
Abstract
Birth asphyxia is a global health burden, and effective neonatal resuscitation could reduce the burden of deaths. Providing a suitable newborn resuscitation care will depend on the availability of an effective skilled health worker, who is competent in neonatal resuscitation. The study explores and assesses the effect of neonatal resuscitation training and retention of knowledge and skills in the management of asphyxiated newborns in rural Nigeria. This study used a narrative analysis technique to analyze data from a semistructured, individual interview. Data were analyzed using ATLAS.ti 8 qualitative software and applying the principle of thematic analysis. There was a considerable retention of knowledge and ability to practice the procedure even though some equipment was not available. Proficiency in neonatal resuscitation is an essential intervention for the survival of newborns and infants. Therefore, execution of neonatal resuscitation training program in rural communities can further improve knowledge and skills of community birth attendants in Nigeria.
Introduction
Globally, about 4 million deaths occur in neonates while about 99% of them take place in low- and middle-income countries. 1 The transition from intrauterine to extrauterine life is characterized by a series of unique physiological events. At birth, many vital things occur to enable transition to extra uterine life successful. According to the World Health Organization (WHO), birth asphyxia is the failure to initiate and sustain breathing at birth. It causes about a quarter of all the neonatal deaths. 2 About three quarters of all neonatal deaths occur during the first week of life, while a million babies die on the day they are born. 3 Efficient resuscitation at birth can prevent a huge percentage of these deaths. 4
The WHO and the American Academy of Pediatrics endorsed guidelines for neonatal resuscitation (NR) act as an established practice set to improve outcomes in asphyxiated newborns. The guidelines and processes emphasized the significance of drying, stimulating, and warming babies in distress, as well as clearing their airways. If the newborns, after this important procedure has been done, still have persistent apnea or bradycardia, ventilation with bag-and-mask or any equivalent device is indicated, 5 and this creates an important measure in the management of asphyxiated infants. Even though the intervention is relatively simple and inexpensive, its effectiveness of NR is not universal. Translating resuscitation principles into practice is somehow difficult in settings where practitioners lack training in newborn care and where access to essential resuscitation equipment is limited, unlike health care environments that benefit from highly skilled and well-outfitted resuscitation teams. 5 It is pertinent to know that in parts of many low-income countries, resuscitation practice and intervention may not be present or unsuitable. Equipment like bulb syringes and bag-and-mask devices may be substandard or not available; even where present and functioning, health care professionals may not be familiar with their use. 5
Effective resuscitation could prevent some of these asphyxia deaths as well as improve the outcomes of surviving asphyxiated babies. Studies on the effectiveness of neonatal resuscitation program (NRP) training and adoption of different methodologies indicate an increase in knowledge and skill scores after training. Several of the studies have documented the immediate outcomes in terms of knowledge and skills of the participants after training in low-resource settings. 6
The NRP is the official educational program of the American Academy of Pediatrics and the American Heart Association for educating and training health care providers in the knowledge and skills of neonatal resuscitation. 7 NRP was introduced in 1987, and it was reported that deaths caused by birth asphyxia in the United States decreased by 42%, a decade after its introduction; although it was noted that the improvement cannot be ascribed to NRP alone.8,9 Although studies conducted in China, India, and Uganda suggested that training in resuscitation with the NRP or other programs reduced neonatal mortality caused by birth asphyxia, these studies did not show a consistent decrease in mortality.9-12
Also case studies conducted in China and India showed that 90% of newborns with asphyxia need only drying, warming, and stimulation to restore them back to life.10,13 These techniques with good patent airway, suctioning, ventilation, administering oxygen, and chest compressions are parts of the NRP. 14 NRP is the developed world’s standard of care to prevent death and complications of cerebral palsy due to asphyxia, and when systematically implemented by trained personnel, it has the potential to annually prevent 192 000 intrapartum-related neonatal deaths worldwide and 5% to 10% of deaths related to preterm complications.15,16
In Nigeria, the burden of newborn death is enormous. Various studies have reported that perinatal asphyxia is a leading cause of neonatal mortality and morbidity in Nigeria, especially among babies born outside the teaching hospital. 17 According to a World Bank report, Nigeria has one of the highest neonatal mortality rates in the world and NR training is not directed to the appropriate health care provider. 18 As a result of this, mortality challenges related to asphyxia-related death occur in newborns. 19 According to a UNICEF report of 2018, neonatal mortality rate per 1000 live births in 2017 for Nigeria was 33%, and 27% in Sub-Saharan Africa. 20 In Nigeria, community health extension workers, traditional birth attendants (TBAs), and other birth attendants assist in majority of births more often than doctors in rural and community primary health care centers (PHCs). 19 This study therefore explored and assessed the influence of NR training on retention of knowledge and skills of community health extension workers to manage asphyxia in newborns and infants in Nigeria. We are not aware of any previous qualitative study on the influence of NR training on practice of community health extension workers in the PHC setting in Nigeria. This study will enhance the NR knowledge and skill competence among community health extension workers, and this has the capacity of reducing the high neonatal mortality rate in rural communities in Nigeria.
