
Abstract
Objective. Triage in resource-limited settings (RLS) improves outcomes. Emergency Triage Assessment and Treatment (ETAT) is a simple triage algorithm that improves assessment and initial management of children in RLS. In Belize, pediatric triage varies with setting, from a 5-level Emergency Severity Index (ESI) used at the National Referral Hospital to a lack of triage at government health centers (GHC). Most data on ETAT implementation are in settings where no triage system existed; data on how to integrate ETAT into existing, heterogeneous triage systems are lacking. The aim of this study is to explore health care providers’ (HCPs) attitudes toward the current triage system prior to national pediatric triage process implementation. Methods. A qualitative study was performed via convenience sampling of HCPs who participated in an ETAT training course using focus groups immediately and 1 year after an initial ETAT training. Focus groups were digitally recorded and transcribed. Three coders analyzed all transcripts to identify emerging themes. Constant comparison analysis was performed until achieving thematic saturation. Results. The following principal themes emerged: (1) importance of triage education and implementation to standardize and improve communication; (2) major limitations of ESI include its complexity, lack of pediatric-specific criteria, and dependence on equipment not consistently available; and (3) desire to implement a simple, low-resource pediatric-specific triage system. Conclusions. Participants believe triage education and process implementation is essential to improve communication and pediatric emergency care. Simple, low-resource pediatric-specific triage systems, like ETAT, may improve utilization by providing faster recognition and improved care for acutely ill children.
Keywords
Introduction
Effective triage is crucial to improving outcomes in children. In resource-limited settings (RLS), the lack of triage systems can result in delays in care.1-9 The Emergency Triage Assessment and Treatment (ETAT) guidelines and triage process were developed by the World Health Organization as part of the Integrated Management of Childhood Illnesses program to promote improved assessment, triage, and initial management of acutely ill children in resource-limited hospital-based settings.10-12 Most studies of ETAT implementation have been conducted in resource-limited settings where no prior triage system exists. Those studies show that ETAT is not only an effective triage screening tool, but that process implementation also leads to decreased admission rates, decreased inpatient length of stays, and decreased mortality.9,11-13 No studies, however, have addressed if ETAT is applicable in RLS with an existing triage system. This distinction is crucial as many available triage systems are not pediatric specific and can lead to difficulties in triage classification for the pediatric population. 14
In Belize, pediatric triage practice varies with setting. The only public tertiary referral hospital in Belize (Karl Heusner Memorial Hospital Authority [KHMHA]) uses the 5-category Emergency Severity Index (ESI), while the government polyclinics and health centers (GHC) have no formal pediatric triage process. A prior needs assessment identified a demand for a triage system that adequately addressed the needs of the pediatric population for the Department of Accident and Emergency (A&E) at KHMHA, and ETAT was identified as a possible solution. The objective of this study was to explore health care providers’ (HCPs) attitudes and perceived barriers to the current triage system in an RLS after an ETAT training course.
Materials and Methods
Study Design and Setting
This was a qualitative study assessing the attitudes toward the emergency triage system in Belize utilizing focus groups. The study was conducted at KHMHA, a tertiary-level public hospital under the direction of the Belizean Ministry of Health (MoH) in Belize City, the largest city in Belize. KHMHA serves as the only public referral hospital for the entire country (population: ~390 000; 34% <15 years old). 15 In Belize, the crude mortality rate is 4.5/1000, and the mortality rate for children <5 years old is 17.8/1000 live births. 16 This referral hospital’s A&E evaluates ~6800 children aged 0 to 14 years annually. The A&E is open 24 hours/day and is staffed primarily by 3 to 4 general physicians and 6 to 9 nurses per shift, depending on time of day. KHMHA inpatient pediatric services include a 15-bed inpatient medical pediatric ward, a 5-bed surgical pediatric ward, a 23-bed neonatal intensive care unit, and 7-bed pediatric intensive care unit. The average admission rate to the pediatric ward from the A&E is 6.8% and all subspecialty needs are met at KHMHA.
