
Abstract
Objective
The CYP2C19 genetic variation may be involved in the development of atherosclerotic cardiovascular disease (ASCVD). Serum lipid levels are important risk factors for ASCVD, but the effect of the CYP2C19 gene on serum lipid metabolism remains unclear. This retrospective cohort study investigated the relationship between the CYP2C19 gene polymorphism and serum lipid levels in patients with ischemic stroke (IS).
Methods
IS patients (n = 230) and control subjects (n = 100) were enrolled. All patients were diagnosed with IS via clinical manifestations and brain magnetic resonance imaging. All patients were genotyped.
Results
Triglyceride (TG), total cholesterol (TC), low-density lipoprotein-cholesterol (LDL-c), and apolipoprotein B (ApoB) levels were significantly higher and high-density lipoprotein-cholesterol (HDL-c) and apolipoprotein A1 (ApoA1) levels were significantly lower in the IS group compared with the control group. Lower ApoA1 levels and higher ApoB levels were significant predictive factors for IS. Patients with higher ApoB levels had a higher risk of IS recurrence. Compared with extensive metabolizers, intermediate and poor CYP2C19 metabolizers had a higher risk of IS recurrence.
Conclusions
Our study indicates CYP2C19 gene polymorphisms are related to lipid metabolism in patients with IS. IS patients who are poor CYP2C19 metabolizers may have a higher risk of disease recurrence.
Keywords
Introduction
Ischemic stroke (IS) is caused by a focal occlusion or stenosis of one or multiple arteries within and leading to the brain, including intracranial occlusion and extracranial cervical artery occlusion, which accounts for about 85% of stroke. 1 Stroke has a high morbidity and disability rate; it is the second leading cause of death worldwide, and accounts for >2 million deaths annually in China.2,3 Based on relevant reports, the total global burden of stroke is increasing, and prevention is essential for stroke management.4–6 Risk factors for IS include smoking, hypertension, diabetes, and elevated cholesterol. 7 Among them, the serum lipid level is an important risk factor for IS, and it is positively correlated with disease prognosis. Authoritative research shows that lowering lipoprotein levels can still bring net benefits to China’s overall stroke and cardiovascular disease.7–10
Cytochrome P450 (CYP450) is a superfamily of genes that play an important role in the metabolism of endogenous and exogenous substances in a wide range of organisms. The largest P450 family in mammals is the CYP2 gene family. Among them, CYP2C8, CYP2C9, CYP2C18, and CYP2C19 metabolize more than half of the commonly used prescription drugs, arachidonic acid, and some steroids. 11 CYP2C9 and CYP2C19 have long been considered to be important drug metabolism genes, but emerging studies have shown that CYP2C9 and CYP2C19 gene polymorphisms may be associated with the occurrence and recurrence of cerebral ischemic stroke.12,13 Another group of scholars found that CYP2C9 polymorphism gene may reduce the serum total triglyceride (TG) and low-density lipoprotein (LDL) levels in young adult epileptic patients and lower the risk of subclinical atherosclerosis. 12 However, there are few articles on the relationship between CYP2C19 gene polymorphisms and lipoproteins in IS patients. In this present study, we divided patients into different metabolic groups based on the status of different alleles to elucidate the relationship between CYP2C19 gene polymorphisms and serum lipid levels in patients with IS.
Patients and methods
Study patients
In this study, we randomly selected 230 patients (male, 158; female, 72) who were treated in the First Affiliated Hospital of Nanchang University from January 2018 to May 2019, and all patients were diagnosed with IS on the basis of clinical manifestations and diffusion-weighted brain magnetic resonance imaging. The inclusion criteria were as follows: (1) patients experienced new onset within 72 hours and had no medical history of antiplatelet, anticoagulant, and thrombolytic treatment in the previous 2 weeks; (2) patients were free of other serious illnesses such as infectious diseases, hemopathy, cancer, autoimmune diseases, severe cardiac, and renal and hepatic diseases; and (3) had no recent history of trauma or surgery.
We collected the patients’ demographic data and established risk factors for stroke, such as age, sex, hypertension, and diabetes. The results of alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum creatinine (SCr), blood urea nitrogen (BUN), blood glucose (GLU), TG, total cholesterol (TC), low-density lipoprotein cholesterol (LDL-c), high-density lipoprotein cholesterol (HDL-c), apolipoprotein A1 (ApoA1), and apolipoprotein B (ApoB) were collected using electronic medical records (EMRs). The above parameters are part of the results of the fasting blood collection test on day 2 after admission. As a control group, we also collected the same information from 100 individuals from the Physical Examination Center of First Affiliated Hospital of Nanchang University between January 2019 and May 2019. All the subjects in this study were ethnic Han.
Genetic testing
Blood samples (EDTA anti-coagulated; 2–3 mL) were taken from IS patients, and DNA was extracted from the blood on the same day. DNA was extracted using a fully automatic gene extractor (NP968-C, Suzhou, China). The concentration and purity of the samples were determined via nucleic acid detection analyzer (Quawell, San Jose, USA). CYP2C19 genotype was detected using real-time PCR. In accordance with the instructions, four kinds of reaction solutions were added to each sample. The internal reference probe was added to control the quality of the reaction. Each experiment was performed using a positive control and a blank control. The PCR reaction total system was 25 μL, of which 23 μL were from each of the reaction solutions, 1 μL of enzyme, and 1 μL of template. The entire fluorescent quantitative PCR reaction was performed on an ABI7500 instrument (Applied Biosystems, Foster City, CA, USA). The PCR reaction protocol consisted of a 2-minute hold at 37°C, a 3-minute hold at 95°C, followed by 10 cycles of 30 s at 95°C, 30 s at 56°C, and 45 s at 65°C. This was followed by 30 cycles of 30 s at 95°C, 30 s at 56°C, and 45 s at 65°C. Sample fluorescence results were recorded during the extension step of the last cycle. At the end of the program, the amplification curve was obtained, and the samples were analyzed using the Ct value. Genotype results were then interpreted.
