
Abstract
Since its first outbreak in 2007 in the Pacific (Yap islands and Federal States of Micronesia), Zika virus has gradually and recently spread to the Americas in 2015. The neurotropic character of the virus was first noted during this outbreak in Brazil in 2015. Increasing number of infants born with microcephaly and other congenital deformities were identified through studies that have highlighted the importance of prevention of transmission of Zika virus in pregnant women. Long-term outcomes in infants born with this infection are now better understood than at the time of onset of this outbreak. Topics covered in this review include the history, modes of transmission, diagnosis of suspected cases, pathophysiology, complications, and prevention of Zika virus infection.
Keywords
Introduction and History
Zika virus (ZIKV) is a RNA virus in the Flaviviridae family, closely related to other flaviviruses such as West Nile virus, dengue virus (DENV), Japanese encephalitis virus (JE Virus), Chikungunya virus (CHIKV), and yellow fever virus. It was first isolated from a rhesus monkey that was being used as a sentinel for yellow fever virus in the ZIKA forest of Uganda in 1947. The life cycle of ZIKV in Africa used to be primarily sylvatic and was limited to nonhuman primates and mosquitos of Aedes sp, mainly Aedes africanus. Later, it was also found isolated from Aedes aegypti mosquito in Malaysia in 1966.1,2 The first case of symptomatic human infection was reported in 1954 during an outbreak in Nigeria. 3 ZIKV was known to cause sporadic human infections with less than 20 cases of self-limiting illness reported before 2007.2,4
The first outbreak of ZIKV infection was recognized on Yap islands and Federal States of Micronesia in 2007. A large proportion of residents of Yap islands (up to 73% of population above age 3) were found to be infected with ZIKV, and about one fifth of these had reported clinical symptoms. Most of the reported cases during this outbreak had mild illness characterized by fever, rash, arthralgia, and conjunctivitis.5,6 In 2007, ZIKV was also isolated from Aedes albopictus in Gabon, Africa, which was also found to carry CHIKV and DENV. 7 ZIKV then caused an outbreak of human infections in South Pacific (French Polynesia) in 2013-2014, which was its first known outbreak outside of Africa. This is the first time when clusters of Guillain-Barre syndrome (GBS) were identified in the areas of prevalence of ZIKV infection. 2
In 2015, Zika was first detected in Latin America in Bahia, a northeastern state of Brazil, where it was causing an outbreak of “maculoexanthematic” illness marked with rash, myalgia, arthralgia, headache, or fever. Seven out of 24 symptomatic patients who were tested (29.2%) were found to be reverse transcriptase-polymerase chain reaction (RT-PCR) positive for ZIKV. The phylogenetic analysis revealed that ZIKV in Bahia was 99% identical to the isolate from French Polynesia, indicating its Asian lineage. 8 By the end of 2015, up to 1.3 million people were suspected to be infected with ZIKV in Brazil alone. 9 By November 2015, the Ministry of Health in Brazil reported increased incidence of microcephaly in newborn infants and the possible association of microcephaly with ZIKV infection during pregnancy. More than 3000 cases of microcephaly were reported in the second half of 2015 in Brazil, although it is now thought that this number was inflated due to overreporting of this condition. In December 2015, ZIKV was identified in amniotic fluid of pregnant females who were carrying fetuses with microcephaly, and isolation of ZIKV was confirmed from brain tissue of an infected infant who died in the neonatal period. 10 This association of Zika infection in pregnancy with microcephaly was later confirmed by a retrospective study of all the cases of microcephaly in French Polynesia. 11 On February 1, 2016, the World Health Organization declared this association as a Public Health Emergency of International concern. 12 By this time, 28 countries of the Americas had reported cases with ZIKV infection. 13
ZIKV infection in the United States
In 2015, 62 cases of ZIKV infection were reported in the United States, all of whom were returning travelers from affected areas, mostly identified in California (21 cases) and Texas (10 cases). An additional 10 symptomatic cases were reported in US territories in 2015, 9 of which were presumed to be acquired by local mosquito-borne transmission. Because of the risk of Zika infection in pregnant females and possible adverse outcomes, the Centers for Disease Control and Prevention (CDC) issued a travel alert in January 2016, advising pregnant women to consider postponing travel to areas with ongoing local transmission of ZIKV infection. 14 This number increased astronomically to 5168 symptomatic cases in US states in 2016, most of whom were returning residents (4897 cases). A considerable number of the 224 cases were acquired through presumed local mosquito-borne transmission, the majority of which were from Florida (218 cases). Only 45 of these cases of sexual transmission were identified. The US territories, on the other hand, were 7-fold more affected in 2016 with 36 512 cases, out of which 36 367 were due to local mosquito-borne transmission. Sexual transmission of Zika was not reported in US territories as, with such a high rates of local transmission of Zika, it was not possible to determine whether the infection occurred by mosquito-borne or sexual transmission. Overall numbers have gradually decreased in subsequent years of 2017 and 2018 with only 452 and 74 cases, respectively, in US states. Corresponding numbers in US territories have been 666 and 148. At the time of writing this review in November 2019, 15 cases of travel-associated ZIKV infection were reported from the United States so far in 2019, whereas no confirmed cases were reported from US territories in 2019 where a mere 51 cases were presumed to be infected as they only had antibodies to Zika but negative molecular testing for ZIKV. 15 The last nucleic acid amplification test (NAAT)-confirmed case of locally acquired ZIKV infection in the United States was in March 2018. 16
Transmission of ZIKV
