
Abstract
Introduction. Pediatric thoracic empyema is a special entity with increasing frequency. Consensus regarding the best management strategy is still evolving. We describe our single-center 10-year experience adopting intrapleural thrombolytics using tissue plasminogen activator as first-line treatment following failure of simple thoracostomy drainage techniques. Methods. Observational prospective study included all children from 1 day to 18 years admitted for parapneumonic effusion and treated with intrapleural thrombolytics. Results. From January 2008 to December 2018, 95 patients were treated by intrapleural thrombolytics for different stages of empyema thoracis. Number of thrombolytic doses required is 2.1 (range = 1-3), and mean amount of drainage is 1050 mL (range = 400-2500 mL). Mean total days of hospitalization is 7.3 days. Complete re-expansion was the primary outcome in 94 patients (98.9%). Conclusion. Intrapleural thrombolytics in complicated pediatric thoracic empyema results in excellent outcome and should be encouraged particularly in limited resource countries.
Introduction
Empyema thoracis occurs in children when parapneumonic effusion complicates pulmonary parenchymal infection resulting in accumulation of exudative fluid in the pleural space followed by fibrin deposition, which if not properly treated would eventually form an inelastic peel that inhibits lung from proper expansion. 1
A meta-analysis performed by Avansino et al showed that approximately 1 out of 150 children admitted for pneumonia only would develop empyema, at an incidence between 0.4 and 6 cases per 1000 pediatric admissions. 2 Giving an approximate incidence of 0.6% to 2% of pediatric pneumonia cases to be complicated by empyema. 3
Though its well-known that the infection process occurs in a continuum and not distinctly, pediatric thoracic empyema (PTE) has been classified into 3 different stages: (1) exudative or simple parapneumonic effusion, where there is only clear pleural fluid; (2) fibriopurulent stage, where the fibrin starts to deposit forming septations and loculations within which the fluid is still flowing freely; and (3) organizing phase, where the fluid would be infiltrated by fibroblast and the thin intrapleural membranes changes to thick nonelastic peel resulting in impairment of lung function.1-4
Currently, management of pediatric empyema is dependent on local practice guidelines and physician preference as there is no standardized treatment regimen for PTE yet. This might be due to a deficiency of pediatric-based and population-based evidence.4,5
Sixty-nine years ago, use of fibrinoltyics was described in the management of complex pleural process by Tillet and Sherry when they introduced streptokinase. Ever since, the use of streptokinase as a thrombolytic agent was taxing because of the possibility of antibodies’ development and the occurrence of delayed hypersensitivity reaction. This led to the introduction of urokinase to minimize the aforementioned complications associated with streptokinase. Withdrawal of urokinase from markets by the Food and Drug Administration in the United States because of infection risks led to the emergence of alteplase in 2000. The use of intrapleural thrombolytics in certain patients has been stated by many authors despite the controversies about many aspects.4-6
In spite of the breakthrough in antibiotics therapy in the latest era, parapneumonic effusion and pleural empyema are still a frequent clinical problem that may cause significant mortality and morbidity. The well-established treatment for parapneumonic effusions is drainage by closed system tube drainage and systemic antibiotics.3,7 However, the latter can be associated with failure rate as high as 40% in addition to increased hospital stay duration.2,8 Surgical intervention becomes mandatory when the infection and sepsis are not adequately controlled by tube thoracostomy. In multiloculated pleural effusion and empyema, installation of a thrombolytic agent like tissue plasminogen activator has been broadly described for ease of lysis of the fibrinous loculi.5,7,8 Despite many studies describing outcomes of intrapleural thrombolytics in pediatric empyema thoracis, the current literature is still deficient in randomized control trials about this subject, which has led to controversial evidence in support for the use of this approach.5-8 In this article, we discuss our 10 years of experience in the outcome of using intrapleural thrombolytics for pediatric patients with thoracic empyema.
Patients and Methods
Patient Selection
Observational prospective clinical cohort study included all children aged from 1 day to 18 years, admitted consecutively for treatment of parapneumonic effusions by tube thoracostomy of appropriate size and length (14-28 French) combined with intrapleural instillation of thrombolytics in a single center. Other causes for pleural effusion such as tuberculosis and malignant effusions were excluded.
