
Abstract
Background:
Neural tube defects are a major public health problem and substantially contribute to morbidity and mortality, particularly in low-income countries, including Ethiopia. There are a paucity of data on the magnitude and associated factors of neural tube defects in Ethiopia, particularly in the study setting.
Objective:
This study aimed to assess the magnitude of neural tube defects and associated factors among neonates admitted to the neonatal intensive care unit in Hiwot Fana Specialized University Hospital, Harar, Ethiopia.
Methods:
A hospital-based cross-sectional study was employed from October 2019 to January 2020. A total of 420 newborn-mother pairs were included consecutively. Data were collected using a face-to-face interviewer-administered questionnaire and clinical examination. Data were entered into Epi Data version 3.1 and analyzed using the statistical package for Social Sciences version 20.0 software. An adjusted odds ratio (AOR) with 95% confidence interval (CI) was used to identify the associated factors. A p-value <.05 was considered statistically significant.
Results:
The magnitude of neural tube defects was 5.71% (95% CI: 3.5-7.9). Approximately 83.5% of infants had spinal bifida and 16.5% anencephaly. In multivariable logistic regression analyses, preterm birth (32-34 weeks) (AOR= 3.84; 95% CI: 2.1,10.7), low birth weight (1000-1500 g) (AOR = 4.74; 95% CI: 1.8, 9.1), 1500-2500 g (AOR = 3.01; 95% CI: 2. 1, 13.2), maternal coffee consumption (AOR = 11.2; 95% CI: 3.1, 23.7), a history of abortion or stillbirth (AOR = 9.6; 95% CI:7.6,19.4), radiation exposure (AOR = 5.0; 95% CI:1.6,14.3), and intake of anticonvulsant drugs during pregnancy (AOR = 4.75; 95% CI: 1.5,16.2) were factors associated with neural tube defects.
Conclusion:
In this study, the burden of neural tube defects was 5.71% among neonates admitted to the neonatal intensive care unit, which was a public health concern. Increased attention to the monitoring of neural tube defects in eastern Ethiopia is crucial to improve birth outcomes in the study setting.
Background
Neural tube closure is critical for the formation of the human brain and spinal cord. 1 Neural tube defects (NTDs) are complex congenital malformations of the central nervous system resulting from the failure of neural tube closure during embryogenesis.2,3 NTDs can be classified as “open” NTDs in which neural tissue is exposed and “closed” NTDs with neural tissue covered by tissue.4,5
Worldwide, approximately 300 000 babies are born with NTDs each year, resulting in 88 000 deaths and 8.6 million disability-adjusted life years. 6 The incidence of NTDs ranges from 5.2 to 75.4 per 10 000 births in Africa.7,8 This translates into approximately 190 000 neonates who are born each year with NTDs in low- and middle-income countries (LMICs). The consequences of NTDs are more serious in LMICs, where preventative measures and long-term quality care for surviving NTDs patients are limited. 9
In Ethiopia, the prevalence of NTDs is 63.4 per 10 000 births, 17.3, 3.5, and 40 for anencephaly, encephalocele, and spinal Bifida cases per 10 000 births, respectively.3,10 NTDs are important determinants of perinatal morbidity and mortality. 11 Many surviving children have multiple lifelong disabilities and face many significant impacts on physical, social, neurocognitive, emotional, self-esteem, psychological, and economic problems.2,6,12-16 The impact of disabling malformations is more severe especially in Sub-Saharan Africa because of limited rehabilitative services in the region. 17
The specific cause of NTDs remains unknown; however, some cases are influenced by genetic and environmental risk factors. In terms of genetic underpinnings, monozygotic twinning and single-gene disorders have long been associated with NTDs. 18 Numerous studies have explored a variety of candidate gene pathways, such as the folate/1-methyl carbon metabolic pathway, glucose metabolism/transport DNA repair, and oxidative stress pathway retinoic acid receptors. In addition, there are potentially preventable causes, such as environmental influences such as parental occupation, socioeconomic status, maternal use of anticonvulsants (AEDs), lack of routine folic acid supplementation, poverty, maternal nutritional status, and exposure to cigarette smoke, also have contributed to the occurrence of NTDs.4,14,19-21
