
Abstract
The present study characterized the plasma glycemic and lipid profiles in full-term newborn babies at birth and correlated these variables with growth markers and maternal clinical and metabolic conditions, to observe if maternal pregnancy conditions can influence metabolic programming in these newborn babies. Anthropometric and biochemical data were collected from 162 mother/newborn binomials at birth and at 6 months at a public hospital in Western Paraná State, Brazil. Samples of blood tests for glucose, insulin, total cholesterol, and triglycerides were obtained. Two classes of mothers/babies were statistically defined. The glycemic profiles in Class 1, at birth, were 63.0 ± 19.6 mg/dL and at 6 months 80.4 ± 10.6 mg/dL; in Class 2, at birth, they were 66.1 ± 20.8 mg/dL and at 6 months 78.2 ± 9.4 mg/dL. The triglycerides levels in Class 1 and Class 2, at birth, were 124.5 ± 47.8 mg/dL and 132.6 ± 60.2 mg/dL, respectively, and at 6 months they were 139.0 ± 51.5 mg/dL and 115.2 ± 39.9 mg/dL, respectively. Even though most of the pregnant women were overweight at the end of the gestation period, the anthropometric patterns found for babies followed the desirable standards. Furthermore, the average glycemic profile values were between the cutoff standards at birth and at 6 months; however, the triglycerides were above the expected values.
Introduction
Scientific evidences from epidemiologic, clinical, and experimental studies indicate that pregnancy events have a powerful influence in later susceptibility to certain chronic diseases, such as diabetes, hypertension, and cardiometabolic disorders. 1 Meanwhile, there is a lack of information about the glycemic and lipid profiles as related to the growth and development parameters in the scientific community. However, the patterns of full-term newborn babies’ (≥37 completed weeks of gestation) growth and development, including weight, height, and gestational age, are well defined in the literature. 2
Studies in recent decades have shown that the gestational period and the first years of life are critical times of development. In this context, nutritional or hormonal changes that modulate these critical periods affect an individual’s metabolism and predispose the individual to the onset of diseases in adult life, a phenomenon known as metabolic programming. 3
The intrauterine environment is fundamental for optimal fetal growth and development. A suboptimal intrauterine process may interfere in the fetus developmental pathway affecting health status later in life, as well as metabolic and cardiovascular disorders in childhood and in later adulthood. In premature babies, studies have presented relations between gestational conditions and development of diseases in the future, due to fetal programing. However, these relations are not clearly defined to full-term newborn babies. 1
In this article, we have studied maternal clinical and metabolic conditions using the same indicators in full-term newborn babies at birth and at 6 months of life. The parameters analyzed in order to evaluate metabolic conditions were glycemia (glucose and insulin) and lipids (total cholesterol [TC] and triglycerides [TG]). Alterations in these parameters, regardless of their association with obesity and arterial hypertension, may contribute to disease initiation, especially type 2 diabetes mellitus and cardiovascular diseases, which perhaps develop into metabolic syndrome. 4
Metabolic syndrome has received prominence in the scientific context, especially because of its increasing prevalence worldwide in adults and adolescents, but primarily in populations of children. 5 However, there is a lack of information about childhood and full-term newborn babies. 6 In Brazil, few published scientific studies about this syndrome demonstrate the prevalence of this disorder. 7 When these studies are performed in newborn babies, they are generally realized in premature babies with a focus on growth assessment. 8
The early identification of clinical or metabolic conditions that may be associated with health problems throughout life enables preventive treatment, guidelines, and changes in lifestyle related to eating habits and physical activities. Consequently, more aggressive procedures, such as pharmacological and surgical treatments, might be minimized in the future.
Based on this context, the objective of this study was to characterize the plasma glycemic and lipid profiles in full-term newborn babies at birth and at 6 months, correlated with growth markers and maternal clinical and metabolic conditions. The addition of the glycemic and lipid profiles as an evaluation method of the health level for full-term newborn babies to the already existing growth markers may be applied as reference parameters for this group.
Materials and Methods
This research was performed in an observational, cross-sectional study, with grants supported by the government (MCTI/CNPQ/Universal 14/2014). The inves-tigation was carried out in a maternity unit of a public hospital in the Western Paraná State. The following inclusion criteria were established: pregnant women without comorbidities, full gestational term, and living in the city where the study was conducted. Infants with no comorbidities and who were born at full-term were also included. In order to be a part of the research, both women and babies had to fulfill the requirement of having blood samples collected for routine biochemical examinations at the institution.