From January 2008 to January 2018, 95 patients were treated by intrapleural thrombolytics for different stages of empyema thoracis. Tissue plasminogen activator (Actilyse, Boehringer Ingelheim) 0.1 mg/kg/dose mixed in 10 to 30 mL of normal saline was instilled through the tube thoracostomy followed by clamping of the chest tube for 4 hours. Patient’s mobilization is encouraged during and after the clamping period to allow better distribution of the chemical agent and for enhancing drainage after de-clamping.
There were 50 females (52.6%) and 45 males (47.4%). Mean age was 6.3 years (range = 0.5-15). Regarding empyema stages, 86 patients (90.5%) were in stage 2, 5 patients (5.3%) were in stage 3, and 4 patients (4.2 %) were in stage 1.
Mean number of thrombolytic doses required was 2.1 (range = 1-3), with a mean amount of drainage 1050 mL (range = 400-2500).
The patients were followed-up clinically and radiological by serial chest X-rays (CXR; Figure 1) for 1, 2, 3, 6, 12, 18, and 24 months and continued to 3 and 5 years.

Chest X-ray shows right side parapneumonic effusion with a chest tube inserted and minimal amount of drainage after 2 days.
The focus was pointed on in hospital course, 1-month follow-up (primary outcome), and 1 year (secondary outcome).
Statistical Methods
Descriptive and inferential statistical analysis has been carried out in the present study. The statistical software SPSS (22.0) and R (ver. 3.2.2) were used for the analysis of the data, and Microsoft Word and Excel were used to generate graphs, tables, and so on. Suggestive significance was when P value was <.05 < P <.10; moderately significant when P value was <.01 < P ≤ .05; and strongly significant when P value was P ≤ .01.
Ethical Approval and Informed Consent
Informed consent and consent for publication was obtained from all parents of the participating children. Ethical approval was obtained from the Ethical Committee of Kurdistan Board for Medical Specialization (Approval Number: 346, August 7, 2018).
Results
A total of 95 (50 females and 45 males) pediatric patients were treated by intrapleural Actilyse, over 10 years. The right hemithorax was involved in 60 patients (63.2%), while the left side was involved in 35 patients (36.8%).
Mean age was 6.3 years (range = 0.5-15), mean hemoglobin concentration was 11.5 g/dL (range = 8-15), mean white blood cells count was 16835.8 cells/L (range = 1500-30 000), and mean erythrocyte sedimentation rate was 81 mm/h (range = 40-110).
There were 86 patients (90.5%) in stage 2, 5 patients (5.3%) in stage 3, and 4 patients (4.2%) in stage 1. Mean number of thrombolytic doses required is 2.1 (range = 1-3), and mean amount of drainage is 1050 mL (range = 400-2500 mL). Mean total days of hospitalization is 7.3 days (range = 1-21 days. Table 1 shows number of doses and amount of drainage distribution of patients studied, and Table 2 shows number of thrombolytic doses required in relation to the provisional stage of empyema. Table 3 shows comparison of study variables according to provisional stage of patients studied.
Number of Doses and Amount Drainage Distribution of Patients Studied.

Number of Doses.

Comparison of Study Variables According to Provisional Stage of Patients Studied.

Abbreviations: WBC, white blood cell; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate.
In 93 patients (97.9%) the presenting symptom was shortness of breath, 91 patients(95.8%) had fever, 55 patient (57.9%) had history of weight loss, 50 patients (52.6%) had dry cough, 45 patients (47.4%) had productive cough, 31 patients (32.6%) had vomiting, 26 patients (27.4%) were not feeding properly, 23 patients (24.2%) had hemoptysis, diarrhea was present in 21 patients, chest pain was present in 21 patients (22.1%), 10 patients (10.5%) had failure to thrive, 2 patient (2.1 %) were accidentally diagnosed, and 1 patient (1.1 %) had stridor.