Methodology
This qualitative study was part of a larger study toward testing and refining a NR training model for semiskilled birth attendants. The qualitative method used in data collection was focused group discussions (FGDs) and in-depth interviews (IDIs) with participants. Each interview was moderated by the researcher; this was to ensure that the technicalities of the study were not misplaced or misinterpreted. The data were analyzed using a narrative analysis technique. This technique is similar to Constant Comparison analysis technique. 21 This method gives a systematic and creative process for analyzing data. The narrative technique was decided to be best suited for this study because of the nature and the purpose of the qualitative data. Codes were generated and themes developed. These themes were partly created following the objectives. There were 3 major themes in this study. These themes were developed through an inductive and deductive process. This research was conducted at PHCs in Oyo State of Nigeria.
The study participants were the community health extension workers working in 54 PHCs in selected local government associations. Respondents for FGDs and IDIs were purposively selected from the quantitative sample, that is, those who participate in NR training. The community health workers selected were those with extensive knowledge and experience in providing maternal and neonatal care at the PHC based on their years of experience. Fifteen participants were selected for FGD, with 2 groups of 8 and 7 participants, while 10 participants were selected for IDI.
Data were collected by the researcher (AAO) in Yoruba (local language) as preferred by participants. A semistructured interview guide was adopted and used for each participant. 22 Qualitative research helps researchers access the thoughts and feelings of research participants, which can enable the development of an understanding of the meaning that people ascribe to their experiences. In this study, face-to-face interviews, through FGDs and IDIs, were used to explore research phenomenon and help in clarifying less-well-understood problems and situations. These tools were selected because they aligned with pragmatism paradigm.
During the interviews, participants were so excited, and this was demonstrated throughout the period. The interview lasted 50 to 90 minutes and was audio-tape recorded with participant approval. Because they were semiskilled birth attendants working in the community, they were comfortable with “Yoruba” indigenous language; therefore, all interviews were conducted in “Yoruba” language. All interviews were translated into English language, and transcription was done verbatim at the end of each day.
The interview transcripts were read line by line several times, to achieve data immersion while reflecting on the data analysis. ATLAS.ti, a qualitative software, was used to manage the data.
Trustworthiness in qualitative research is achieved by establishing adherence to a number of criteria during data collection and analysis to ensure truth value, applicability, consistency, and neutrality of the findings. This study achieved trustworthiness by obediently following the established criteria during data collection and analysis, to guarantee significant reality, uniformity, and objectivity of the findings. The trustworthiness of this study was established with reference to Guba’s 4 proposed criteria of Credibility, Transferability, Dependability, and Confirmability. 23
Ethical Approval and Informed Consent
The study was approved by the Biomedical Research Ethics Committee of the University of Kwazulu-Natal, Durban, South Africa (BE391/18), and Oyo State Ministry of Health Research Ethical Committee, Nigeria. All participants provide a written informed consent prior to participation in the study.
Results
The participants were CHEWs (community health extension workers) aged between 25 and 65 years and were all females. They have been practicing for between ≤10 and ≥30 years. All claimed to be married and had postsecondary school education. The demographic characteristics of participants are shown in Table 1.
Participants’ demographical characteristics.
