11(14.1%) patients. Viral co-infection was only documented in 2 patients (one with RSV, 1 adenovirus).
Treatment received and length of stay in study cohort are shown in Table 2.
Treatment Received and Length of Stay in Study Cohort.

Abbreviations: BIPAP, bilevel positive airway pressure therapy; COVID, coronavirus disease; CPAP, continuous positive airway pressure therapy; CPR, cardiopulmonary resuscitation; ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; IQR, interquartile range; MIS-C, multisystem inflammatory syndrome in children; O2, oxygen.
The majority of patients with acute COVID-19 in the ICU required respiratory support (7/11, 63%), with 45% (5/11) requiring intubation and mechanical ventilation. On the other hand, cardiovascular support was provided to majority (12/21, 57%) of patients with MIS-C; most of these patients also required vasopressor support due to shock and myocardial dysfunction. Two patients required ECMO support. Majority of patients with MIS-C received Intravenous Immunoglobulin (IVIG) (n = 19, 90%) and aspirin (n = 15, 71%), and 38% (n = 8) received second-line treatment with infliximab. Corticosteroids were used to treat MIS-C in 2 patients. COVID-19 specific therapies included azithromycin (n = 2), hydroxycholoroquine (n = 2) and remdesivir (n = 1).
The median hospital length of stay was the longest (7 days) for patients with MIS-C; 3 days for patients with acute COVID-19 in the ICU; and 2 days for COVID-19 non-ICU patients. No deaths were noted.
Discussion
Michigan is the tenth largest populated state in the US, but since the COVID-19 pandemic began in March 2020, Michigan has had disproportionately high rates of COVID-19 cases and deaths when compared nationally. During the early surge of the pandemic, about a quarter of COVID-19 deaths in Michigan occurred in Detroit. In the first week of November 2020, by CDC’s COVID-19 data tracker, Michigan has the sixth-highest number of cases and the fifth-highest number of deaths nationally. 9 This is likely due to higher rates of social disadvantage and poverty, and higher comorbidities in our population including obesity, diabetes, hypertension, and asthma that makes the population of the city of Detroit more vulnerable to severe COVID-19 disease.10,11 A CDC report found disparities in incidence of COVID-19 among disadvantaged racial/ethnic groups in COVID-19 hotspot regions. 12
However, data on the impact of COVID-19 on vulnerable pediatric patients in urban communities of predominantly African Americans and other minorities are sparse. A study on the hospitalization rates in children with COVID-19 illness found that cumulative COVID-19 hospitalization rate in children <18 years was 8 per 100 000 population, with rates 8 times higher among children of Hispanic ethnicity and 5 times higher in African American children compared to White children. 5 Our study of COVID-19 infection among children of predominantly disadvantaged minority population of African Americans and Hispanics (85.8%, 67/78) showed a very high rate of hospitalization, 82% (64/78)—this up to 10-times the national rate of pediatric COVID-19 hospitalization. 2
Although the majority of children with COVID-19 manifest mild symptoms, some develop significant respiratory disease requiring hospitalization as seen in our cohort. Children can develop a cytokine response similar to that observed in adults with COVID-19 requiring ICU care. In contrast to a previously reported ICU admission rate in children of 1.7% to 16%, 13 our study revealed a much higher rate of 37% of our hospitalized patients requiring ICU care, 45% of whom required intubation and mechanical ventilation. While the reason for the higher rate of hospitalization and ICU care is not clear, it likely reflects medical and socioeconomic factors prevalent in vulnerable communities that increase the risk for severe COVID-19. Nearly one-half of our patients had an underlying co-morbidity, including obesity (62%), asthma (47%), and neurologic abnormality (15%). These co-morbidities have been shown in adult studies to be associated with severe illness and poor outcomes. 14 Similarly, a published report from a large academic health center in the Midwest region of the US indicated African American adults were more likely to become infected with SARS-CoV-2 and experienced more severe COVID-19–associated illness, including hospitalization. 15
In our study, although all age groups were affected, infants <1 year of age had the highest hospitalization rate and higher ICU admission than the other age groups. Infants seem more vulnerable to COVID-19 than other pediatric populations. 16 This is consistent with what has been published in the literature. The Centers for Disease Control and Prevention (CDC) reported 2 572 cases (1.7% of total 149, 082 cases) in patients aged <18 years old as of April 2020. 17 Children <1 year had the highest proportion of hospitalization (15%-62%) and majority (77%) of hospitalized patients had one or more underlying medical conditions. In another analysis from China, of 2143 (confirmed and suspected) cases, 8 children and adolescents accounted for 2% of SARS-CoV-2 hospitalizations, infants had the highest risk of severe disease (10.6%) compared to children aged 11 to 15 years (4.1%) and children >16 years old (3%).
It is challenging to diagnose COVID-19 in infants as manifestations of this illness in this group can be nonspecific, such as poor feeding or diarrhea. 18 Infants can also present with severe symptoms such as fever 16 and sepsis. 19 Due to the spectrum of COVID-19 presentations in infants, which clinically overlap with other infections, there is a heightened risk associated with the medical care of these infants that may be contributing to the higher hospitalization rate.
Initially, it was believed that acute COVID-19 infection in children was generally benign, but there was a sudden change from this notion with the emergence of Multisystem Inflammatory Syndrome in Children (MIS-C). In late April 2020, reports emerged from Italy and the United Kingdom of children with a different clinical syndrome resembling Kawasaki Disease (KD) 20 and later in New York 21 ; many patients had evidence of prior exposure to SARS-CoV-2 infection.