On physical examination, all patients had unilateral decreased air entry and wheezes (100%), whereas bilateral decreased air entry were found in only 44 patients (46.3%), bronchial breathing were found in 90 patients (94.7%), cervical lymphadenopathy was found in 35 patients (36.8%), and organomegaly was found in only 2 patients (2.1%).
On CXR, 92 patients (96.9%) had pleural effusion (Figure 1), 3 patients (3.2%) had non-homogenous opacity, and 2 patients (2.1%) had multiple air fluid level. Computed tomography was requested in only 5 cases (5.4%); of those, 3 patients (3.2%) had thick effusion, 1 patient (1.1 %) had bilateral cavity lesion, and 1 patient (1.1%) had loculated pleural effusion. In 79 patients (83.2%), Streptococcus pneumonia was the causative microorganism found in the fluid culture and sensitivity, in 7 patients (7.4%) Staphylococcus aureus was responsible, 5 patients (5.3%) had Haemophillus influenza, and 4 patients (4.2%) had Pseudomonas aerogenosa.
Ninety-four patients (98.9%) had total re-expansion as a primary (in hospital) outcome, no signs of lung expansion was seen in only 1 patient (1.1%), who was a 7-year-old male child, with right side involvement, despite 3 doses of thrombolytic and 1100 mL drainage, who recovered well after decortication with good lung re-expansion and no signs of fibrothorax on follow-up. Of the patients who showed total re-expansion in the hospital, after only 1 dose of thrombolytics, at the second month of follow-up signs of moderate fibrothorax started to develop on CXR, ended by decortication at the third month of follow-up.
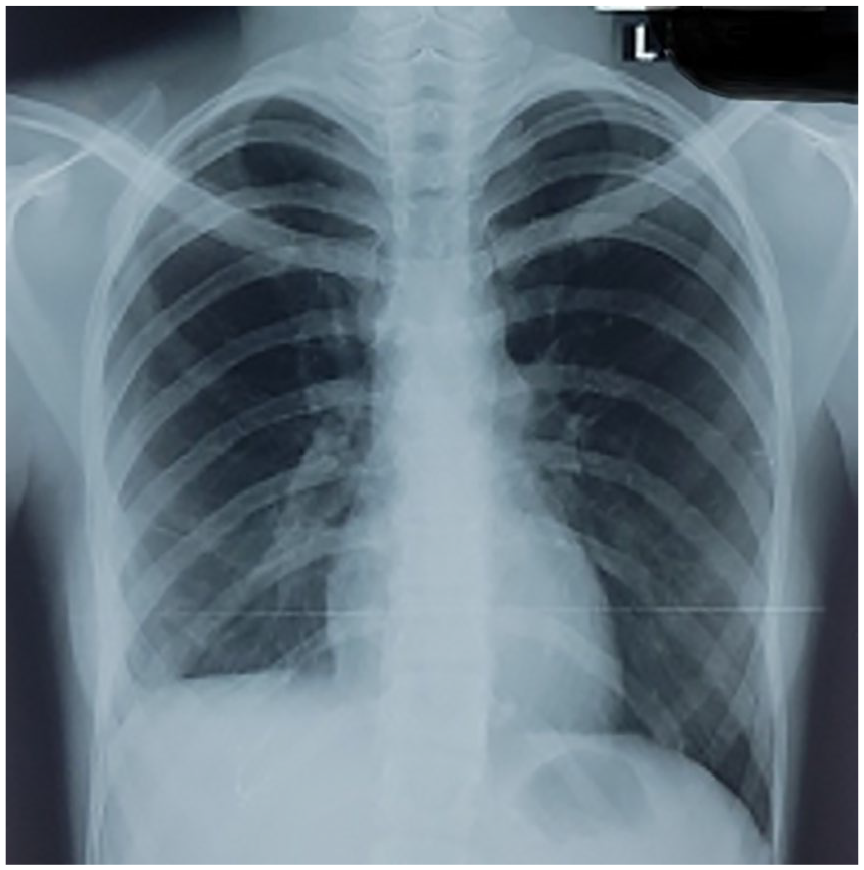
At 1-month follow-up (primary outcome; Figure 2), 63 patients (66.3%) had obliterated costophrenic angle, 16 patients (16.8%) had basal haziness, 11 patients (11.6%) had normal looking CXR, 4 patients (4.2%) had residual effusion, and 1 patient (1.1%) had mild fibrothorax.