Belize has a tiered public health care system. Primary care is provided by the network of 28 polyclinics, health centers, and health posts. Polyclinics provide outpatient general and specialized services such as pediatrics and obstetrics and gynecology. Polyclinics and health centers are staffed by physicians and nurses and provide services such as prenatal care and immunizations. Health posts are usually staffed by nurses and provide health education as well as treatment for minor ailments. These services are available Monday through Friday, 8
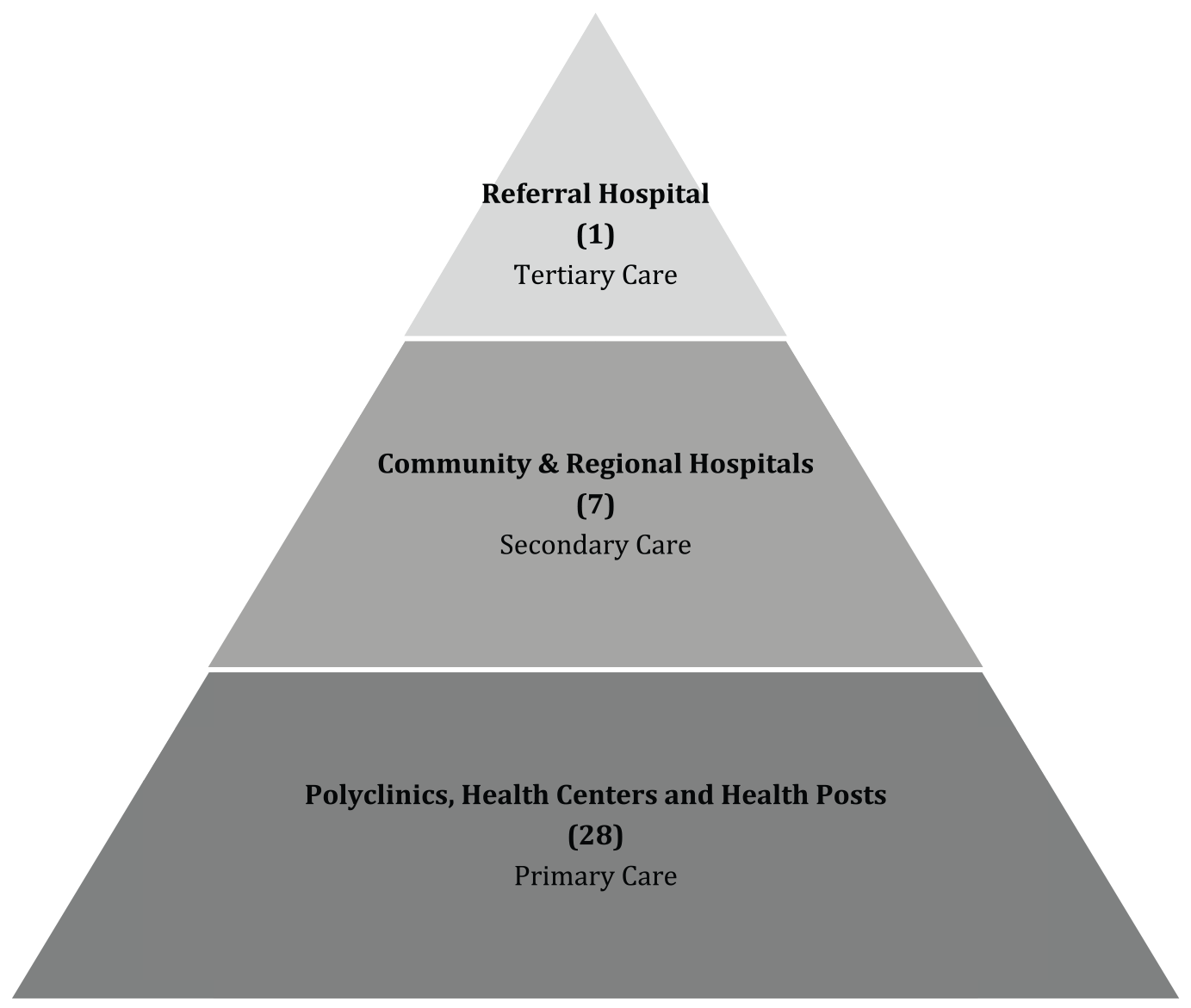
Tiered public health care system of Belize.
ETAT training was provided by a team of pediatric emergency medicine and emergency medicine physicians from Baylor College of Medicine who had taken the ETAT Training of Trainers course, led by one of the researchers (HLC), who developed and published the teaching materials for the ETAT course for the World Health Organization. Pediatric emergency medicine nurses from Texas Children’s Hospital were recruited to facilitate skills stations with these physicians.
Focus groups were held immediately after the initial ETAT training in February 2016. A second set of focus groups were conducted 1 year following the training in February 2017. During this 1-year interval, additional HCPs from KHMHA and the GHCs were provided ETAT training, but formal system-wide ETAT triage process implementation had not yet occurred. All focus groups were held at KHMHA prior to initiation of nationwide pediatric triage training.