Zika virus infection is transmitted to humans mainly through bites of infected mosquito vectors of the genus Aedes. Other non–vector-borne ways of transmission of ZIKV include mother-to-fetus during pregnancy, mother-to-infant during breastfeeding, interpersonal transmission during sexual contact, and transmission by blood transfusion. 2
Vector-Borne Transmission
The life cycle of ZIKV exists in 2 cycles, namely, a sylvatic cycle and urban cycle. In the sylvatic cycle, the virus is maintained between nonhuman primates (monkeys) and arboreal mosquitoes in tropical regions. In the urban cycle, virus circulates between humans and urban mosquitoes. Transmission of ZIKV to humans in urban setting is mainly done by Ae. aegypti Ae. albopictus is also thought to play a role in urban transmission of ZIKV infection and is considered a secondary vector with the potential to cause major outbreaks in the future. 17 ZIKV was isolated from Ae. albopictus mosquitoes as well as from human sera of 5 patients in Gabon, Africa, indicating its possible role in transmission. 7 High rates of dissemination and transmission of ZIKV were observed in study mosquitoes of Ae. albopictus species in Singapore, and these mosquitoes were deemed potentially infectious. 18 Some other species of Aedes mosquito have also been linked to ZIKA transmission such as Aedes hensilli and Aedes polynesiensis. The outbreak in French Polynesia was thought to be caused by Ae. aegypti and Aedes polynesiensis. 19 The vector involved in the epidemic in Yap islands was thought to be Aedes hensilli as it was found to have high rates of infection (86%), as well as high rates of dissemination (23%). 20
Both Ae. aegypti and Ae. albopictus are present in tropical and subtropical regions all over the world. In the United States, Ae. aegypti is found mainly in southern states with southwestern and southeastern states harboring it for longer periods. Ae. albopictus has been found in eastern and northeastern states in addition to southwestern states (Figure 1). Both of these species peak in the months from June to October in the United States and are active during the daytime. Ae. aegypti prefers urban habitats and breeds in stagnant water around homes. An adult female Ae. aegypti feeds predominantly on humans, taking multiple meals per gonotrophic cycle. Ae. albopictus prefers suburban outfields and parks, feeding on humans as well as domesticated animals. 1 In a study from Thailand, both of these species fed on humans and rarely (<1%) on nonhuman hosts (swine, dog, and cat). 21 Ae. aegypti eggs have better survival capability in extreme desiccation, whereas Ae. albopictus can thrive better in colder areas making its expanded distribution toward the north in the United States. 22

Estimated potential range of Ae. aegypti and Ae. albopictus in the United States.
Sexual Transmission
Sexual transmission of Zika was first suspected in the wife of an American male researcher who returned from Senegal in 2008. A few days after unprotected sexual intercourse, the male partner developed headache, maculopapular rash, arthralgia, dysuria, and perineal discomfort. He was noted to have hematospermia. His spouse developed similar symptoms and was found to have positive serology for ZIKV. 23 Presence of ZIKV in semen was confirmed in 2013 in a French Polynesian male who was evaluated for hematospermia and had symptoms consistent with ZIKV infection. RT-PCR detected 3 × 107 copies/mL of ZIKV RNA in his semen. 24
Heterosexual transmission of ZIKV is much more likely to occur if male partner is infected than the other way around, and only one case of female to male transmission has been reported. 25 Penile-vaginal intercourse is much more likely to transmit the infection, although oral and anal intercourse are other possible ways of sexual transmission. 26 ZIKV transmission has also been reported among a homosexual male couple. 27 Only one case of sexual transmission from a vasectomized male to his wife has been reported raising the possibility of presence of ZIKV in fluids from other sources such as prostate, seminal vesicles, bulbourethral glands. 28 The longest period from symptom onset in the index case to potential sexual transmission to a partner was reported to be between 32 and 41 days. 29 It is very difficult to assess the contribution of sexual transmission in areas where vector-borne transmission is very high; however, it is estimated that 1% of cases of ZIKV in Europe and the United States are the result of sexual transmission. 30
ZIKV in Semen
Rates of detection of ZIKV RNA from semen of symptomatic infected men have been consistent in most studies, ranging from 50% to 60% within the first month of onset of symptoms.31 -34 In a prospective study done in Puerto Rico with 117 symptomatic male participants, ZIKV was detected in semen of 48 men (51%). In this study, median time for clearance of ZIKV RNA from semen was 42 days, and 95% of men had undetectable ZIKV RNA in their semen at 120 days after onset of illness. 33 In another study done in the United Kingdom by Atkinson et al, 12 of 23 (52.2%) men with symptomatic ZIKV infection had detectable ZIKV RNA in their semen, 11 of whom were within 28 days of onset of illness. 31
Mead et al found ZIKV RNA in semen of 60 out of 184 (33 %) symptomatic men with ZIKV infection, and it was found more frequently (22/36, 61%) within 30 days after onset of illness. The shedding of ZIKV RNA in semen decreased significantly (≤7%) after 90 days of onset of illness, although there were few cases wherein ZIKV was found in semen even after 6 months of onset of infection, maximum being at 281 days. After controlling for age, this study found that men who ejaculated at least 4 times per week cleared ZIKA from their semen 21 days sooner than who ejaculated at least once a week. Also in this study, only 3 of 19 semen samples positive for ZIKV RNA obtained within 30 days of onset of illness actually had viable ZIKV as demonstrated by growth of virus in VERO cultures. All of these 3 samples had more than 7.0 log10 copies per mL. 32 However, there is evidence that viability of ZIKV and, thus, potential of body fluid transmission of infection may be dependent on other factors such as pH of the fluid, rather than just the concentration of the virus in the fluid. 35 The longest and second longest period reported after which ZIKV was detected in the semen of an infected man is 370 days and 188 days,34,36 although these cases are considered to be outliers of the normal distribution.