Thus, 2 groups were excluded from the research: pregnant women, who were younger than 18 years old, due to the Brazilian law that makes it necessary for parents to authorize participation for minors in a research; and full-term newborn babies undergoing umbilical cord blood collections, which may still present remains from their mothers’ blood. There were also losses due to insufficient sample volume and expiration of the laboratory methodology deadline.
Maternal variables, such as sociodemographic, anthropometric, prenatal, and delivery, were complemented by the full-term newborn babies’ anthropometric variables and integrated in the study. In addition, the glucose, insulin, TC, and TG test results, for both mothers and babies, were considered as variables in the study.
The data were collected using several approaches: an instrument designed for the research; the unit registration books, hospital records, and prenatal portfolio; and, when necessary, interviews with mothers after birth. Blood samples were collected, independently of the study, under routine unit examinations, such as examinations of bilirubin and serologies, during hospitalization. The blood collection procedures followed standard protocols defined by the hospital; then the laboratory technicians collected the samples with the amount established by their guidelines. Therefore, the residual/disposable sample was used to measure the biochemical and hormonal parameters for this investigation, within 24 hours of the blood sample being collected.
These measurements were performed in serum, and the blood components were separated to assess blood glucose and perform TC and TG tests, which were conducted in the clinical laboratory of the institution, following their guidelines. The results of glucose, TC, and TG were given in mg/dL and measured using the dry chemical method in an automatic analyzer (Vitros 4600 Chemical Systems and the Vitros 5600 Integrated System; Ortho Clinical Diagnostics, Raritan, NJ). Insulin was measured using an electrochemiluminescence method (UniCelDxI 800; Beckman Coulter, Brea, CA), following the methodology of the laboratory. The data were presented in µUI/mL, and the sensitivity level of the method was 0.03 IU/mL.
The Brazilian Society of Cardiology provides standard health index values for children between 2 and 19 years old and considers desirable values for TC as <150 mg/dL, borderline between 150 and 169 mg/dL, and increased as ≥170 mg/dL. For individuals aged <10 years old, the desirable values for TG are <100 mg/dL and increased >100 mg/dL. 9
The Brazilian Consensus for the Normalization of the Laboratory Determination of the Lipid Profile proposed new reference values for adult and pediatric subjects, taking fasting prior to blood collection into account. The desirable TC level in children aged 0 to 9 years is <170 mg/dL, independently of fasting. The expected TG level with fasting is <75 mg/dL and without fasting it is <85 mg/dL. 10
Similarities among the mothers were measured using agglomerative hierarchical cluster analysis, the Ward agglomeration method, and the Euclidean distance. Two classes (C1 and C2) were statistically defined according to the similarities among the mothers. Both C1 (n = 102) and C2 (n = 38) exhibited similarities and differences in age, height, body mass index (BMI), gestational duration, time of study, cohabitants, and the type of delivery performed.
After defining the clusters, the maternal qualitative variables were compared between the classes using the χ2 test for independence, followed by the adjusted residual test in cases of statistical significance. The quantitative variables were previously evaluated for data distribution patterns using the Shapiro-Wilk test, and the homogeneity of the variances was examined using the Levene test. Normality and homoscedasticity assumptions were satisfactory, and the variables were compared using the single-factor variance analysis, followed by the significance level test of .05. The tests were performed in the XLStat program, version 2015. All ethical regulations were followed, and the Research Ethics Committee approved the project under analysis number 1 228 229.
The sample, calculated by the Gpower program 3.1.9.2, considered 162 binomial mother/newborn babies at birth. The program predicted 0.95 power of analysis, 0.10 size of effect, and 0.05 error type 1. Sixty-nine babies returned at 6 months old for the follow-up stage. A new authorization was obtained from parents for blood sample collection. The data were collected from November 2015 to December 2016.
Results
The following means and standard deviations were found for the 162 newborn babies: 3.212 ± 438.6 g birth weight; 48.3 ± 2.1 cm height; and 33.7 ± 1.5 cm head circumference. The variations in the Z scores for weight/age (Z W/A), height/age, and cephalic perimeter/age were −0.2 ± 0.9, −0.7 ± 0.9, and −0.4 ± 1.0, respectively. Therefore, the mean value of the thoracic perimeter was 32.9 ± 2.0 cm, and the abdominal perimeter was 31.4 ± 2.2 cm (Table 1).