The World Health Organization (WHO) recommends a daily folic acid intake of 0.4 mg taken at least a month before and in the first trimester of pregnancy.22-24 Adequate use of folic acid reduces the incidence of NTDs when taken before conception.22-28 For instance, in the United Kingdom, after periconceptional folic acid supplementation policy initiatives, the prevalence of NTDs declined from 45 in 1980 to 10 to 15 per 10 000 in the 1990s. 29 Folate is a water-soluble vitamin B that is found naturally in foods, such as fruits, dark green vegetables, potatoes, beans, and yeast extract. Folic acid is the synthetic form of folate found in dietary supplements. There are 3 potential approaches for the delivery of folic acid to the general population: improvement of dietary habits, fortification of food, and use of supplements.4,19,30-32
Improved access and coordination of care in antenatal, perioperative, and rehabilitative services in long-term settings are vital to reduce morbidity and mortality.5,15,33,34 Moreover, identifying intervention targets and offering valuable input to the systematic development of prevention strategies is a crucial component of the effort to minimize the consequences of birth defects. 35
Despite the abovementioned burden of NTDs, studies that assess the magnitude and their associated factors are limited in Ethiopia, particularly in the study setting. The need for greater NTDs surveillance efforts, especially in lower-income countries, is crucial.8,9 Therefore, this study aimed to assess the magnitude of neural tube defects and associated factors among neonates admitted to the neonatal intensive care unit (NICU) in Hiwot Fana Specialized University Hospital (HFSUH) Harar, Ethiopia.
Methods and Materials
Study Area and Period
This study was conducted in HFSUH, which is found in the Harari region, eastern Ethiopia. Harar is located 525 km from Addis Ababa, Ethiopia. HFSUH is a teaching hospital and used as a referral center for the population of eastern Ethiopia. This hospital serves populations with diverse demographic and economic and health characteristics. It provides 24-hour care for the referred representative population. The Department of Pediatrics has 6 units: the pediatric intensive care unit, ward, nutritional rehabilitation unit, NICU, outpatient department, the chronic follow up and including pediatric neurosurgical care facilities. The study was conducted from October 2019 to January 2020.
Study Design and Population
Hospital-based cross-sectional study design was used. All newborn-mother pair admitted to the NICU during the study period were included. However, newborns whose mothers were not available were excluded
Sample Size Determination and Sampling Techniques
The minimum sample size was calculated using double population proportion formula using Statcalc of Epi Info statistical software Version 7 at a 95% confidence level, power of 80%, and an assumption of the ratio of unexposed to exposed equivalent to 1. Using double population formula:
Data Collection Instruments and Procedures
Data were collected using a structured questionnaire adapted from previous literature.17,36-39 The questionnaire was first prepared in English and then translated into local languages (Amharic and Afan Oromo) and back into English for consistency by different language experts. Data were collected by 2 neonatal nurses and 2 pediatricians using face-to-face interviews with maternally related variables (sociodemographic characteristics, labor and delivery-related factors, obstetric and maternal lifestyle, and clinical symptoms of newborns) and physical examination of the newborn by a pediatrician and a thorough review of medical records to obtain birth weight and condition of the newborn before admission. We defined radiation exposure simply by asking the mothers exposures to radiation, such as from a diagnostic medical examination or therapeutic use. Significant caffeine intake was measured as more than 3 cups/day. 40 Alcohol intake during pregnancy: any amount and any time during pregnancy is dangerous for the baby. 41 Consanguineous: marriage between first or second cousin. 42 Maternal smoking during pregnancy was determined based on mothers self-report and was defined as the a “smoker” if she smoked at least 1 cigarettes per day during pregnancy; a “passive” smoker if she was closely exposed to tobacco smoke by people such as her husband, family members, and co-workers. 43
Data Quality Control
Although the data collectors were familiar with all the information in the data collection instrument, refreshment training was given for 1 day before the data collection. The data collection instrument was pretested in Jugal Hospital with 5% (21) of the total sample size. The necessary modifications and corrections were made to the tool before being administered into the actual data collection. The pretested questionnaires were not used in the main data. Double data entry was performed by 2 independent data entry workers.