Efforts to isolate viable ZIKV from semen after 30 days of onset of illness have mostly not been fruitful, 26 with an exception of successful isolation of ZIKV from semen of a vasectomized man at 69 days from onset of illness. 28 Almost all of the cases of sexual transmission of ZIKV were identified within 20 days of onset of illness of the infected partner. 26 The variable duration of excretion of ZIKA in semen of men is thought to be due to different viral and host characteristics. 28 Older age, presence of conjunctivitis on onset of illness, absence of joint pain, and less frequent ejaculation was independently associated with prolonged excretion of ZIKV in semen. It is estimated that only 1% of semen samples would be positive at 240 days of illness. 32 With limited data about the infectivity of semen, it is safe to say that absence of detectable ZIKV RNA suggest that fluid is very unlikely to be infectious but the exact duration of infectivity of semen with detectable ZIKV RNA is still unknown. 26 This prolonged excretion of ZIKV in semen in various studies indicated tropism of ZIKV for male gonadal cells. The presence of ZIKV in the head of the spermatozoa has been demonstrated with immunohistochemical microscopy. Approximately 3.52% of the spermatozoa were found to be infected with ZIKV in a 32-year-old man. 28
ZIKV in Other Bodily Fluids: Urine, Serum, and Saliva
ZIKA in Urine of Men
Excretion of ZIKV in urine is frequent during the initial period of illness, although it declines rapidly after the first few weeks of onset of illness. 32 One hundred thirty-six of 231 (59%) urine samples were positive for ZIKV RNA by PCR in a study of symptomatic men with ZIKV infection, with the median time until the loss of ZIKV RNA detection being 11 days. Ninety-five percent of these men had undetectable ZIKV in urine after 34 days. 33
In contrast to this, in another study, only 8 out of 214 urine samples obtained from men within 14 to 60 days of onset of illness were positive for ZIKV RNA, and all these 8 positive samples were obtained within 40 days of illness. Interestingly, the number of copies of ZIKV per mL of urine were much lower (median of 2.6 log10 RNA copies per mL) as compared with semen samples (median of 5.6 log10 RNA copies per mL) from the same men. None of the samples in this study that were obtained after 30 days of onset of illness could yield viable ZIKV in urine culture. 32
ZIKV in Serum
As compared with urine, ZIKV is detected in serum for a shorter period. Among 55 patients tested within 5 days of symptoms onset, 31 (56%) were positive for ZIKV RNA by RT-PCR as compared with 52 (95%) from urine. Immunoglobulin M (IgM) was found in serum of only 22 of these patients (40%). Eleven patients were tested after 5 days of symptoms onset, and none of them had positive ZIKV RNA PCR as compared with 9 (82%) positive from their urine samples. 37
ZIKV in Saliva
Zika virus RNA was detected in saliva significantly more frequently as compared with serum of 182 patients in French Polynesia (35 vs 16; 19.2% vs 8.8%), although there was no significant difference in the duration of positivity between the 2 samples. 38 Bonaldo et al demonstrated the presence of viable (infectious) ZIKV in the saliva of Brazilian patients, up to the titer of 80 plaque-forming units per mL. 35 Although saliva functions as a protective barrier for virus entry, 39 a break in the epithelial lining of the oral mucosa or gingival disease may facilitate virus entry into blood. 40 Transmission of ZIKV infection to an Australian traveler after a monkey bite in Bali has been postulated; however, he was also bitten by mosquitoes during his stay. 41
Transfusion-Related Transmission of ZIKV
Zika virus RNA was detected in 42/1505 (2.8 %) of asymptomatic blood donors during the 2013-2014 outbreak in French Polynesia. Eleven of these 42 donors eventually became symptomatic. A similar rate (1.1%) of ZIKV RNA positivity were found in donors in Puerto Rico in 2016. 42 Transfusion-related transmission of ZIKV has been reported in Brazil after both packed red blood cell and platelet transfusion.43 -45 Only 9 of 4 325 889 donors in the United States were confirmed positive for ZIKV between June 2016 and September 2017. 46 Since the majority of the patients with ZIKV infection are asymptomatic, history of possible exposure or ZIKV symptoms may not be a reliable method of screening donors. The US Food and Drug Administration (FDA) has issued revised guidelines for screening of donors of blood and blood components in July 2018. All blood donations collected in the United States and its territories should be tested with licensed NAAT for ZIKV, or else blood components (platelets and plasma) should be collected and prepared using pathogen reduction technology with an FDA-approved pathogen reduction device. 47
Maternal-Fetal Transmission and ZIKV Infection in Pregnancy
Vertical transmission of ZIKV can occur in all 3 trimesters of pregnancy regardless of the presence or absence of symptoms in the mother. 2 Approximately 26% of infected mothers transmit ZIKV to their fetuses. 48 However, the risk of developing birth defects, including neurological abnormalities, was highest among women who were infected during the first trimester. 49 In contrast, the risk of fetal neurological complications was found to be lowest among pregnant females who acquired ZIKV infection during third trimester of infection. 50 Although ZIKV infection of the fetus of the mother who acquired ZIKV after sexual intercourse has been reported, it is not clear if the risk of fetal infection is higher through sexual transmission to mother than vector-borne transmission to mother. 51 ZIKV has been detected in breast milk, but this mode of transmission has not been documented. And therefore, World Health Organization recommends mothers with possible or confirmed ZIKV infection to continue breastfeeding. 52