In our study, 21 of 78 patients (27%) presented with symptoms consistent with MIS-C. These patients typically had high inflammation markers (ESR, CRP, ferritin, D-dimer); low lymphocyte count, low serum albumin and sodium, and elevated troponin and BNP levels indicative of cardiac injury. SARS-CoV-2 antibody tests have been reported positive in a greater proportion 18 (86%) of MIS-C patients than PCR testing (43%) indicating a post infectious multisystem inflammatory process in genetically susceptible hosts.
In a study from China of 20 pediatric patients with COVID-19 infection, 22 co-infection with other respiratory pathogens (influenza, respiratory syncytial virus, Mycoplasma pneumoniae) ranged from 5% to 20%. However, co-infection with other viruses and bacteria has been rare in our study population, only seen in 2 patients (adenovirus and RSV). This could be secondary to the low level of testing for respiratory confections in our cohort as well as the study period being in spring and early summer seasons when these respiratory viral infections are less prevalent in our community. 23
There was no COVID-19 related mortality in our cohort likely related to care and treatment received in our hospital. A study evaluating the association of race on all-cause mortality for hospitalized adult patients with COVID-19 found that despite reports that African American patients have a disproportionate share of COVID-19 infections and death, after adjusting for sociodemographic and clinical factors, mortality did not differ between Black and White races for those patients who were able to access hospital care. This suggests the importance of ensuring easy access to health care facilities among high-risk COVID-infected patients. 24
Our study has strengths and limitations. This study examined the epidemiology and characteristics of pediatric patients with COVID-19 disease in Detroit, Michigan during an early surge of the pandemic in the US. Given the disproportionate incidence and severity of COVID 19 illness in racial and ethnic minority communities, further studies are needed to elucidate the reasons for the same. Addressing the pandemic’s disproportionate incidence among racial/ethnic minority communities can help inform, design and implement community specific initiatives thereby leading to improvement of community-wide health outcomes related to COVID-19. The retrospective nature of the study could have limited the information that was available. SARS-CoV-2 testing was not performed in all patients and antibody testing was performed in only a few patients of the cohort. Laboratory and radiographic investigations were not performed in all study patients and for those who had serial investigations performed, only the first set of results was analyzed. Respiratory viral panel was performed only in a little over one-third of patients which limits our ability to draw meaningful conclusions on co-infection. Though our institution had specific guidelines for performance of SARS-CoV-2 testing, it was preferentially performed in patients requiring hospitalization. This could have underestimated the number of patients with an asymptomatic or mild illness. In addition, majority of our patients were African Americans who have been shown to have a higher morbidity and mortality from COVID-19. Furthermore, children with MIS-C were included to illustrate the spectrum of COVID-19 illness in children. These could have resulted in a higher proportion of our cohort with severe and critical illness. This was a single institutional study with a small sample size. These study results may not be generalizable to other settings and areas with different prevalence of SARS CoV-2.
In summary, our findings illustrate the burden of pediatric COVID-19 disease in our region. Our cohort consisted predominantly of disadvantaged racial/ethnic groups of children from a national COVID-19 hotspot. Although the majority of children with COVID-19 had a mild disease, a significant proportion had severe and critical illness requiring hospitalization and critical care. COVID-19 highlights existing health inequities. More studies are needed in racial and ethnic minorities to better understand the disproportionately severe impact of COVID-19 in these communities. Working with leaders in our community to develop targeted interventions within disadvantaged minority populations may help to reduce disparities in COVID-19 incidence and impact.
Supplemental Material
sj-pdf-1-gph-10.1177_2333794X211022710 – Supplemental material for COVID-19 among Minority Children in Detroit, Michigan during the Early National Surge of the Pandemic
Supplemental material, sj-pdf-1-gph-10.1177_2333794X211022710 for COVID-19 among Minority Children in Detroit, Michigan during the Early National Surge of the Pandemic by Jocelyn Y. Ang, Nirupama Kannikeswaran, Katherine Parker, Eric McGrath, Nahed Abdel-Haq, Harbir Arora, Jorge L. Lua, Ronald Thomas, Hossein Salimnia, Teena Chopra, Tommy Tran and Basim Asmar in Global Pediatric Health
Supplemental Material
sj-pdf-2-gph-10.1177_2333794X211022710 – Supplemental material for COVID-19 among Minority Children in Detroit, Michigan during the Early National Surge of the Pandemic
Supplemental material, sj-pdf-2-gph-10.1177_2333794X211022710 for COVID-19 among Minority Children in Detroit, Michigan during the Early National Surge of the Pandemic by Jocelyn Y. Ang, Nirupama Kannikeswaran, Katherine Parker, Eric McGrath, Nahed Abdel-Haq, Harbir Arora, Jorge L. Lua, Ronald Thomas, Hossein Salimnia, Teena Chopra, Tommy Tran and Basim Asmar in Global Pediatric Health
Footnotes
Acknowledgements
The authors with to thank the patients and their families.
Author Contributions
NK, JL, JA, NA, HA, EM and BA: Clinically cared for these patients.
HS: Provided laboratory assistance and consult toward the clinical care of the patients.
JA and KP: Worked on data abstraction and early analysis.
JA, RT, TT, TC, EM: Completed the statistical analysis or requested critical additional analyses.
All authors participated in writing the early drafts, critically revised, reviewed, and finally approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Keypoints
The COVID-19 pandemic has disproportionately impacted racial/ethnic minority groups. Our pediatric patients consisted of underrepresented minority population (African American, Hispanic), and had a hospitalization rate 25 times the national average with over 1/3 of those hospitalized requiring critical care.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.