Anthropometric Profiles of Newborns at Birth (Cascavel, Paraná, Brazil, 2017) a .
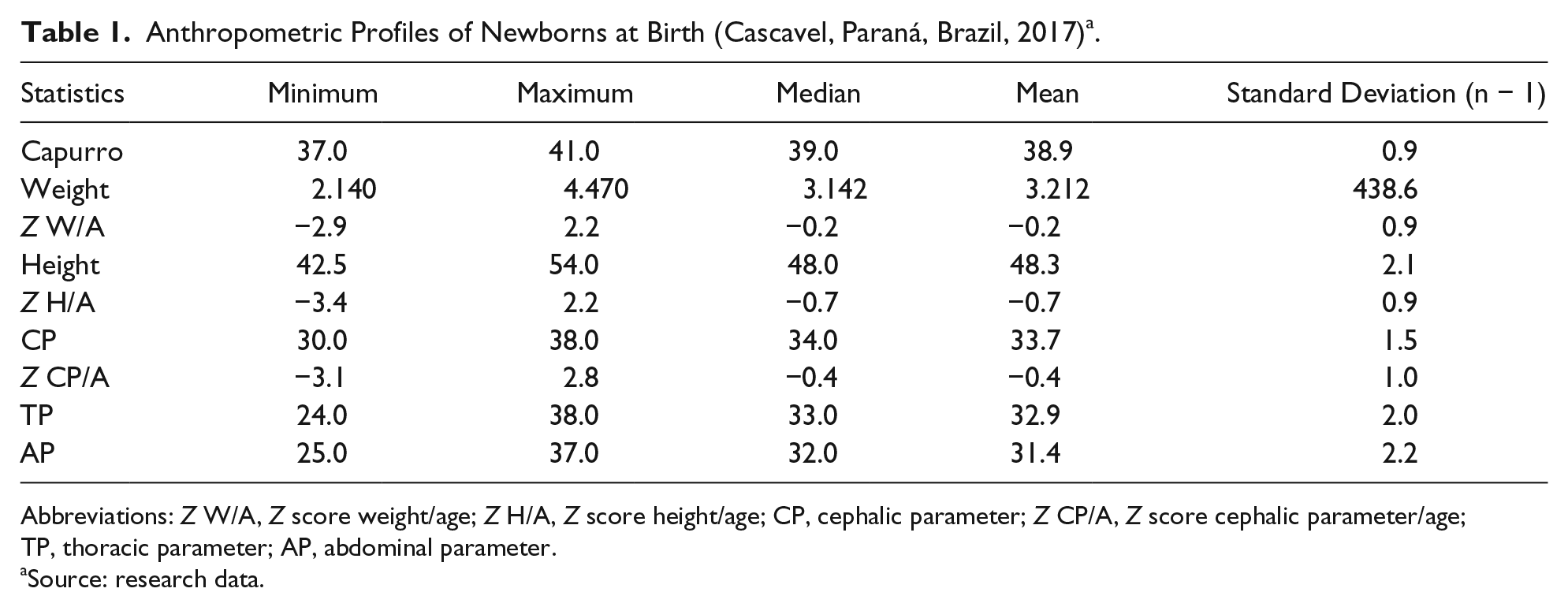
Abbreviations: Z W/A, Z score weight/age; Z H/A, Z score height/age; CP, cephalic parameter; Z CP/A, Z score cephalic parameter/age; TP, thoracic parameter; AP, abdominal parameter.
Source: research data.
In the full-term newborn babies’ sample, 50.6% of them were female and 49.4% were male. For weight, 84.6% of the full-term newborn babies were adequate for gestational age, 8.6% were small for gestational age, and 6.9% were large for gestational age.
Tables 2 and 3 present the characteristics of the mothers classified in the 2 classes (C1 and C2) according to their similarities.
Grouping of Classes Based on the Similarity of Maternal Sociodemographic, Prenatal, and Puerperal Data (Cascavel, Paraná, Brazil, 2017) a .

Abbreviations: NB, normal birth; NBE, normal birth with episiotomy; NBL, normal birth with laceration.
Note. Numbers in bold indicate statistics significance diference.
Source: research data.
Grouping of Classes According to the Similarity of Maternal Data, Age, Family Income, and Anthropometric Data (Cascavel, Paraná, Brazil, 2017) a .

Abbreviations: SD, standard deviation; BMI, body mass index.
Note. Numbers in bold indicate statistics significance diference.