Clinical features of ZIKV infection in pregnant females are similar to those in nonpregnant adults. Common symptoms in pregnant females include maculopapular rash (44% to 93%), conjunctivitis (36% to 58%), myalgia/arthralgia (39% to 64%), headaches (53% to 62%), and lymphadenopathy (40%). 53 The rash was pruritic in 90% of the ZIKV-infected pregnant women in one large prospective study. The illness is self-resolving, lasting up to 7 days as in nonpregnant patients. One case of GBS in a pregnant woman has also been reported. 54
ZIKV Infection in Nonpregnant Adults
The incubation period of ZIKV infection ranges from 3 to 14 days, and the majority (50% to 80%) of those infected are asymptomatic. Most of the patients experience mild illness marked by rash, low-grade fever, arthralgia, myalgia, and conjunctivitis that can last up to 1 week.6,55-58
Congenital ZIKA Syndrome
Zika virus causes a constellation of fetal and birth defects known as congenital Zika syndrome (CZS), affecting mainly central nervous system along with other systems. Several studies and reports estimate the risk of CZS to be 5% to 14%.49,50,59 -62 However, Brasil et al found a large proportion (36/117, 42%) of babies to have abnormal clinical or radiological findings at birth. 63 Manifestations of CZS mainly stem from the neurotropic nature of the virus. 64 CZS has been mainly divided into structural and functional lesions and their related manifestations. The fetal brain disruption sequence is a spectrum of lesions that is very specific for CZS and is rarely seen in other congenital infections. It constitutes microcephaly, collapsed skull, premature closure of fontanels, overlapping sutures, and redundant scalp skin. Other structural lesions of CZS include subcortical calcifications, decreased myelination, ventriculomegaly, cerebellar hypoplasia, intrauterine growth restriction, congenital contractures, and neuronal migration disorder (agyria, pachygyria, polymicrogyria, dysgenesis of corpus callosum, and lissencephaly). 2 Several ocular structural lesions are seen in CZS, including macular scarring, glaucoma, optic nerve atrophy, intraocular calcifications, microphthalmia, anophthalmia, iris coloboma, lens subluxation, and cataract. Chorioretinal atrophy and pigmented retinal mottling are very specific for CZS. 2
Functional lesions and manifestations of CZS comprise seizures, visual impairment, hearing loss, and developmental delay. Pyramidal and extrapyramidal lesions are manifested as hypertonia, swallowing disorder, movement abnormalities (dyskinesia, dystonia), impatient crying, hyper excitability, and sleep disorders. 2 Neonatal mortality during the first week of life of babies born with CZS ranges from 4% to 7%.48,63
CZS in the United States
A large study was done wherein 1450 children aged ≥1 year born to mothers from all US states, the District of Columbia, US territories, and US freely associated states (American Samoa, Federated States of Micronesia, Marshall Islands, Puerto Rico, and the US Virgin Islands) with confirmed or possible ZIKV infection and who were registered in the US Zika Pregnancy and Infant Registry (USZPIR) were followed-up. Eighty-seven (6%) had ZIKA-associated birth defects (intracranial calcifications, congenital microcephaly, cerebral atrophy, abnormal cortical formation, corpus callosum abnormalities, cerebellar abnormalities, porencephaly, hydranencephaly, ventriculomegaly, hydrocephaly, microphthalmia, coloboma, cataract, intraocular calcification, chorioretinal anomalies, and optic nerve atrophy). Nine percent (136/1450) of them had ≥1 neurodevelopmental abnormality possibly associated with congenital ZIKV infection with or without the above-mentioned birth defects. These neurodevelopmental abnormalities included hearing abnormalities, congenital contractures, seizures, body tone abnormalities, movement abnormalities, swallowing abnormalities, possible developmental delay, visual impairment, and postnatal onset microcephaly. With the overlap of these 2 outcomes, a total of 14% of babies born to ZIKV-infected mothers were found to be affected. 62
Microcephaly and ZIKV
In a prospective study of ZIKV-positive pregnant women in Rio de Janeiro, microcephaly was noted in prenatal ultrasound and confirmed at birth in 4/117 (3.4%) live births. 63 Similar rates of microcephaly at birth (43/972, 4.4%) were noted in a report of fetal outcomes of completed pregnancies of 972 ZIKV-infected women registered in US Zika Pregnancy Registry. 59 In the previously mentioned USZPIR report of 1450 infants, 20 additional cases of microcephaly (postnatal-onset) were identified during the first 24 months of life, increasing the rate of microcephaly from 4% (64) to 6% (84), thus highlighting the postnatal role of ZIKV infection in hampering brain growth that was originally within normal size limits at birth. 62
Pathophysiology of ZIKV in CZS
Once introduced into the human body, ZIKV invades and persists in many target host cells including skin, blood, placental cells, retina, and neural stem cells, and progenitor cells of placental, neural, and gonadal tissues.65,66 Tropism of ZIKV for neural stem cells and progenitor cells has been described. 67 ZIKV gains access to host cells through Axl receptors present on the host cell membrane. The life cycle of ZIKA in host cells has 4 steps: (1) translation of viral proteins, (2) replication of ZIKV RNA, (3) assembly of viral particles in the endoplasmic reticulum (ER), and (4) release of virion from the host cell. ZIKV encodes for 3 structural proteins, namely, capsid (C), envelope (E), and prM; and 7 nonstructural proteins: NS1, NS2A, NS2B, NS3, NS4A, NS4B, and NS5. The structural proteins of prM and E are required for attachment to host neural cell membrane. The C protein and nonstructural proteins localize to various organelles in the neuron including nucleus and its nucleoli, Golgi apparatus, and lipid droplet in cytoplasm, causing cell cycle arrest, apoptosis, and cell death.65,68 Nonstructural proteins NS4A and NS4B play a role in virus replication and assembly. 65