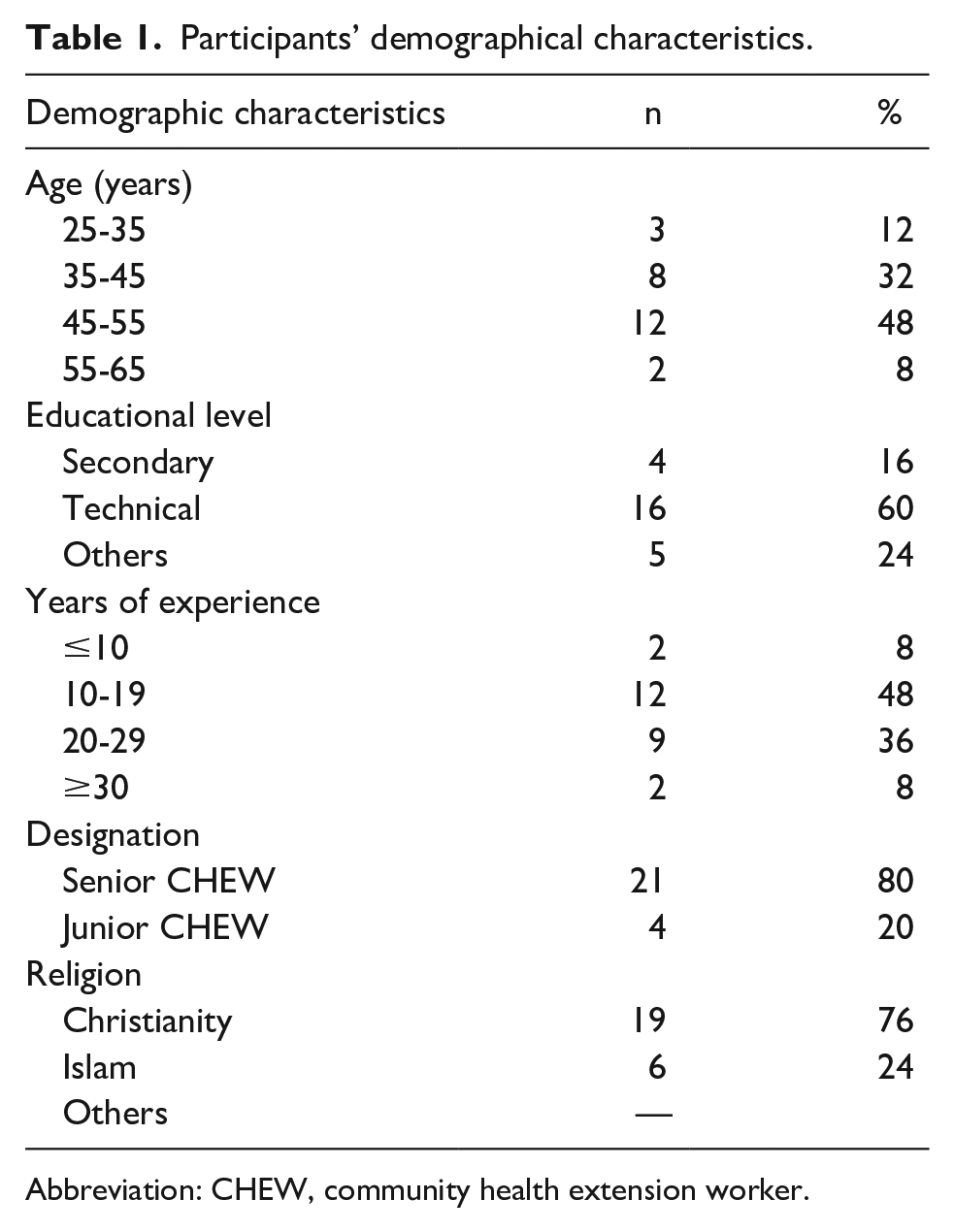
Abbreviation: CHEW, community health extension worker.
These community health care workers shared their knowledge and experiences of NR after intervention was instituted including the influence of practicing NR on the management of asphyxiated babies in their various centers. The interval between their training and qualitative data collection was 4 weeks; the FGDs were conducted before the IDI sessions. FGD and IDI participants were selected randomly from the study PHCs. The themes that emerged were knowledge and understanding of neonatal resuscitation, ability to resuscitate a newborn, and sequential description of steps of neonatal resuscitation. All participants practiced NR at their various PHCs after training was instituted.