The same patient chest X-ray after 1 month from thrombolytic therapy shows minimal right costophrenic angle obliteration with mild right lung entrapment.
At 1-year follow-up, 85 patients (89.4 %) had normal looking CXR (Figure 3), 6 patients (6.3%) had obliterated costophrenic angle, 2 patients (2.1%) had mid fibrothorax, and 2 patients (2.1%) had asthma-like symptoms.
Chest X-ray at 1 year from thrombolytics shows near-normal lung expansion.
Comparison between primary and secondary outcome revealed a P < .001 in favor of 79.0% improvement (Table 4).
Comparison of Primary Outcome at 1 Month Versus Secondary Outcome at 12 Months a .
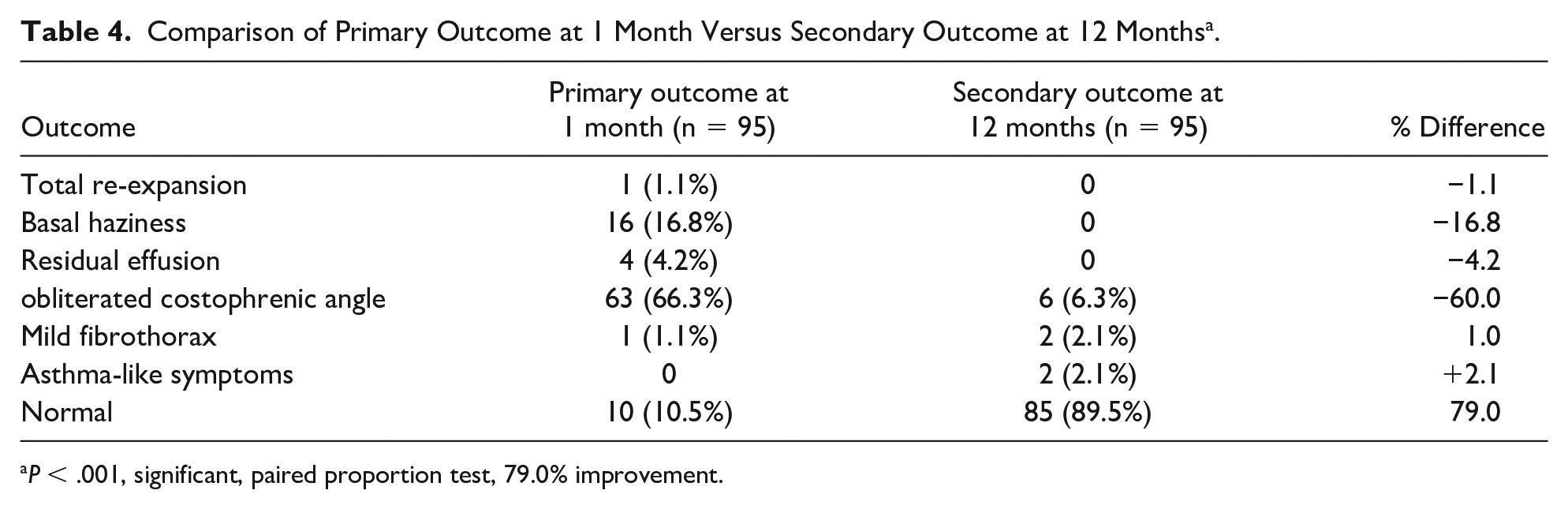
P < .001, significant, paired proportion test, 79.0% improvement.