Zika virus has been demonstrated to cause host cell DNA damage by causing double-strand breaks and halt the host cell in its S phase, thus preventing its replication. These cellular effects have been postulated to cause growth arrest of fetal neural cells in the cortex and lead to a poorly developed brain noted in ZIKV-infected fetuses. 69 In addition to this, ZIKV is thought to evade human cellular defense through its nonstructural proteins–mediated interferon antagonism or by decreasing the production of interferons, which are responsible for inhibiting ZIKV replication in human cells. Multiple other evasion mechanisms of ZIKV have been identified that are carried out by ZIKV mainly by inhibiting innate cellular immune pathways. 66
Complications of ZIKV in Older Children and Adults
The neurological complications of ZIKV infection include development of GBS, transverse myelitis (TM), and acute disseminated encephalomyelitis (ADEM). These complications of ZIKV infection can be seen concomitantly or shortly after the onset of infection (parainfectious) because of direct viral neurotropism, or can occur after a period of latency (postinfectious) resulting from immune-mediated reactions against virus. A mean latency period of 10.5 days (range = 1-96 days) was found in review of 19 cases of TM, encephalitis, and ADEM. 70 Several cases of TM and ADEM associated with ZIKV infection have been reported.71 -76 In one report of TM after ZIKV infection, anti-myelin oligodendrocyte glycoprotein antibody against the myelin sheath was detected, favoring an autoimmune-mediated neurotoxicity. 75 The role of preexisting immunity to other arboviruses (CHIKV and DENV) from prior infection leading to augmented auto-inflammatory response against the neural tissue after subsequent ZIKV infection was hypothesized in a patient who developed ADEM and GBS after ZIKA infection. 70 Magnetic resonance imaging of brain and spinal cord in a majority of these cases showed multifocal subcortical lesions and spinal cord lesions at various levels visualized as hyperintense signal on T2 sequences.70 -78 ZIKV infection has also been reported to cause transient polyneuritis marked with distal weakness, stocking-glove hypoesthesia, and hyporeflexia acutely within 1 to 2 days of ZIKV symptom onset. The direct neuropathic effect of ZIKV leading to inflammation and nerve swelling was thought to be the pathophysiology of this quick onset of symptoms. 79
ZIKV Infection and GBS
The first case of GBS associated with ZIKV was reported from French Polynesia during the outbreak in 2013. 80 The incidence of GBS associated with ZIKV infection is estimated to be 2 to 2.4 per 10 000 cases of ZIKV infection.81,82 In comparison, the estimated incidence of GBS associated with Campylobacter jejuni infection is estimated to be 2.5 to 6.5 cases per 10 000 infections. 83 GBS associated with ZIKV has been found to occur sooner after the infection onset (6-10 days) as compared with occurring little later (up to 4 weeks) after other triggering infections. 77 Nerve conduction evaluation done on GBS patients associated with ZIKV infection have yielded mixed results, showing predominantly acute motor axonal neuropathy in a study done in French Polynesia 82 and acute inflammatory demyelination polyradiculopathy in 2 other studies conducted in Brazil and Columbia.71,84 Mechanical ventilation was needed for almost one third of the affected patients.82,84 Prognosis of GBS after ZIKV infection is favorable. Two major studies showed close to 60% of patients becoming ambulatory at 3 months.71,82
Other Complications Associated With ZIKV Infection
Transient myocarditis was diagnosed in a 45-year-old French man who acquired ZIKV infection during his travel in La Martinique (French Caribbean). The patient had symptoms of fever, conjunctivitis, joint pains, and squeezing chest pain. Laboratory evaluation revealed elevated troponins and elevated creative phosphokinase. He was noted to have ST segment elevation on electrocardiogram and hypokinesia of inferior-medial wall on echocardiogram. PCR for ZIKV RNA and anti-ZIKA IgM was found to be positive from his blood 5 days after onset of his symptoms. 85 ZIKV has also been isolated from cardiac tissue of infected nonhuman primates. 86 ZIKV infection has been reported to be associated with atrial fibrillation in a previously healthy (with no history of cardiac illness) 49-year-old man from Brazil who was admitted with hypertensive crisis (blood pressure of 240/120 mm Hg) and was noted to have symptoms compatible with ZIKV infection. Patient developed atrial fibrillation during his hospital stay that was treated with amiodarone. RT-PCR was positive from his saliva. 87
Diagnosis of ZIKV Infection
Zika virus RNA is likely to be detected in serum of infected patients approximately 2 days before to 1 week after onset of symptoms; however, this duration may be prolonged in pregnant patients. IgM are detectable during the first week of illness; however, the duration of their persistence in serum is precisely unknown. Furthermore, different flaviviruses exhibit cross-reactivity of IgM antibodies, thus making interpretation of IgM test result very difficult. IgG is detectable shortly after appearance of IgM and generally persists lifelong. Among patients living in flaviviruses endemic areas with previous infection with flaviviruses, a subsequent infection with another flavivirus may produce IgG against multiple flaviviruses very rapidly, thus limiting the value of checking IgG in such patients.5,33,37,88 Plaque reduction neutralization tests (PRNTs) are quantitative assays that measure virus-specific neutralizing antibody titer against dengue, ZIKA, and other flaviviruses. 89 In general, for patients with suspected ZIKV infection, NAATs are the preferred method of evaluation. 90
The Centers for Disease Control and Prevention has developed and periodically updated diagnostic algorithms and guidelines for interpretation of test results for evaluation of ZIKV infection in patients with a clinically compatible illness and relevant epidemiologic exposure.90,91 CDC’s definition of possible ZIKV exposure includes travel to or residence in an area with risk for mosquito-borne ZIKV transmission or sexual contact with a partner who has traveled to or resides in an area with risk for mosquito-borne ZIKV transmission. These areas can be found on webpage: https://wwwnc.cdc.gov/travel/page/world-map-areas-with-zika.