Ethical Approval and Informed Consent
Institutional review board approval was obtained from Baylor College of Medicine (IRB #H-38442). As there is no institutional review board in Belize, approval from the Board of Directors from KHMHA was also obtained. Written informed consent was obtained from all focus group participants.
Selection of Participants
Focus groups were composed of a convenience sample of pediatric HCPs from both KHMHA and 3 of the Central Region’s GHCs who attended a 2-day ETAT Participant Course in February 2016. We conducted 6 focus groups with all available pediatric HCPs from KHMHA and the GHCs who participated in ETAT training immediately following the training and 1-year post-training. All ETAT training participants were invited to join the focus groups. The first focus groups (4 total) were held immediately after ETAT training and ranged in size from 3 to 5 HCPs with ~40% of trainees participating in the focus groups. The second focus groups (2 total), were conducted 1 year after ETAT training, with 25 total HCPs (~63% participation). Availability was dependent on HCPs’ personal and/or professional schedules. Focus group duration ranged from 30 minutes to 70 minutes, with no specific end time, allowing for a natural conclusion of conversation.
KHMHA personnel were identified by the hospital administration and included physicians and practical and registered nurses from the pediatric and A&E ward. GHC personnel were identified by the MoH and included general physicians and practical and registered nurses. Registered nurses have a minimum of 4 years of university education following high school, while practical nurses train for 12 to 18 months after high school.
Outcome Measurements
The first set of focus groups was conducted immediately following ETAT trainings to assess participants’ knowledge about their current triage system and to identify the advantages and barriers to their current triage system. We also discussed their perceptions of the utility, if any, in implementation of an ETAT-based triage system at their institutions. The second set of focus groups were conducted 1-year after the ETAT training and focused on how individuals have implemented ETAT into their personal practice since their training. An experienced, ETAT-trained moderator (AEG) facilitated the focus groups using a standardized script, with prompts for deeper exploration, to ensure all areas of the triage process were explored throughout the study.
Analysis
All focus groups were audio-recorded and transcribed in English, Belize’s official language. After compilation of all transcriptions (AEG), 3 researchers (AEG, EMS, HLC) independently coded the transcriptions from each time point using an iterative coding process to identify patterns of responses, ensure reliability, and examine discrepancies through thematic analysis. Rigorous memos of coding decisions were kept, providing consistency in coding as the coding progressed. The codes were then categorized, and emerging themes were identified. Thematic analysis was performed until content saturation was achieved. Member checking occurred to ensure trustworthiness. Demographic information was provided by participants and verified by KHMHA administrative staff.
Results
There was a total of 6 focus groups during the study period. During the first study period, 42 HCPs participated in the initial ETAT training in February 2016. Of that group, 16 HCPs (7 physicians and 9 nurses) participated in 4 focus groups. During the second study period in February 2017, 25 HCPs (16 physicians and 9 nurses; 11 [44%] from first focus groups) participated in 2 focus groups 1 year later (Table 1). Three principle themes emerged: (1) the importance of triage education and implementation to standardize and improve communication; (2) major limitations of ESI include its complexity, lack of pediatric-specific criteria, and dependence on equipment not consistently available; and (3) desire to implement a simple, low-resource pediatric-specific triage system (Table 2).
Participant Demographics.

Abbreviations: KHMHA, Karl Heusner Memorial Hospital Authority; GHC, government health center.
Principal Themes With Illustrative Quotes.

Communication
For the initial focus groups, one of the principal themes that emerged regarding current triage systems was the importance of triage education and implementation to standardize and improve communication by using a unified language between HCPs. HCPs wanted a “universal language” to use in triage that everyone could understand. One year after ETAT training, although there has not been formal system-wide ETAT implementation, participants from KHMHA believe ETAT training improves communication between HCPs and strengthens their relationships because they are “on the same page.” This communication facilitates prompt and efficient care for patients.
Limitations of Current System
Government health centers expressed “frustration” with lack of triage and its impact on patient care in that “you have patients that get worse” while waiting. At KHMHA, many participants noted that the major limitations of ESI included the difficulties of assessing pediatric patients due to the system’s lack of pediatric-specific criteria as well as dependence on equipment that is not consistently available such as pulse oximeters and thermometers. Additionally, determining triage level using ESI is challenging as patient’s triage level reflects the anticipated need for resources that may not readily be available (eg, specialty consultation, laboratory studies, imaging). They believed the ESI triage categories overlapped and there were “gray” areas.