Knowledge of Neonatal Resuscitation
In this study, participants shared their knowledge and understanding of NR. This theme is major focus of the training the participants received. Under this theme, participants’ responses were discussed following their knowledge and understanding of the process of neonatal resuscitation, previous practice of resuscitation before this present training, ability to practice neonatal resuscitation, and sequential steps in resuscitation.
Understanding of Neonatal Resuscitation
Participants were asked to define neonatal resuscitation. Most of the participants were clearly able to define neonatal resuscitation. Other participants were noticed to have an idea of what it is but could not properly express themselves. This is evident in their quotes as expressed below. One participant said, Neonatal resuscitation is the care we give to a baby that does not cry or breathe well. (Respondent [R] 1, FGD)
Another participant said, Neonatal resuscitation is when a baby is born or delivered and does not cry or breathe very well. We resuscitate the baby using ambu-bag and mucous extractor to clear the airway. (R3, FGD)
Others expressed themselves as follows: Neonatal resuscitation is using ambu-bag to resuscitate a new born that is not crying or breathing well. (R2, FGD) Neonatal resuscitation from the training you gave us is when a baby is born or delivered whether at term or premature and the baby is not crying or breathing, we will resuscitate the baby. (R4, FGD) When we deliver a baby, after suctioning with mucous extractor, clean and cut the cord and we see that the baby is not active, that is, not breathing or crying well, the care or procedure we carry out to make sure the baby cry or breath well is what we referred to neonatal resuscitation. We use ambu-bag to do this. (R5, FGD) Neonatal resuscitation is when we revive a dying baby. We use ambu-bag to give oxygen but we suction the nose and mouth first before applying the ambu-bag. (R6, FGD) The procedure in which we revive a newborn that is not crying or breathe well. (R7, FGD)—FGD, Group A
Thirty-five-year-old junior CHEW with 12 years working experience said, Neonatal resuscitation is a way in which we ventilate an infant or newborn that does not breathe or breathe properly. (IDI_JUNIOR CHEW (35 years), 12 years)
Participants associated a good understanding of NR to the importance of executing the process of resuscitation, by explaining the steps to take in the implementation of the process.
Also, a 55-year-old senior CHEW explained the steps in carrying out the process of resuscitation: Neonatal resuscitation is the activity we carry out to revive a baby that does not breathe. This activity entails clearing the airway of the baby, covering the baby with a warm cloth and make baby warm and to revive in all the ways we are taught last time we had your training. After cleaning the airway, we check and monitor the heart rate and breathing. After that we wrap the baby. After doing all these, the baby will come back to life. If the baby does not breath, we refer to secondary facility and monitor them. (IDI_SENIOR CHEW (55 years), 31 years)
While a senior CHEW with 17 years of working experience, narrated the following: From what you trained us about the other time, neonatal resuscitation is when a baby cannot breathe or his breathing is not good, we perform resuscitation on the baby to make him live and not die. We can use ambu-bag to introduce oxygen to the baby. We can suck the baby, making his airway patent. (IDI_SENIOR CHEW (45 years), 17 years)
Ability to Perform Neonatal Resuscitation
Most of the participants reported that they could perform NR on asphyxiated infants. Some of the participants described how they had performed the process in recent times at their various clinics.
Others expressed themselves as follows: I can resuscitate an asphyxiated newborn now. (R1) I can resuscitate now. (R2) I can resuscitate as well. (R4) Yes, I can do it. (R5) I can do the resuscitation. (R6) Yes ma, I can. (R7) I can resuscitate. (R3) But ma, even though I can resuscitate, we don’t have the ambu-bag to do it. (R5) Moderator: So what have you been dong or using? I remembered that during the training, I told you that if there is no ambu-bag, what we can do? We have been doing mouth-to-mouth resuscitation but I just want you to know that the government has not given us this bag to use. Although not the ambu-bag alone but other equipment and instruments. (R5) Moderator: That is very good of you.—FGD, Group B Moderator: Based on the training you had on NR, can you resuscitate an asphyxiated newborn?