Diagnosis of ZIKV in Nonpregnant Patients With Clinical Compatible Illness
As the clinical presentation of ZIKV and DENV infection are very similar and the epidemiology of these 2 illnesses is overlapping in the United States, CDC has developed a surveillance case definition of ZIKV infection. ZIKV infection should be considered in a patient with a fever, rash, arthralgia, or conjunctivitis who lives in or has recently traveled to an area where there is risk of infection with Zika. NAATs should be done within 7 days of onset of symptoms on any one of the plasma, whole blood, cerebrospinal fluid (CSF), or urine. Positive NAAT is indicative of acute infection, and serology is not indicated in such cases. However, a repeat NAAT should be performed in cases of clinical or epidemiologic significance (first local transmission, unusual clinical syndrome, or new transmission mode) to rule out false-positive results. ZIKV viremia may resolve over time. Therefore, in patients where sample is obtained after 7 days of onset of illness and patients with negative NAAT on samples obtained within 7 days of illness, ZIKV IgM serology should be performed. Negative NAAT followed by negative IgM indicates no evidence of ZIKV infection. If IgM is positive, PRNT should be performed to confirm the diagnosis. PRNT titer of ≥10 against ZIKA is considered diagnostic. A negative PRNT rules out ZIKV infection, and positive IgM in such a case implies another recent alternate flavivirus infection or false positive (Figure 2). 90
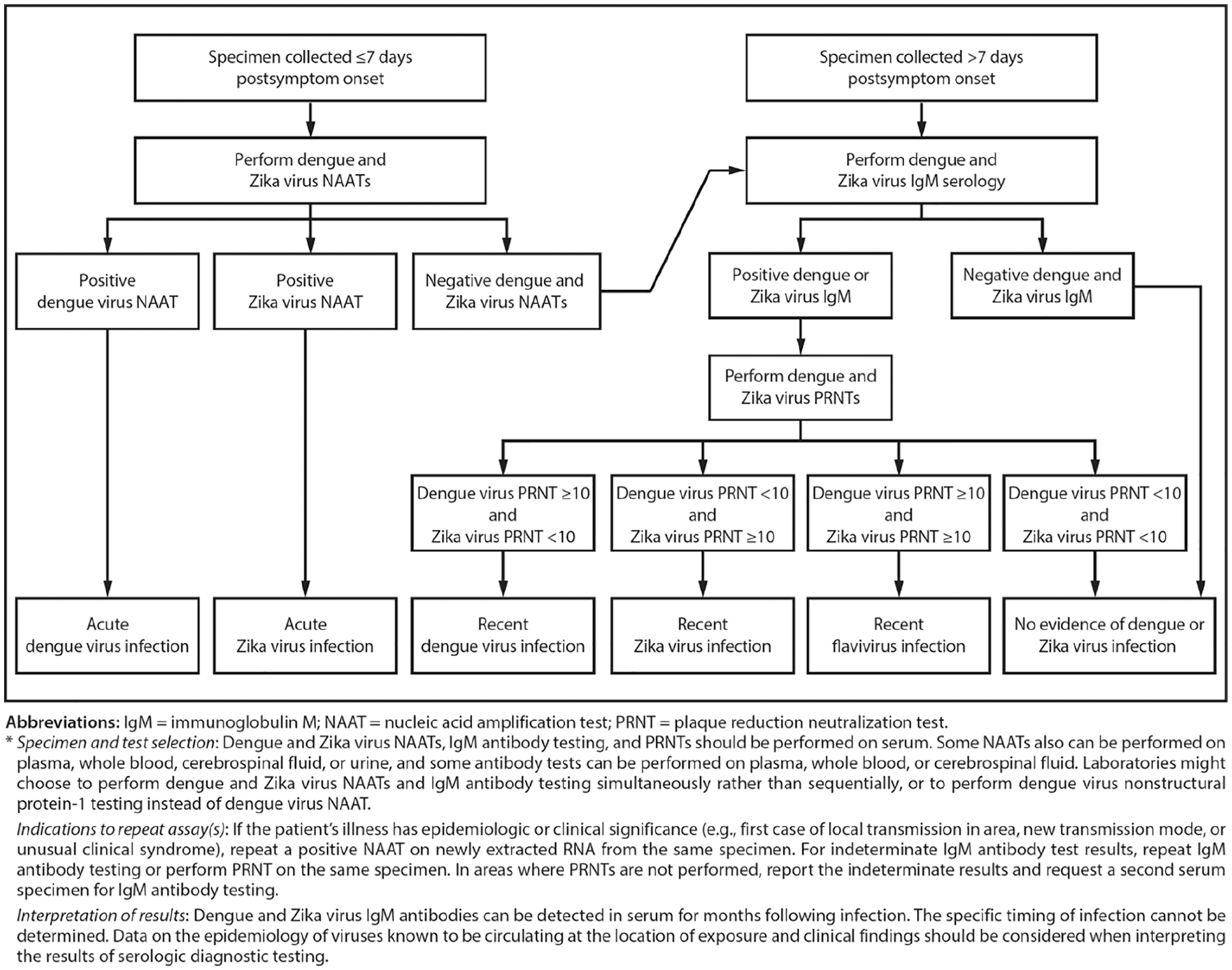
Dengue and Zika virus testing recommendations for nonpregnant persons with a clinically compatible illness and risk for infection with both viruses*.