Data Processing and Analysis
The data were coded and entered into Epi Data version 3.1 and analyzed using SPSS version 20.0 for analysis. A bivariate logistic regression analysis was performed to select the variables to be entered into the final logistic multivariable analysis. Explanatory variables with p-values less than .20 in the bivariate logistic regression analysis were entered into the multivariable logistic regression analysis model, and the associated factors with NTDs were assessed using an adjusted odds ratio at a 95% confidence interval. The statistical value of p < .05 was used to declare statistically significant.
Ethical Approval and Informed Consent
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee in the College of Health and Medical Sciences, Haramaya University (Ref. No. IHRERC/167/2019). Following approval, a written official letter of cooperation was given to the hospital administration. Informed written consent was obtained from all mothers of the newborns. Furthermore, confidentiality was assured throughout the process.
Results
Maternal Sociodemographic Characteristics
Among the 420 mother-newborn pairs requested, all participated in the study, with a response rate of 100%. The mean (±SD) age of the mothers was 23 (±5) years. Of the mothers who participated in the study, 414 (98.6%) were married, and 265 (63.0%) were from rural residents. Two hundred ten (50.0%) had monthly incomes ranging from 2500 to 5000 Ethiopian Birr. Among all newborns, 223 (53.1%) and 197 (46.9%) were female and male, respectively. Regarding gestational age, 291 (69.3%) were 37 to 42 weeks, followed by 110 (26.2%) 34 to 36 weeks. Three hundred and sixteen (75.2%) newborns had normal birth weights (2500-4000 grams), followed by 1500 to 2500 g (19.3%) and 1000 to 1500 g (5.5%) (Table 1).
Sociodemographic Characteristics of Mother-Newborn Pairs Who Admitted to the NICU in HFSUH eastern Ethiopia From October 2019 to January 2020 (n = 420).

Perinatal and Behavioral Characteristics