Source: research data.
The present study observed the following variables: study time, cohabitants, type of labor (set out in Table 2), age, height, and BMI (presented in Table 3). These variables showed statistically significant differences between the classes of mothers (P < .05).
Data analysis demonstrated that the Class 1 mothers, composed of 102 women, exhibited a mean age of 25.2 ± 3.9 years, mean height of 161.6 ± 5.9 cm, and a previous BMI of 24.7 ± 4.4 kg/m2. School attendance was >8 years in 73.5%. Mothers who lived with people other than the father of the full-term newborn baby totaled 23.5%, and there was an expressive number of normal deliveries with episiotomy (28.4%).
Class 2 mothers, composed of 38 women, exhibited a mean age of 36.3 ± 3.7 years, a mean height of 158.7 ± 6.2 cm, and a previous BMI of 26.9 ± 5.7 kg/m2. School attendance was between 3 and 4 years in this group of mothers (10.5%), and most women lived with the full-term newborn babies’ father (94.7%). Normal delivery with laceration (21.1%) was more frequent if compared with Class 1 mothers.
Characteristic assessments of the full-term newborn babies at birth were also performed according to the mothers’ class (Table 4). Despite the differences between the 2 classes of mothers, there were no significant differences regarding their babies in the measurements of glucose, insulin, TC, TG, or any anthropometric variables. The only exception was the Z W/A of the full-term newborn babies at birth: a significantly higher index (−0.37 ± 1.0) was found for the babies born from Class 1 mothers, when compared with the babies born from Class 2 mothers (0.07 ± 0.8; P = .006).
Anthropometric Data of Babies at Follow-up, From Birth and at 6 Months, According to the Mothers’ Classes (Cascavel, Paraná, Brazil, 2017).*

Abbreviations: SD, standard deviation; CP, cephalic parameter; TP, thoracic parameter; AP, abdominal parameter; Z W/A, Z score weight/age; Z H/A, Z score height/age; Z CP/A, Z score cephalic parameter/age; TC, total cholesterol; TG, triglycerides.
Note. Numbers in bold indicate statistics significance diference. Mean and SD with equal letters are not different among each other. Different letters show different results (from the expected) in a column or line.
Source: Research data.
Characteristic evaluations of the full-term newborn babies were also tabulated according to the class of mothers, and the evolution of the variables, when at birth and at 6 months of life, was analyzed (Table 4).
In this study, none of the full-term newborn variables exhibited significant differences between the classes of mothers at 6 months. The growth patterns of the 2 groups were similar throughout the evaluated period for all anthropometric parameters. However, the Z score for W/A exhibited an increase in value at 6 months in Class 1, and there was a decrease in the development pattern in Class 2 children (P < .05).
Discussion
The parameters of lipid and glycemic profiles in full-term newborn babies on scientific literature is scarce. Thus, we have tried to standardize their values from our study under comparison with other stages later in life. For TC, we found at birth 84.8 mg/dL and at 6 months 143.4 mg/dL, in Class 1 mothers, and 89.6 mg/dL at birth and 140.0 mg/dL at 6 months in Class 2 mothers, 2 very similar patterns, according to the desirable values for TC (<150 mg/dL) in the 2 to 19 years old group.
For TG, at birth, our study found 124.5 mg/dL in Class 1 mothers, and 132.6 mg/dL in Class 2 mothers, meanwhile at 6 months, in Class 1 mothers, the mean was 139.0 mg/dL, and in Class 2 mothers it was 115.2 mg/dL, above the desirable values for TG, <100 mg/dL for individuals aged <10 years old.
The full-term newborn babies’ TC was compatible with desirable values, independently of the selected class, in comparison to the Brazilian Society of Cardiology reference values in its 2005 Guidelines. Regarding the Brazilian Consensus, the TC values were compatible with desired levels, in contrast to TG, which was above desirable values.
Related to the glycemic profile, our results shown at birth, for Class 1 mothers, 63.0 mg/dL, and for Class 2 mothers, 67.1 mg/dL. At 6 months, in Class 1 mothers, 80.4mg/dL, and for Class 2 mothers, 78.2mg/dL. All results correspond to the expected TG level with fasting, which is <75 mg/dL, and without fasting it is <85 mg/dL.