Similarly, same senior CHEW reportedly said, Yes, I can do the resuscitation on infants who is asphyxiated, but our centers don’t have ambu-bag. We make use of mucous extractor and do mouth-to-mouth for those of us that can do it. And it has been working for us. (IDI_SENIOR CHEW (45 years), 7 years)
Another junior CHEW explained, Yes, I can. I will ventilate with ambu-bag, I will place the ambu-bag on face of the baby with the mask part placed over the mouth and nose of the baby while I squeeze the bag part to give oxygen to the baby. When I see the chest moving, then I know that I have done it well. (IDI_JUNIOR CHEW (35 years), 12 years)
Some participants, however, mentioned that having equipment to work might be more helpful in remembering the steps they are to follow in neonatal resuscitation.
A 33-year-old senior CHEW reiterated, Personally, I can do it, others too can do provided we have booklets or poster that can show us the step-by-step way of doing the procedure. I know it is not really difficult but it is easy to forget the step-by-step way of doing it. We can do it anyway. (IDI_SENIOR CHEW (33 years), 12 years)
Knowledge and Practice of Sequential Steps in Neonatal Resuscitation
Following the training received by the participants, they were asked to list out the steps involved in resuscitation of asphyxiated infants. Most of the participants were able to mention the steps. However, very few of the participants were able to correctly list the steps in the right order without prompts from the interviewer. The correct order of NR as the participants were taught is provision of warmth, suction, stimulation, and ventilation.
Participants’ responses are as follows: After delivery, we then cut the cord, clamp, and suction the baby of all mucous. We then clean the body, put dress on and wrap in towel. (R3) The first thing is to make the baby warm not to expose the baby. Then check the pulse and respiration of the baby to be sure it is adequate. Check the color of the baby to see that it is pink. We suck the mouth and nose of the baby. Then we clean the body and use another towel to wrap him up. If the baby is crying very well, he does not have problem; just wrap and put beside the mother. But if the baby is not crying, we use an ambu-bag to ventilate the baby. We do this for just 1 minute and continue to assess and check the baby. (R4) In my own understanding, after the birth of the baby, that is, after delivery, we clean the baby with olive oil or clean the liquor with a towel, we then put the baby on the mother’s abdomen, wrap the baby with a clean towel. If the baby does not cry, we put him on a flat surface where we can resuscitate him, clear the airway of all mucous, use ambu-bag to resuscitate him, cut the cord and use cord clamp to clamp. After sometime, we assess the baby again before continuing ambu-bagging. If the baby’s response is minimal, we can suction again. We suction the mouth before the nose and reapply the ambu-bag to give oxygen again. (R5) Steps in neonatal resuscitation: immediately after delivery, suctioning the baby’s mouth and nose with mucous extractor is very important. The baby will cry immediately. But if the baby does not cry, that is when we resuscitate the baby. Put the baby on mother’s abdomen, cut the umbilical cord and clamp with cord clamp. Continue to suction the baby; cover the baby with a towel, so that he won’t get cold, put the baby on a flat surface and use ambu-bag to give oxygen. When you see that the baby is breathing, we stop ambu-bagging and suction him if need be, if not we will monitor the baby continuously until he breathes very well or cry. Sorry, I forgot to say that the towel used to clean the baby will be removed and another towel will be used to wrap. (R6) Neonatal resuscitation starts from when the baby is born or from the training. We were taught that even mothers can rush a baby or child to our center, not breathing or not breathing well or it might be within our community, they can come and call us to attend to a child that is not breathing or breathing well. Whichever the case may be, we will open the mouth and suction or remove anything that may obstruct the airway whether mucous or any obstruction. Then we use an ambu-bag to give oxygen. The ambu-bag should cover the mouth and the nose and squeeze the ambu-bag to release oxygen. After sometime, we assess the baby to see that he is breathing well. If it is at the community, we can do mouth-to-mouth resuscitation. After that, we wrap the baby very well. (R7)—FGD, Group A Steps in neonatal resuscitation start from suctioning. After this, we cut the cord and place baby on the mother’s abdomen, clean the baby, and wrap him in a big towel. If the baby does not cry, we will use ambu-bag to introduce oxygen into the baby, this we do on a flat surface. (R2) The way you taught us: first step is to make the baby warm. Although when we deliver we suction first but in resuscitation, you keep the baby warm, then suction if need be. After sucking the baby, we will cut the cord and clamp, if the baby is good, then we don’t need much stress, we just clean the baby and wrap with a good cloth, but we dress for the baby before wrapping. If the baby is not good or active, we can suck again. Then use ambu-bag to resuscitate him for some time. We should assess the baby at interval. (R3) Steps in neonatal resuscitation include suctioning the baby immediately after birth, cutting the cord, cleaning the baby’s body, and wrapping him in a warm cloth. If the baby is not crying or breathing well, we suction again and ambu-bag. (R4) In neonatal resuscitation, we were taught that if a baby does not cry or breathe well, he/she needs resuscitation. This starts from the labor room when the baby is born. Immediately after delivery, if we see that the baby is not crying, we suction the baby very well, then use ambu-bag to give oxygen to the baby. After that we assess the baby, clean the baby, and wrap in a cloth or wrapper. (R5), FGD, Group B
