
Abstract
This narrative review presents the emerging published evidence on the existence of a phenotypic behavior in children with fetal alcohol spectrum behavior. Such a phenotype, exhibiting high sensitivity, specificity, and predictive values, may assist clinicians and families in identifying children who often miss some of the information needed for full diagnosis, but who may benefit from these screening tools in mobilizing help to these youngsters and their families.
Keywords
Introduction
The diagnosis of fetal alcohol spectrum disorder (FASD) is often very challenging, as it necessitates a history of maternal drinking, evidence of in utero and postnatal growth restriction, evidence of different domains of brain dysfunction, and pathognomonic facial changes (Figure 1). The presence of the typical triad of facial dysmorphology (flat upper lip, flat philtrum, and small palpebral fissures than the third percentile) can obviate the need for clear history of maternal drinking.1,2 However, there are numerous cases without clear evidence of maternal drinking and with no pathognomonic facial changes. These children will often not receive FASD diagnosis and will stay undiagnosed and hence not optimally managed.

The typical pathognomonic triad facial dysmorphology: flat upper lip, flat philtrum, and small palpebral fissures below the third percentile.
Because FASD is characterized by a complex neurobehavioral deficit, a majority of FASD children exhibit disruptive behaviors, including aggression, impulsivity, rule breaking, and asocial behavior, to mention a few. 3 Hence, since almost all the first diagnoses were presented in the early 1970s, efforts have commenced to define a behavioral phenotype to help in the diagnosis. The following statements have been made and are familiar to clinicians diagnosing and managing these children:
“Children with FASD tend to lack conscience, guilt, and remorse after misbehaving.”
“They tend to be cruel.” However, beyond the general statement of a “generalized deficit in processing complex information,” 4 there were no measures to quantify these impressions.
The objective of the present study was to review attempts at identifying a behavioral phenotype of FASD that may help clinicians screen children potentially afflicted by in utero alcohol exposure, with focus on predicting FASD in cases where maternal alcohol exposure cannot be substantiated, and/or when pathognomonic changes in facial morphology are not apparent.
Methods
We conducted a narrative review, focusing on studies that linked specific behavioral measures with the diagnosis of FASD. Searching PubMed, MBASE, Google Scholar, and Cochrane databases from inception to July 1, 2019, we identified articles in any language focusing on human studies that measured behavioral outcome and its correlation to in utero alcohol exposure and signs of FASD. Animal studies, reviews, letters to the editor, or meeting abstracts were not included.
Ethical Approval and Informed Consent
Ethics approval or informed consent was not needed, because this is merely a review of the published literature.
Results
Out of 124 titles suggesting linkage of measures of neurobehavior and fetal alcohol behaviors, the vast majority did not present data that could be used to predict statistically a link between child behavior and fetal alcohol exposure.
Altogether, 2 research groups focused on such links.
Streissguth, Seattle, WA
The pioneering scientist in exploring and defining a phenotypic behavior for FAS was Seattle’s Ann Streissguth in her work on the Personal Behavioral Checklist. Her aim was to develop a scale that describes the essence of fetal alcohol syndrome (FAS) and fetal alcohol effects (FAEs). 5 In 1998, her team presented a list consisting of 68 items that were endorsed by clinicians and parents managing children with FAS or FAE. The most frequently endorsed items were impulsivity (>85%) and stubbornness (>85%). Some of the other highly endorsed items are listed in Table 1.
Behavioral Characteristics That Were Commonly Endorsed by Clinicians and Parents Managing Children With FAS or FAE.

Abbreviations: FAS, fetal alcohol syndrome; FAE, fetal alcohol effect.
Streissguth’s study sample included 472 patients diagnosed with FAS or FAE between the ages of 2 and 51 years. The Fetal Alcohol Behavioral Scale (FABS) exhibited high item-to-scale reliability (Cronbach α of 0.91) and good test-retest reliability (r = 0.69). The FABS was able to correctly identify many of the children in detection studies from both prison and general populations. While the FABS predicted dependent living, as hoped by the researchers it did not correlate with IQ, sex, age, or race. While the authors outline areas of further work needed “to define the specificity and utility of this FABS,” we cannot find published evidence in the ensuing 20 years, and there have not been published studies utilizing the FABS to identify FASD children based on their behavioral scores.