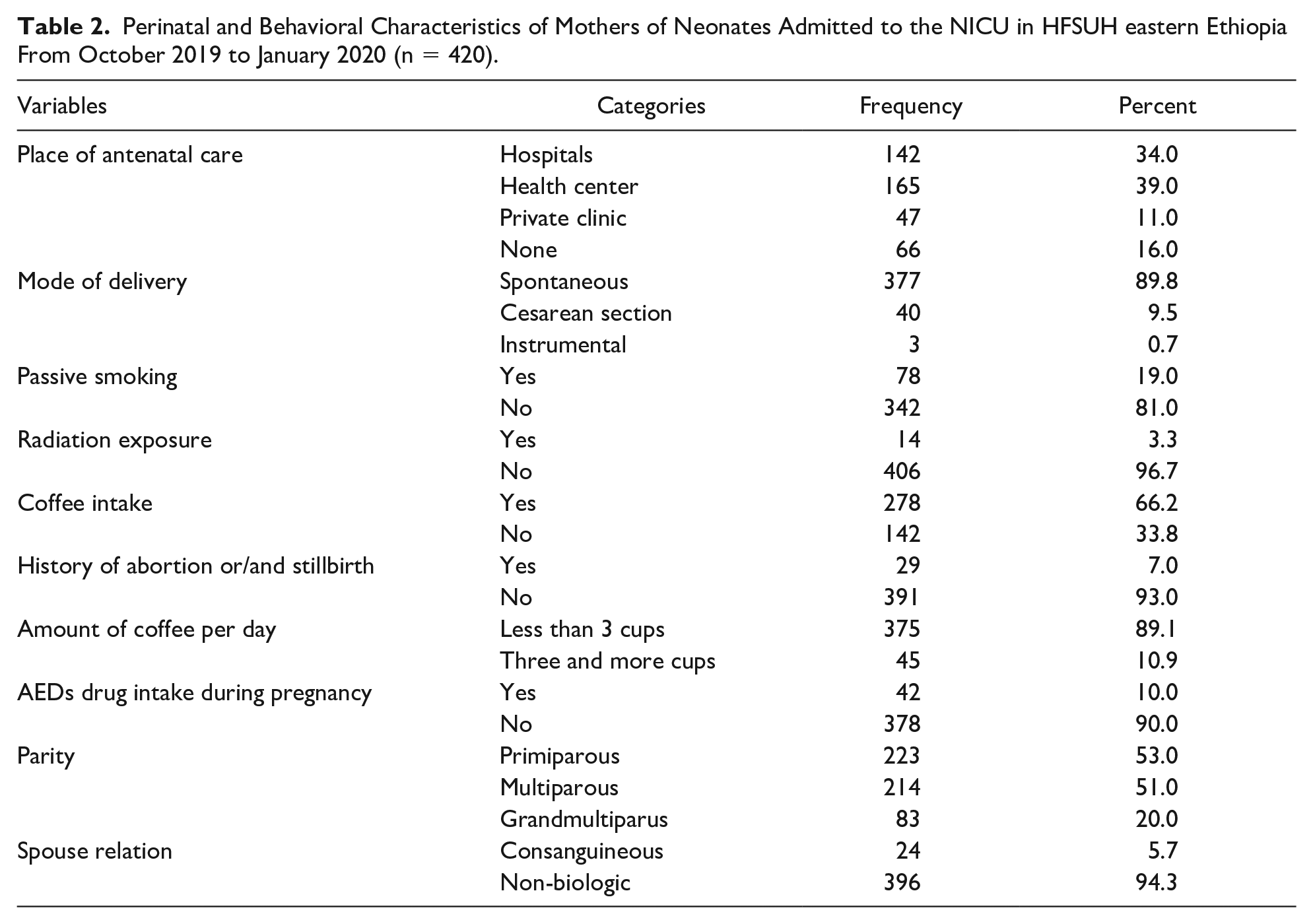
Regarding perinatal care, 354 (84%) had at least 1 antenatal care visit, only 21 (5.0%) participants took folate supplementation, a month before, and during the first trimester of pregnancy, 314 (75.0%) participants had taken folate but not at the recommended time. Moreover, 85 (20.0%) did not take any folate during the current pregnancy. However, 184 (43.8%) of mothers were delivered in health facilities. Only 40 newborns (9.5%) were delivered by cesarean section, and 3 (0.71%) were delivered by instrumental delivery 214 (51.0%) mothers were multiparous. Twenty-nine (7.0%) mothers had a history of abortion or stillbirth. Two hundred seventy-eight (66.2%) mothers of the newborn were coffee drinkers. Twenty four (5.7%) relation were consanguineous. Concerning AEDs Drug intake during pregnancy, 42 (10.0%) were known clients with AEDs. Seventy-eight (19.0%) mothers were exposed to passive smoking. However, none of the mothers were active smokers (Table 2).
Perinatal and Behavioral Characteristics of Mothers of Neonates Admitted to the NICU in HFSUH eastern Ethiopia From October 2019 to January 2020 (n = 420).
Magnitude of Neural Tube Defects
Out of the 420 admitted newborns, 24 (10 male and 14 female) infants had NTDs. The overall magnitude of NTDs was 5.71% (95% CI: 3.5-7.9). Of them, 20 (83.5%) and 4 (16.5%) had spinal Bifida and encephalocele, respectively. Anatomical location of the Spina Bifida cases was thoracic 8 (40.0%), thoracolumbar 10 (50.0%), and lumbar 2 (10.0%), respectively. The clinical characteristics of the observed spinal bifida were 13 (65.0%) cystic, 5 (25.0%) epitheloid, and 2 (10.0%) purulent. The most associated anomalies were 12 (50.0%) hydrocephalus, 4 (16.7%) clubfoot, and 4 (16.7%) a combination of hydrocephalus and clubfoot. Babies affected with NTDs had distorted neonatal reflexes, such as 4 (16.6%) suckling reflexes, 8 (33.3%) grasping reflexes, and 10 (41.7%) moro reflexes in the general neurological examination (Table 3).