The average glycemic profile values in this study were between the cutoff standards of 45 and 145 mg/dL independent of the class, as established by the Ministry of Health. 11 Furthermore, these values were similar to Amorim’s 12 study and above the cutoff values for hypoglycemia reported by the Committee on Fetus and Newborn and Adamkin. 13 The glycemic profile in Class 1 was 62.5 ± 15.5 mg/dL, and that in Class 2 was 66.7 ± 18.6 mg/dL, which are according to the expected parameters.
The lipid profile of full-term newborn babies at 6 months found in this research was lower than the TC and close to the TG values from Harit’s 14 research. Regarding the Brazilian Society of Cardiology Guidelines, 9 the TC values were considered desirable (<150 mg/dL), and the TG values were above the desirable level in Class 1 and considered to be borderline in Class 2. In relation to the Brazilian Consensus for the Normalization of the Laboratory Determination of the Lipid Profile, 10 the TC values were desirable for both classes, and the TG values were above the desired level, independently of the classes. Regarding the glycemic profile, the average values of the classes remained within the cutoff standards stipulated by the Ministry of Health. 11
In addition, maternal anthropometric data in this study showed a weight gain above the Ministry of Health recommendation. 15 Using the Atalah Curve 11 as a reference for evaluation, the mean BMI of these pregnant women was adequate when at the beginning of their pregnancy, but they were overweight at the end of gestation. In comparison, a study of 712 pregnant women found an initial BMI of 24.05 ± 4.74 kg/m2, a final gestational weight of 75.84 ± 13.86 kg, and a weight gain during pregnancy of 13.20 ± 5.51 kg, which are very similar to the values in our research. 16
The variations in the Z score of all anthropometric measurements in our results were consistent with the World Health Organization 17 for growth assessment in this age group. Similarly to our study, Amorim 12 found that the mean values were 48.9 ± 2.3 cm for height and 33.9 ± 1.7 cm for head circumference.
The anthropometric patterns were coincident to previous studies,12,16 but the lipid profile of the full-term newborn babies at birth were higher than others, such as Amorim, 12 Sales et al, 18 Aletayeb et al, 19 and Murthy et al, 20 for TC or TG values.
The Z score growth ranges at 6 months were in compliance with the guidelines of the World Health Organization. 17 The negative correlation found between the Z score W/A can be determined by the characteristics of the classes of mothers. In Class 1, mothers had a higher schooling level and were younger than Class 2. This condition may show greater knowledge and a higher health literacy level for feeding care with babies, which favors a greater weight gain for the full-term newborn babies in Class 1.
In a cohort study by Lin et al 3 to assesses the impact of prenatal environment and genetic and epigenetic factors on birth weight and size/adiposity in early childhood, 11 of 30 prenatal environments, including maternal adiposity, smoking, blood glucose, and plasma unsaturated fatty acid levels, were associated with birth weight. Individual prenatal environmental influences on birth weight were also identified, as maternal BMI, gestational weight gain, and glucose levels, among other factors, were associated with offspring size and adiposity in early childhood. These findings were consistent with our results, despite the distinct correlations.
The differences between our studied variables were not significant, which may be related to the number of subjects, which is one of the limitations of this study. Another one is related to the study design, primarily performed to obtain few environment measures and follow-up the full-term newborn until 6 months only. However, this research showed relevant data regarding the glycemic and lipid profiles of full-term infants. We recommend the continuation of this study with a larger number of samples and evaluations of dietary associations on the glycemic and lipid profiles during the follow-up.
Determining a definitive parameter for the glycemic profile of full-term newborn babies remains a challenge because blood collection is an invasive procedure and birth characteristics are extremely particular to each individual. This fact, added to variables that involve the gestational period and the conditions at birth and growth, among other factors, make standardization difficult. However, our data provide future evaluations of full-term newborn babies, considering the glycemic and lipid parameters, in order to avoid complications in adult life.
Footnotes
Acknowledgements
The authors thank the National Research Council, the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), for the support offered from the Biosciences and Health Master’s at Western Paraná State University.
Authors’ Note
Author Contributions
Hugo Razini Oliveira, Beatriz Rosana Gonçalves de Oliveira Toso, Ana Teresa Bittencourt Guimarães, Cláudia Silveira Viera, Sabrina Grassioli: participate in the conception, design, analysis and interpretation of the data; writing of the manuscript and its revision, and in final approval of the version to be published. Bruna Juliana Zancaro Frizon, Graziella Massoti Scalabrin Barreto, Julia Reis conterno and kamila Caroline Minosso participate in the design, analysis and interpretation of the data and in final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Council, the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).