Rovet, Toronto, Canada: The Neurobehavioral Screening Test (NST)
In Toronto, Canada, child psychologist Joanne Rovet and her colleagues have tried to address the effort to describe an FASD phenotype by utilizing Achenbach’s Child Behavior Checklist (CBCL). This validated scale has been used in the diagnosis of FASD in a large cohort of children. Hence, it has provided the researchers an opportunity to examine the predictive value of items from the CBCL. 6
Achenbach’s Child Behavior Checklist 7
This battery of tests aims at children 6 to 18 years of age. 7 It consists of 113 questions, scored on a 3-point Likert-type scale (0 = absent, 1 = occurs sometimes, 2 = occurs often).
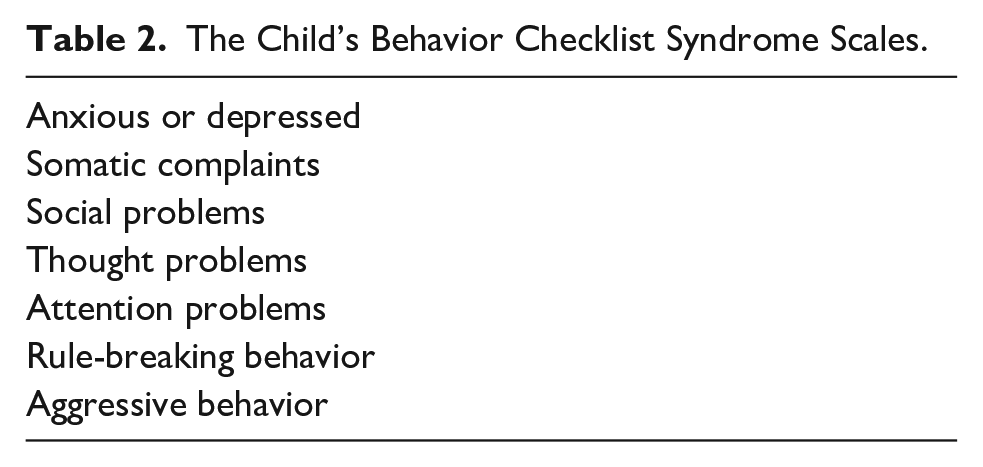
Using the 2001 version of the revised CBCL, the scoring system identifies several syndrome scales (Table 2).
The Child’s Behavior Checklist Syndrome Scales.
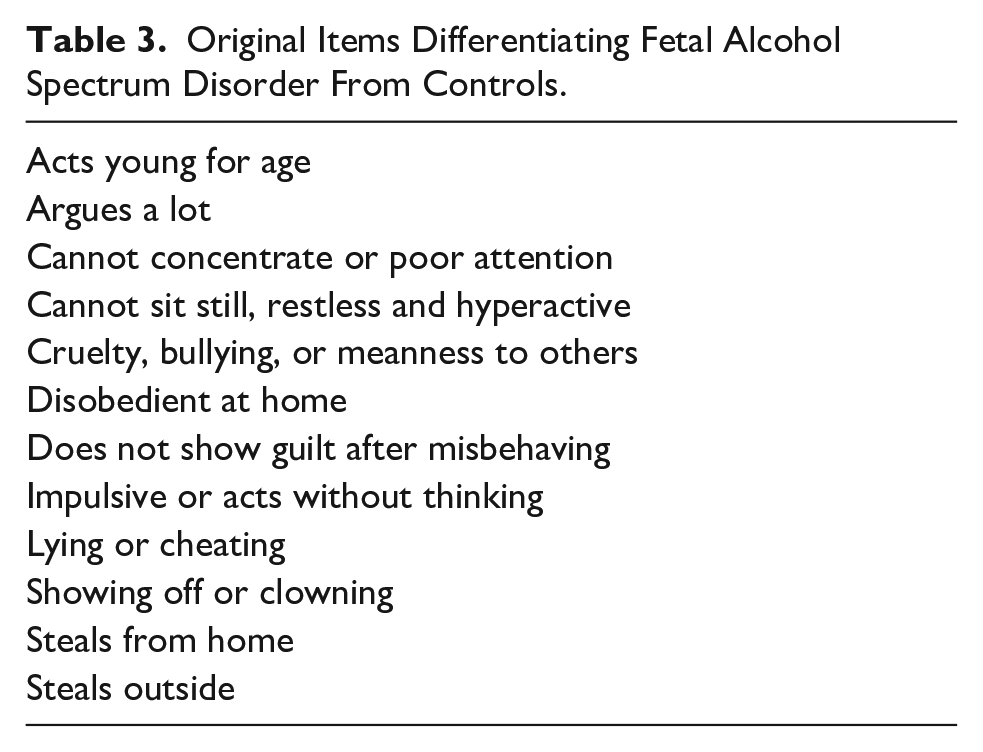
Rovet’s original work compared the achievements on the CBCL in 3 groups of children: 30 children diagnosed with FASD; 30 children with attention deficit hyperactivity disorder (ADHD), but no FASD; and 30 healthy children matched for age and socioeconomic status. 6 Originally, 12 CBCL items significantly differentiated children with confirmed FASD from controls (Table 3).