Discussion
Empyema thoracis in pediatric population is a remarkable factor for morbidity but not mortality, and can represent a therapeutic dilemma; however, so far there is a limited consensus regarding its management, partly due to deficient data from pediatric trials and second due to the inconvenience of applying adult data to pediatric population. The fundamental difference between the 2 groups is the rarity for underlying lung disease in children in contrast to adult favoring the almost always excellent prognosis in the pediatric group treated for empyema as described by the British Society for Thoracic Surgeons guidelines in 2005. 4 However, the reason behind why some healthy children develop empyema and others not is still not clear; perhaps future studies will show genetic predisposition behind that. 8
The 2 ancient pillars for management of empyema thoracis are antibiotics and tube thoracostomy drainage of the purulent fluid. 9 Following this approach alone could lead to prolonged hospital stay and high rate of unsuccessful treatment in advanced stage of this clinical entity. Therefore, the need for a more effective yet less invasive management modality than thoracotomy had led to the introduction of intrapleural thrombolytics and video-assisted thoracoscopic (VATS) debridement or decortication. The aim of all modalities remain the same in breaking the septations, liquefaction of the fibrinous material aiming at restoring the near-normal lung functions. 10 Comparable outcomes of VATS and intrapleural thrombolytics have been stated by various pediatric trials.3,11
Hanson et al 10 studied the effectiveness of alteplase as an intrapleural fibrinolytic agent in pediatric population, and their results showed significant increase in pleural fluid output on irrigation with alteplase, as they stated this was due to volumetric decrease of the intrapleural fluid and not due to inflammatory reaction as previously was postulated. 10
Despite the relatively few consensus regarding management of pediatric empyema thoracis, the most recent published ones, such as the position statement from the Thoracic Society of Australia and New Zealand and the British Thoracic Society guidelines for the management of pleural infections in children, are strongly recommending the use of intrapleural thrombolytic agents with a clear benefit of shortening hospital stay. In addition to the strong advices against standard open thoracotomy as a first-line management, this latter option is only reserved for case of failure of thrombolytic trial and limited expertise in VATS surgery.8,4,12,13,14
In developing countries, choosing the best treatment modality relies on the existing expertise and common local practices. Currently, we are lacking randomized control trials from developing nations to assess the efficacy of intrapleural thrombolytics versus VATS. Nonetheless, in economically and resource-challenged countries, in which epymema thoracis is not infrequent, utilization VATS require and add to the load of the operative waiting lists, cost, and intensive care units.11,14 The fact that in majority of such countries including ours, even the availability of a dedicated pediatric intensive care is a concern and this in turn precludes and discourages adopting VATS decortication for PTE.
Unlike most of published studies where urokinase has been more clinically studied, we presented our experience with alteplase (Actylase) being the thrombolytic agent available.
The commonest microorganism continues to be Streptococcus pneumonia; however, there might be differences in developed countries where pneumococcal vaccines is being routinely used. In our series, we had 4 patients with Pseudomonas aeruginosa as the culprit microorganism, which is a rare cause of community-acquired pneumonia in healthy children,10,14 and one of those children had a total hospital stay of 14 days but otherwise good outcome.
Of a total 95 patients, only 2 patients required decortication, one of them during the initial hospital course with failure of lung re-expansion after thrombolytic and the other at 3 months of follow-up, which stands firm with others’ opinion to encourage the usage of intrapleural thrombolytics in management of PTE.
Conclusions
Pediatric thoracic empyema is a special entity with growing frequency, and adult guidelines should not be applied to this entity.
Management with tissue plasminogen activator (Actylase) has a good success rate and should be always considered prior to thoracoscopic or open surgical intervention.
Limitation
The study is limited to a relatively small sample size and single-center experience.
Future Research
More studies need to be done in this field to help establish a global guideline in the management of thoracic empyema in children.
Footnotes
Acknowledgements
We would like to acknowledge all our personnel who assisted in serving our patients. Also, we would like to appreciate the great efforts of Dr K. P. Suresh, Scientist (Biostatistics), National Institute of Veterinary Epidemiology and Disease Informatics (NIVEDI), Bangalore 560024, India, in analysis of our raw data.
Author Contributions
Aram Baram: Surgeon in charge, study design, follow-up, data collection, manuscript revision, and statistical analysis.
Fitoon Falah Yaldo: Assisted in surgeries, follow-up, study design, data collection, and drafting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was approved by the Ethics and Scientific Committees of Kurdistan Board for Medical Specialization (Approval Number: 364, August 7, 2018).
Informed Consent
Written consent obtained from all participants that their operation photos and images may be used for scientific publications only.