Diagnosis and Management of Symptomatic Pregnant Females With Possible ZIKV Infection
Pregnant women with clinically compatible illness with ZIKV infection should have concomitant testing for dengue and ZIKV. Both NAAT and serology for IgM should be done on serum, and NAAT should also be done on urine sample for both viruses. Specimens should be collected within 12 weeks of symptom onset. NAATs and IgM antibody testing can also be performed on plasma, whole blood, and CSF, whereas amniotic fluid can be used for NAAT only. A positive NAAT on both serum and urine indicates recent infection; however, if only one sample has positive NAAT and IgM is negative, then NAAT should be repeated on freshly extracted RNA from the same specimen to rule out false-positive results. If both dengue and ZIKV NAATs are negative and either IgM is positive, then confirmatory PRNT should be done to check for dengue, ZIKV, and other flavivirus that are endemic in the area of possible exposure. IgM antibody testing should be repeated on the same specimen, or PRNT should be performed for cases with indeterminate antibody testing. 90 As IgM can persist for a long period after infection, it can be difficult to determine if infection occurred before or during the pregnancy. This is further complicated by the fact that antibodies can cross-react among various flaviviruses. 91 Thus, if IgM antibody is positive for one virus but the testing was not done for the other virus, the case should be labeled as presumptive flaviviruses infection. A negative NAAT followed by negative IgM indicates no evidence of ZIKV or dengue infection. If IgM is positive, PRNT should be performed to confirm the diagnosis. PRNT titer of ≥10 against ZIKA is considered diagnostic. A negative PRNT for ZIKV and dengue rules out these 2 infections, and positive IgM in such a case implies another recent alternate flavivirus infection or false positive. 90
Management of Asymptomatic Pregnant Females With Possible ZIKV Exposure
Since the prevalence of ZIKV in the Americas has been decreasing, CDC has updated and published guidance for testing of asymptomatic pregnant women with possible exposure to ZIKV (Figure 2). 91 CDC recommends that all pregnant women in the United States and US territories should be asked at every prenatal care visit about possible ZIKV exposure before and during the current pregnancy.
Asymptomatic pregnant women with ongoing possible ZIKV exposure should be offered NAAT testing 3 times during pregnancy, although the optimal timing and frequency of testing with NAAT alone is not known. For such cases, IgM antibody testing is not routinely recommended as it can persist for months after infection and may not be able to reliably determine if an infection occurred during the current pregnancy or before the current pregnancy. If initial NAAT test done during early stages of pregnancy is negative, 2 more tests should be done during the course of pregnancy on the days of prenatal visits. 91
For asymptomatic women with possible ZIKV exposure during the current pregnancy or periconceptional period (8 weeks before conception or 6 weeks before the last menstrual period), ZIKV testing is not routinely recommended. For such cases, communication between the obstetric care provider and the pediatrician regarding possible maternal exposure to ZIKV is very critical for early identification of infants who are born without clinical findings of infection but may develop manifestations of CZS later. If these asymptomatic women have fetuses with ultrasound findings consistent with CZS, they should be tested for ZIKV infection with both NAAT and IgM to establish the etiology of the fetal findings. Postnatal testing of placental and fetal tissue can be performed for women who did not have laboratory confirmed diagnosis of ZIKV and if their infants or fetuses have clinical findings consistent with CZS. IgM testing of nonpregnant women before conception to establish their baseline status is not recommended for women with ongoing possible risk of ZIKV exposure. 91
Management of Infants With Possible Congenital ZIKV Infection
For infants who are born with findings consistent with CZS, NAAT of both blood and urine for ZIKV should be done. Additionally, testing of CSF (if available) with NAAT should be considered. IgM can also be checked in serum and CSF (if available) to diagnose CZS. If both PCR and IgM are negative within first few weeks of life, diagnosis of ZIKV infection is unlikely. If this differentiation cannot be ascertained in an infant, he or she should be evaluated as a case of congenitally acquired infection. Alternate etiologies of the congenital findings should also be evaluated. Such infants should get head ultrasound, comprehensive ophthalmologic examination, and auditory brainstem response by the age of 1 month. Consultation with pediatric infectious disease specialist, clinical geneticist, pediatric neurologist, and other relevant specialists should be considered. 92