Original Items Differentiating Fetal Alcohol Spectrum Disorder From Controls.
In analyzing these data, 6 items significantly separated children with FASD from those exhibiting ADHD (Table 4).
Items That Significantly Separated Children With FASD From Those Exhibiting ADHD.

Abbreviations: FASD, fetal alcohol spectrum disorder; ADHD, attention-deficit hyperactivity disorder.
Discriminant function analysis identified predicting differences among groups. The following set of 7 items separated FASD from controls: “no guilt,” “lying or cheating,” “cannot concentrate,” “restless,” “impulsive,” “disobedient,” and “acts young.” Scores of 6 on these items differentiated the groups with a sensitivity of 86% and specificity of 82%. 6
FASD Versus ADHD
Because 70% of children with FASD exhibit symptoms of ADHD, it was critical to try to distinguish between the 2 conditions. Two combinations of items significantly differentiated these groups with high sensitivity and specificity (Table 5).
Differentiating FASD From ADHD: Option 1.

Abbreviations: FASD, fetal alcohol spectrum disorder; ADHD, attention-deficit hyperactivity disorder.
Six of 7 endorsed items are positive for FASD with 86% sensitivity and 82% specificity.
For children not showing ADHD symptoms the following 3 different combinations of items appear to distinguish FASD from non-FASD (Tables 6-8).
With 3/4 Positives Identify FASD.
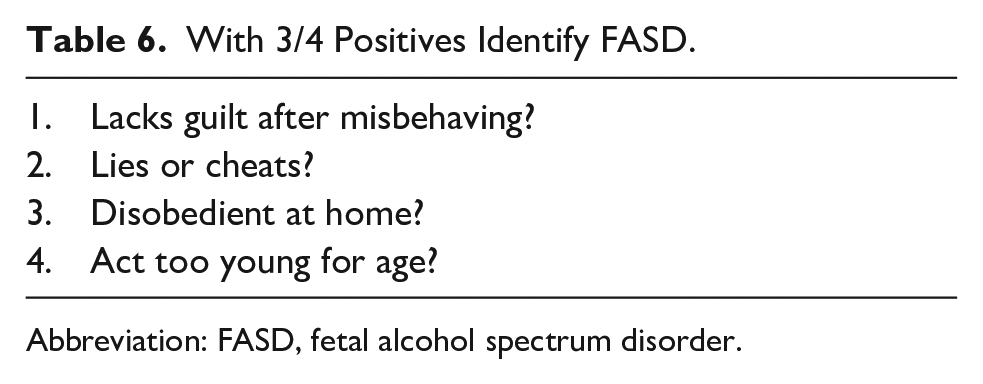
Abbreviation: FASD, fetal alcohol spectrum disorder.
With 2/3 Positives Identify FASD.

Abbreviation: FASD, fetal alcohol spectrum disorder.
With 3/6 Positives Identify FASD.

Abbreviation: FASD, fetal alcohol spectrum disorder.
Testing Children at 4 to 6 Years of Age
A potential challenge is the fact that the CBCL uses an age cutoff of 6 years, whereas in many cases families and clinicians may wish to apply this scoring system for children 4 to 6 years of age.
The authors compared the scores of children 4 to 6 years diagnosed with FASD to those referred but not receiving a diagnosis, as well as healthy children of the same age. 8
Out of the 10 CBCL items used at age 6 to 13 years, 3 are not scored in children between 4 and 6 years (lies and cheats, steals at home, steals outside home). Using the 7 remaining items, children with FASD endorsed significantly more items (6.7 ± 1.3) than healthy controls (2.3 ± 1.2), or alcohol-exposed children who were not given an FASD diagnosis (4.7 ± 1.9).
Using a cutoff of 5 out of 7 items, the NST had a 94% sensitivity and 96% specificity in identifying children aged 4 to 6 years with FASD.