Discussion
Knowledge of Neonatal Resuscitation
In reducing neonatal mortality related to birth asphyxia, birth attendants must be well equipped with the knowledge and skills of neonatal resuscitation. This study showed that the reported knowledge and skills of semiskilled birth attendants were sufficient. Adequate knowledge and skills of health professionals are essential for improving neonatal outcomes. The study revealed that participants had improved knowledge of NR after training was instituted. This finding was in agreement with the result from India. 6 It was observed that participants had improved knowledge after administration of an educational intervention as compared with their knowledge during the pretest and was noted that there was a significant increase in knowledge in all areas tested. It is also in line with the study conducted in Zambia, 7 where there was an increased knowledge after NR training. Consistent with this study was the findings from Ghana, Malawi, and Afghanistan, respectively, it was shown that there were improved knowledge and skills among participants of the studies.24-26 Contrary to this study finding was a study by Murila et al, 27 in their assessment of knowledge on NR among health care providers in Kenya and by Gebreegziabher et al, 28 in their study conducted in Ethiopia. It was reported that health workers had a poor performance when their knowledge of NR was assessed. A study conducted in Tamale, Ghana, 29 also reported that almost all participants in the study had insufficient knowledge of neonatal resuscitation. These studies and many others have shown that NR training implementation influence knowledge enhancement of health workers although the level of knowledge attained during posttraining decrease after the implementation period. Ogunlesi et al 30 in their study conducted in Nigeria among skilled birth attendants revealed that there was a high level of knowledge of NR among participants who had had training and has been practicing it before, compared with those who did not have training in NR before. It also revealed improved knowledge and skill in NR practice after the training.
Understanding of Neonatal Resuscitation
This study also showed that semiskilled birth attendants had a good understanding of the steps in NR, although some could not mention those steps accordingly. They were skilled in critical areas of NR steps like suctioning the airway for patency to maintain spontaneous breathing and providing warmth. This may be as a result of their knowledge and skills in newborn care and on the fact that they have spent substantive years practicing in their respective PHCs. This study also revealed that the birth attendants understood what NR is all about and was able to recall the critical aspect of NR 4 months after their initial training. This was in agreement with the study of Subbiah et al, 6 in which there was improved retention of knowledge among respondents 1 year after initial training was conducted. It is also similar to a study on practice and outcomes of NR on newborns with asphyxia conducted by Carlo et al. 7 The study revealed that effective NR training with a focus on maintaining the warm chain and other steps are needed for health care providers providing NR. But in contrast to this study was a finding from a study conducted in Zambia, where there was a decline in knowledge after 6 months of training. 7 In a study conducted in Ethiopian by Hoban et al, 31 it was revealed that resuscitation knowledge improved after the training and participants received the training well. In the study of Draiko et al 32 in South Sudan, it was found that the practical psychomotor skills and competency of the health workers improved greatly and were retained after 3 months. This is in contrast to studies about retention conducted in Rwanda and Kenya, where it was pointed out that it was most challenging to retain the skill and competence at 3 to 6 months after the Helping Babies Training intervention.27,33 In the study of Opiyo et al, 34 it was reported that there was a significantly high proportion of perfect initial resuscitation steps among participants and this is in agreement with the present study. This study is in agreement with the study from Afghanistan 26 ; it was found out that nearly all of the facilities used possessed necessary supplies of basic equipment for neonatal care and infrastructure components, thereby participants understood NR and were skilled in practicing it. Although very few facilities lack a bag, mask, or simple suction device, which affected their understanding, knowledge, and skills needed to perform resuscitation. This is similar to this present study, which revealed participants’ reported lack of bag and mask in nearly all the PHC settings in Oyo State. Also, the present study showed that other basic instruments for the practice of resuscitation were bought by individual patients before coming for delivery at any PHC.