Testing of cord blood is not recommended as it may yield false-positive and false-negative results. Testing of an infant should be done as soon as possible, preferably within first few days of life as levels of IgM decline over time. If testing of infants is delayed, differentiation of congenital infection from postnatal infection may be difficult in infants who are from areas with ongoing transmission of ZIKV. An infant with positive IgM and negative PCR result is considered as probable CZS. An infant with nonnegative IgM (positive, equivocal, presumptive positive, or possible positive) should undergo ZIKV-specific PRNT that measures virus-specific neutralizing antibodies. If PRNT is negative, congenital ZIKV infection is unlikely and it indicates false-positive IgM in an infant. However, a positive PRNT may be seen in an infant due to passive transfer of maternal antibodies to infant, which become undetectable by age of 18 months. PRNT should be repeated for infants with positive PRNT at age ≥18 months, which might help confirm or rule out congenital ZIKV infection. If PRNT is positive in an infant at age ≥18 months, congenital ZIKV infection is presumed, except for infants living in or traveling to areas with risk of ZIKV transmission who could have acquired postnatal infection. If PRNT is negative at age ≥18 months, congenital ZIKV infection is unlikely. Infants who are born with physical findings consistent with CZS and positive maternal tests during pregnancy indicating possible ZIKV infection, PRNT at age ≥18 months could be considered if their NAAT or IgM were negative at birth or if testing was not done at birth. 92
Prevention of Sexual Transmission
The CDC now recommends that couples who are planning to conceive in whom only the male partner is at risk of ZIKV exposure (due to travel to area with Zika risk) abstain from sex or use condoms for 3 months after symptom onset (if symptomatic) or possible ZIKV exposure (if asymptomatic) before engaging in unprotected sex. If the female partner is the one who is traveling to an area with ZIKA risk, then the couple should use condoms or abstain from sex for at least 2 months after the female partner’s symptom onset (if symptomatic) or last possible ZIKV exposure (if asymptomatic). If both partners are traveling to areas with risk of ZIKV exposure and are planning to conceive, they should abstain from sex or use condoms for 3 months after the male partner’s symptom onset (if symptomatic) or the male partner’s possible exposure (if asymptomatic) before engaging in unprotected sex. For couples who are already pregnant and male partner is at risk of exposure to ZIKV, such couples should consistently and correctly use condoms during sex or abstain from sex for the duration of pregnancy. For couples who are not planning to conceive, men can consider using condoms or abstaining from sex for at least 3 months after symptom onset (if symptomatic) or after their possible ZIKV exposure (if asymptomatic) to minimize their risk for sexual transmission of infection. If one or both partners have ongoing exposure to ZIKV (living in area or frequently travel to area with risk of exposure), the couples should talk with their health care provider and discuss their plans, risk of ZIKV infection, possible outcomes of the baby if infected, and ways to protect themselves from infection. If either partner of such couples develops symptoms compatible with ZIKV infection, the couple should follow suggested time frames mentioned above before trying to conceive. 93
Prevention of Vector-Borne Transmission
The CDC recommends that pregnant women should not travel to areas with risk of ZIKV transmission. These areas can be found on webpage: https://wwwnc.cdc.gov/travel/page/world-map-areas-with-zika. All travelers and residents of such area should be advised to follow preventative measures to avoid mosquito bites. Protection from mosquito bites is required throughout the day as mosquitoes of Aedes sp bite mostly during the day. Mosquito bites can be prevented by wearing long-sleeved shirts, pants, permethrin-treated clothing, and using US Environmental Protection Agency–registered insect repellents. Insect repellents containing DEET, picaridin, and IR3535 are safe for use during pregnancy when used in accordance with the product instructions. Persons infected with Zika should protect themselves from mosquito exposure during the first week of illness to decrease chances of human-to-mosquito-to-human transmission. Other preventative measures include emptying of the standing water from containers, installing screens on windows and doors, and using air conditioners. 94
Immunity and Vaccines for ZIKV
Even though ZIKV has 2 lineages (African and Asian/American), in animal studies, it was found to behave as a single serotype with limited strain variability, inducing a similar immune response and providing cross protection for the other lineage. This property of ZIKV allows development of a monovalent vaccine that can render protection against both strains. 95 Several complex immune pathways (cellular vs humoral) have been postulated, leading to development of different types of platforms for ZIKV vaccines. 96 These platforms include purified inactivated whole virus vaccine, live-attenuated virus vaccine, recombinant subunit vaccine, nucleic acid vaccine (single plasmid containing DNA vaccine, self-replicating RNA vaccine, and mRNA vaccine), and viral-vectored vaccine. More than 10 vaccine candidates are in phase-I clinical trial currently and one is undergoing phase-II clinical trial.97,98
As women of reproductive age are the primary target population and a theoretical risk of live, attenuated, or replication competent viral vaccines given to pregnant women may be capable of crossing the placenta and potentially infect the fetus, a nonreplicating vaccine platform with no safety concerns for its use during pregnancy would be an ideal platform for ZIKV vaccine. Vaccines based on replication-competent platforms appear to be more suitable for routine vaccination of nonpregnant personnel to decrease endemic transmission.98,99
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval and informed consent was not needed for this article as this is a review article. All the references have been duly cited and credit has been given to the source (Centers f or Disease Control and Prevention) of both the figures in the article.