Differentiating Children With FASD From Psychopathology Without Alcohol
The previous steps of development of the behavioral phenotype tool for FASD have shown that the items distinguishing children with FASD from non-FASD (eg, ADHD) are all signs of conduct disorder, which can very well be genetic-familial. There is a strong correlation between parental alcoholism and psychopathy or other forms of conduct disorder, and hence, the test results till now do not rule out psychopathy versus fetal alcohol disorder. The next task in developing the CBCL-based phenotype analysis included trying to separate maternal alcohol use from maternal psychopathology.
For that end the authors recruited 4 nonexclusive groups of children (8–15 years). 9
Children exposed to alcohol in utero (n = 25)
Children not exposed to alcohol in utero (n = 46)
Children exposed to parental psychopathology (n = 37)
Children not exposed to parental psychopathology (n = 34)
To distinguish between the effects of alcohol and parental psychopathology, the children were further subdivided into groups with alcohol exposure in utero and parental psychopathology (n = 23), and psychopathology without alcohol exposure (n = 14).
Children exposed to alcohol scored significantly lower than unexposed children on school competency, special classes, repeating a grade, more disobedience, and vandalism.
Children with parental psychopathology differed from children without parental psychopathology in the anxious/depressed, social problems, and attention problems subscales. The subscale items that were significantly different between the groups were nervousness, self-consciousness, feelings of worthlessness, loneliness, and difficulty in concentration.
No significant differences were found when the groups with alcohol and parental psychopathology, and psychopathology without alcohol were compared.
Parental psychopathology was a significant predictor of a child’s internalizing behaviors, as well as social problems, whereas alcohol exposure was more predictive of externalizing behaviors.
Differentiating Children With FASD From Those With Prenatal Alcohol Exposure but No FASD
A study from Edmonton, Alberta, compared the NST achievement among children 6 to 17 years of age, among 48 FASD children, 22 with prenatal alcohol exposure but no FASD diagnosis and 32 typically developing children. 10 The NST yielded 62.5% sensitivity among participants with FASD and 50% among those exposed to alcohol but not diagnosed with FASD. Specificity was 100% and no normative child scored positive. The fact that alcohol-exposed, but not FASD diagnosed scored often as positive highly suggests that many of them may have FASD. Within the FASD cases, the sensitivity among adolescents (70.8%) tended to be higher than among children aged 6 to 11 years (54.2%), suggesting that with age more items become positive as FASD symptoms may be clearer.
The Effect of Maternal Depression on the NST Score
Maternal depression is not uncommon among families with FASD, and it may affect the maternal reporting of symptoms of the child. Heynes and colleagues compared the NST scores among 134 children previously diagnosed with FASD, 112 typically developing children, and prospectively collected results of children born to and reared by mothers suffering from clinical depression (n = 49) and additional typically developing children. In this study, none of the children born to depressed mothers screened positive on the NST; however, substantial numbers scored positive on the hyperactivity item. The mother’s level of depression as measured by her score on the Center for Epidemiologic Studies Depression Scale correlated with the child’s conduct, specifically on the item of lying/cheating and disobedience at home. This study indicated that the sensitivity and specificity of the NST are not affected by maternal depression. 11
Clinical Application of the NST for FASD Behavioral Phenotype
Over the last 5 years, Rovet et al’s NST tool has been utilized in several FASD diagnostic clinics in Israel as an adjunct tool 12 to the international criteria for diagnosing FASD.1,2 Its role was especially directed to cases where maternal drinking history was not directly apparent or when the pathognomonic facial dysmorphic features have not been evident. It has been included in clinical reports and presented to the court system in cases dealing with youngsters potentially afflicted by fetal alcohol exposure.
The appendix presents the guidelines for the NST, through 2 exemplary cases.
Conclusions
Because of the overwhelming range of brain insult caused by fetal exposure to alcohol, studies continue to describe different aspects of this “generalized deficit in processing complex information,” 4 but such information has not been used to date to identify a neurobehavioral phenotype that can assist in the diagnosis of the most common cause of congenital mental morbidity. 13 The NST system described above may help numerous afflicted children in whom some of the needed criteria for FASD diagnosis may be missing, whereby the behavioral phenotype may help them get the support they urgently need. More work is needed to further validate this tool.
Footnotes
Appendix
Author Contributions
GK conceived this project and wrote the first draft. AO critically reviewed the manuscript and added additional elements.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.