Pediatric Triage Implementation
Another theme that emerged was the desire to implement a simple, low-resource pediatric-specific triage system. It was important for providers to learn to differentiate “between a sick and not so sick child” and to identify “priority” signs. GHCs expressed needing “structure” and interest in implementing ETAT. They believed it was helpful and more “efficient.” One year following ETAT training, individuals at the GHCs are using ETAT independently with qualitative success stories want to continue trainings and formalize ETAT-based triage implementation. They believed ETAT was valuable particularly to “prioritize” pediatric patients when there were long wait times.
At the referral hospital, KHMHA, pediatric HCPs believe ETAT allows them to triage children more effectively than ESI alone, given the simple algorithm and pediatric focus. Participants believe they have “less complaints” and experience “improved service delivery” and patient satisfaction anecdotally. There is interest in creating a hybrid system that would incorporate ETAT triage signs into their current ESI-based system.
Discussion
Quick and efficient triage of pediatric patients improves morbidity and mortality worldwide. In RLS, ETAT has helped improve pediatric outcomes by training HCPs to recognize and initiate treatment for critically ill children through triage process implementation. Despite using the ESI, which has been shown to be a reliable pediatric triage tool, 17 HCPs in Belize underscored the desire for a triage system with more pediatric-specific criteria that does not rely heavily on equipment for it to be useful in settings where this equipment is not readily available. This may reflect that the ESI is designed to be used, and therefore would be valid, in a resource-abundant setting. 18
Participants also feel that triage education and implementation facilitate appropriate and timely care of patients. This finding is similar to that of a study of US emergency room nurses that identified lack of trained staff as a hazard to triage decision-making and emphasized the need for continued triage education.
Participants note the triage education and implementation improves communication among providers. Additionally, participants from the GHCs note that ETAT improves efficiency and reduces waiting times for patients. For participants from KHMHA, ETAT strengthens the already existing ESI-based triage system, enhancing their ability to care for children. These findings have not been shown in previous literature.
Limitations
There were several limitations to our study. First, the population is a small convenience sample and does not include key stakeholders such as hospital and MoH administrators. Additionally, no HCPs from the private sector were included so we do not have data regarding their triage practices or attitudes. Therefore, not all attitudes regarding triage practice are represented. Due to the unique study population, the results may not be generalizable to other settings. Also, we conducted the first focus groups after ETAT training, possibly introducing bias. Despite the small, nonrepresentative sample, member checking was conducted to ensure trustworthiness.
Future Directions
As a result of the positive provider buy-in, perceived improvement in pediatric emergency care and patient/parental satisfaction, KHMHA, with the support of the Ministry of Health of Belize and the local chapter of the Pan-American Health Organization, are collaborating to rollout a phased countrywide educational initiative to train all pediatric providers within the government health care system in ETAT. Also, to encourage consistency of care, ETAT training will be extended to include private clinics and hospitals within the country. A natural next step to training program rollout is triage process implementation. KHMHA intends to incorporate the ETAT pediatric-specific criteria into their already existing ESI-based triage system, a hybrid design that has not been previously described. ETAT introduces the concepts of Emergency and Priority signs as easily identifiable pediatric signs and symptoms that signal a child needs either immediate or urgent care. These signs and symptoms can correspond to an ESI triage level 1 (requires life-saving intervention) for Emergency signs or an ESI level 2 (high risk for decompensation) for Priority signs. Once piloted, there is interest by the MoH in standardizing a national pediatric triage system based on this KHMHA hybrid triage process that we anticipate will improve timely emergency care for children throughout the country.
Conclusion
Participants feel that triage education and implementation is essential to improve communication and pediatric emergency care and agree that a national pediatric triage system would be beneficial. Prior to triage implementation all staff should be educated in the new process. When choosing which system to use a simple, low-resource pediatric-specific system, like ETAT, may improve utilization by staff, providing faster recognition of and improved care for acutely ill children. These beliefs should be considered when addressing triage implementation in RLS.
Footnotes
Acknowledgements
We would like to thank our partners at KHMHA for their support of this work, especially Drs Adrian Coye, Marta Habet, and Cecilio Eck and nurses Casilda Bowman and Marilyn Aspinall-Dawson.
Author Contributions
AEG: Contributed to conception and design; contributed to acquisition; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
EMS: Contributed to design; contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JMM: Contributed to conception and design; contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
LJ: Contributed to interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
HLC: Contributed to conception and design; contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Authors’ Note
This work has previously been presented as a poster presentation at both the American Academy of Pediatrics National Conference and Exhibition (Chicago, IL, on September 17, 2017) and the Consortium of Universities for Global Health Annual Conference (New York, NY, on March 16, 2018).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.