Knowledge of Sequential Steps in Neonatal Resuscitation
The study conducted in Ghana explored knowledge on specific areas of neonatal care and resuscitation. It was revealed that knowledge on evaluation and identification of babies in distress and appropriate interventions to employ in remedying the situation were insufficient.
In the study conducted in Ghana, it was reported that participants demonstrated insufficient knowledge on evaluation and assessment of babies at birth and the appropriate interventions to carry out for babies who need resuscitation. 29 In the study of Ogunlesi et al 30 in Western Nigeria, it was reported that almost all participants in the study had adequate knowledge in the evaluation of babies at birth and knowledge of appropriate intervention to carry out after evaluation. In the study conducted in Kenya, it was observed that there was an adequate initial resuscitation step among trained observed participants compared with the untrained controlled group. They had knowledge of the sequential steps in NR and it is in line with the study of Opiyo et al. 34 The outcome of Opiyo et al’s study revealed a significantly improved performance of NR steps as evidenced by adequate initial practice. In contrast to this study, is the study conducted in Afghanistan, which observed providers’ inability to recognize the need for resuscitation in nearly all the facilities, even though the facilities were equipped with basic equipment to practice newborn care. 26 Also, it was reported that 3 months after NR training was done, participants from many facilities did not perform NR procedure, while few participants claimed lack of training as the reason for nonperformance and others claimed no newborn required resuscitation even though there were records indicating early neonatal deaths in many facilities. This is contrary to the present study where many participants have been practicing the skills of NR immediately after the training and recalling the steps 4 months after the initial training. Similar to this study is a study conducted in Zambia among TBAs. 7 It was reported that the training intervention was highly effective at reducing neonatal mortality in a rural setting. The study provided relevant details of how NR intervention training programs were developed and TBAs were trained to perform them.
Conclusion
The effect of training community birth attendants resulted in better retention of the knowledge and skills required in performing resuscitation on asphyxiated infants. It was shown that attendance at the NR training course improved their knowledge and skills. But lack of essential NR equipment was observed, and staff shortage remained a major problem in all the PHCs used for this study. This may be one of the many reasons for not having good NR skills and the outcome of training failing to develop in most low-income countries.
Recommendation
Introducing regular schedule and serial NR training programs can further enhance and improve the knowledge and skills of CHEWs, who attend to delivery in low-resource settings like Nigeria. This is crucial to improving the survival of newborn infants and reducing the high mortality rate resulting from asphyxia-related causes in rural communities in Nigeria. There is still a need to stock some emergency equipment essential to NR in all the PHCs. The importance of having newborn resuscitation equipment cannot be overemphasized as stated by the WHO. 2 The United Nations Commission on Life-Saving for women and children includes a bag and mask device for newborn resuscitation on its list of 13 essential, affordable, effective, but underutilized life-saving commodities. Therefore, it is pertinent for the government to provide adequate funding, equip health facilities with essential and basic items needed to provide standard quality care.
Footnotes
Acknowledgements
The authors are grateful to all birth attendants who participated in the study.
Author Contributions
AAO conceptualised the study, responsible for literature search, supervised and participated in data collection, data analysis and prepared the manuscript under the guidance and supervision of BPN. AAO and BPN contributed to the development and study design of the study. BPN reviewed the literature and manuscript. All authors contributed to critical revisions of the manuscript and approved the final submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the University of Kwazulu-Natal, College of Health Sciences Scholarship to AAO.