Physical Examination of Newborns Admitted NTDs to the NICU in HFSUH eastern Ethiopia From October 2019 to January 2020 (n = 24).

Factors Associated with Neural Tube Defects
In bivariable logistic regression analyses, gestational age, birth weight, AEDs intake during pregnancy, antenatal care visits, history of abortion or stillbirth, radiation exposure, place of residence, exposure to cigarette smoking, and coffee drinking habits of mothers were significantly associated with NTDs. However, in multivariable logistic regression analyses, only gestational age at birth, birth weight, AEDs intake during pregnancy, history of abortion or stillbirth, radiation exposure, and coffee drinking habits were statistically significant factors associated with NTDs. Preterm newborns (less than 34 weeks) (AOR = 3.84; 95% CI: 2.1,10.7) were almost 4 times more likely to be affected by NTDs, whereas gestational age (34-36 weeks) was approximately 83% (AOR = 0.17; 95% CI: 0.1, 0.9) had a less likely risk of NTDs compared to the neonate at 37 to 42 weeks. The low birth weight newborns (1000-1500 g) were nearly 5 times (AOR= 4.74; 95% CI: 1.8, 9.1) and 1500 to 2500 g were 3 times (AOR= 3.01; 95% CI: 2.1, 13.2) more likely to have NTDs compared to the normal birth weight (2500-4000 g) infants. Newborn whose mothers took coffee 3 or more cups per day were eleven times (AOR= 11.2; 95% CI: 3.1, 23.7), and mothers with a history of stillbirth or abortion were nearly 10 times (AOR= 9.6; 95% CI: 7.6, 19.4) more likely to have NTDs compared with their counterparts. Furthermore, mothers with radiation exposure were 5 times (AOR= 5.01; 95% CI: 1.6, 14.3) and took the AEDs during pregnancy were almost 5 times (AOR= 4.75; 95% CI: 1.5, 16.2) more likely to develop NTDs compared to their counterparts (Table 4).
Bivariate and Multivariable Analysis of Factors Associated with NTDs Among Newborns Admitted to the NICU in HFSUH eastern Ethiopia From October 2019 to January 2020 (n = 420).

Abbreviations: COR, crude odds ratio; AOR, adjusted odds ratio; CI, confidence interval.
Significant at ** =
Discussion
Newborn with NTDs present a challenge worldwide and substantially contribute to morbidity and mortality.11,13,44 There are 19 420 deliveries at the facilities in the catchment area of the hospital, with 24 cases of neural tube defects, thus giving a prevalence of 12.4 per 10 000 births. The overall magnitude of NTDs was 5.71% (95% CI: 3.5-7.9) among newborns admitted to the NICU in HFSUH eastern Ethiopia. This is comparable to studies in African countries by WHO, 11.7 per 10 000 births, 8 and in Ghana 44 (5.8%), Iraqi 45 (5.59%), Riyadh, Saudi Arabia 46 (1.2 per 1000), and Iran 47 (2.33 per 1000) births. However, this finding is lower than studies in the systematic review of Globe 13 (18.6 per 10 000), Ethiopia (63.3 cases per 10 000), 10 Addis Ababa, Ethiopia 3 (126 per 10 000), Brazil 11 (4.73 per 1000), and Nigeria38,48 (2.75 per 1000) births. The possible explanation for this variation might be related to methodological and coverage gaps in data collection, 8 nutritional and socioeconomic factors, and the latter study included both live birth and stillbirth in the domains. Approximately 80% of mothers of the newborn received folic acid supplementation in the present study. Moreover, it might be related to the absence of folic acid supplementation or fortification of foods in national NTDs prevention programs in various countries. Regarding folate supplementation, only 5.0% took folic acid a month before, and during the first trimester of pregnancy, 75.0% of participants had taken folate but not at the recommended time. Moreover, 20.0% did not take any folate during the current pregnancy.
The exact cause of NTDs remains undefined. Understanding the genetic and environmental factors is important to reduce the incidence and improve the outcome. 18 In the present study, the factors associated with NTDs were identified by multivariable logistic regression analysis. Accordingly, preterm birth, birth weight, AEDs during pregnancy, radiation exposure, history of abortion or stillbirth, and coffee drinking habits of mothers were factors contributing to the occurrence of NTDs. The risk of having a newborn with NTDs was found to be ten times higher when mothers had a previous history of abortion or stillbirth. This finding is supported by studies in China, 21 Saudi Arabia, 46 Central and Northern Ethiopia,3,49, and Iran. 47 This is because many spontaneous abortions or premature stillbirths occur as a result of congenital defects that might be related to chromosomal abnormalities.
The present finding indicated that mothers who were exposed to radiation were 5 times more likely to had children with NTDs, supported by findings in Turkey 20 and China. 21 However, this should be seen cautiously as it is compared with a trial on mice. 50 Furthermore, maternal AEDs intake during pregnancy was approximately 5 times more likely to have a newborn with NTDs, which is supported by findings in Ethiopia 51 and the Netherlands. 52 The use of AEDs increases the risk of spinal bifida, especially if used during the first trimester of pregnancy.
Moreover, newborns whose mothers consumed coffee (3 or more cups per day) were more likely to have infants with NTDs, which is supported by studies conducted in Ethiopia 53 and Italy. 40 In an animal-based experimental study done in Singapore, they employed early chick embryos as a developmental model to assess the effects of caffeine on the development of the fetal nervous system in which administration of caffeine led to defective neural tube closures and expression of several abnormal morphological phenotypes, which included thickening of the cephalic mesenchymal tissues and scattering of somites. Furthermore, the number of neurons expressing neurofilaments and the degree of neuronal branching were both significantly reduced following caffeine administration. 54 In the present study, preterm babies (<37 weeks) and low birth weight infants (<2500 g) were 4 to 5 times more likely to be affected by NTDs. This finding is supported by studies in Brazil, 11 Ghana, 44 and Addis Ababa, Ethiopia. 3
The possible limitation of the study was related to the study design, the cross-sectional nature of the study does not confirm a definitive cause-and-effect relationship. In addition, the sample size was relatively small, which reduces the statistical power and generalizability of the results. Since it is a hospital-based study and considers only admitted newborns, it not representative of the general population.
Conclusion
In this study, the burden of neural tube defects was 5.71% among neonates admitted to the neonatal intensive care unit, which was a public health concern. It is preventable if mandatory fortification of foods with folic acid is initiated before conception. Gestational age and birth weight, AEDs intake during pregnancy, history of abortion or stillbirth, radiation exposure, and coffee drinking habits were factors associated with NTDs. Increased pregnant mothers’ awareness of timely initiation of antenatal care is recommended since the abovementioned factors would be addressed during this care. Increased attention to monitoring NTDs in eastern Ethiopia is crucial. This study highlights the urgent need for further interventional studies to develop innovative solutions to improve outcomes in the study settings.
Footnotes
Acknowledgements
The authors thank Haramaya University for funding this study as well as participants, data collectors, and staff of all hospitals, without them; this research would not have been realized.
Authors’ contribution
All authors made substantial contributions to the study design and development of the data collection tools. All authors were also involved in data acquisition, analysis, interpretation, and write up. AD drafted the manuscript and prepared the final version for publication. All authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclose receipt of financial support from Haramaya University, Ethiopia.
Consent for publication
Not applicable
Availability of data and materials
All the data of this study are available from the corresponding author upon reasonable request.