Genotyping
Three single-nucleotide polymorphisms (SNPs) for CYP2C19 (National Center for Biotechnology Information [NCBI] Genome build 37.1, GenBank NG_008384), including CYP2C19*2 (681G>A, dbSNP rs4244285), CYP2C19*3 (636G>A, dbSNP rs4986893), were genotyped in 230 IS patients. Patients with at least two *2 or *3 alleles (*2/*2, *2/*3, or *3/*3) were classified as poor metabolizers (PM), those with one *2 or *3 allele (*1/*2 or *1/*3) were classified as intermediate metabolizers (IM), and those without a *2 or *3 (*1/*1) were classified as extensive metabolizers (EM).
Statistical analysis
Statistical analyses were performed using SPSS version 19.0 (IBM SPSS Statistics, IBM Corp., Armonk, NY, USA) and GraphPad Prism version 8.00 (GraphPad, La Jolla, CA, USA). The subjects’ baseline characteristics were compared between the IS patient group, the control group, and the three different groups of metabolomes. Proportions were used for categorical variables, and medians with interquartile ranges (IQRs) were used for continuous variables. A nonparametric Kruskal–Wallis test was used to compare group differences for nominal variables. Variables related to IS were analyzed using univariate and multivariate logistic regression. Cox regression analyses were performed to investigate if lipid levels were independently associated with the risk of IS recurrence. The Kaplan–Meier product limit method was used to estimate the cumulative recurrence-free rate of three genomes. Data were presented using hazard ratios and 95% confidence intervals. Differences in Kaplan–Meier curves were evaluated with the log-rank test. P values < 0.05 were considered to be significant.
Ethical standards
All studies described in this article were performed after obtaining approval of the ethics committee and institutional review board at the First Affiliated Hospital of Nanchang University. Studies were conducted in accordance with national law and the Declaration of Helsinki 1964 (and subsequent revisions). Informed consent was obtained from all participants in the study.
Results
Study patients
There were 230 IS patients with an IS diagnosis confirmed based on clinical manifestations and diffusion-weighted brain magnetic imaging who were enrolled into this study, including 158 men and 72 women. Additionally, 100 controls subjects were enrolled, including 67 men and 33 women.
Clinical characteristics of the IS and control groups
Baseline clinical characteristics of the IS and control groups are shown in Table 1. The proportions of patients with hypertension and diabetes was higher in the IS group compared with the control group (P < 0.001). TG, LDL-c, and ApoB levels were significantly higher in the IS group compared with the control group (P < 0.001 for all), while HDL-c and ApoA1 levels were significantly lower in the IS compared with the control group (P < 0.001 for both). There were no significant differences in the levels of ALT, AST, s-CR, BUN, and GLU.
Clinical characteristics of IS patients and controls.

Data were analyzed using the Kruskal–Wallis test. Data are presented as the median and IQR.
P < 0.05 was considered significant. Boldface indicates statistical significance.
IS, ischemic stroke; ALT, alanine aminotransferase; AST, aspartate aminotransferase; SCr, serum creatinine; BUN, blood urine nitrogen; GLU, blood glucose; TC, total cholesterol; TG, triglyceride; HDL-c, high-density lipoprotein cholesterol; LDL-c, low-density lipoprotein cholesterol; APOA1, apolipoprotein A1; ApoB, apolipoprotein B; N.S., not significant; IQR, interquartile range.
Logistic regression analysis of IS risk factors
Univariate logistic regression analysis was performed on all items, and compared with the control group, the IS group had significantly increased odds of having higher TC levels, higher ApoB levels, lower HDL-c levels, and lower ApoA1 levels (Table 2). Only factors with a P value < 0.05 in the univariate analysis were included in the multivariate regression analysis. As shown in Table 2, lower ApoA1 levels and higher ApoB levels were significant predictive factors in IS patients. ApoA1 was negatively correlated with the onset of IS (OR = 0.001, 95% CI: 0.000–0.011, P < 0.001), and ApoB levels were associated with a higher incidence of IS compared with TG, TC and LDL-c (OR = 72.753, 95% CI: 1.790–2957.475, P = 0.023).
Univariate and multivariate logistic regression analysis of factors predicting IS prevalence.

Data were analyzed using logistic regression analysis. P<0.05 was considered significant.
Boldface indicates statistical significance.
OR, odds ratio; CI, confidence interval; IS, ischemic stroke; ALT, alanine aminotransferase; AST, aspartate aminotransferase; SCr, serum creatinine; BUN, blood urine nitrogen; GLU, blood glucose; TC, total cholesterol; TG, triglyceride; HDL-c, high-density lipoprotein cholesterol; LDL-c, low-density lipoprotein cholesterol; APOA1, apolipoprotein A1; ApoB, apolipoprotein B; N.S., not significant.
Clinical characteristics in different IS patient metabolizer groups
There were 230 patients who were categorized as having a CYP2C19 metabolizer status based on *2 and*3 genotypes using the common consensus star allele nomenclature. 14 Patients with at least two *2 or *3 alleles (*2/*2, *2/*3, or *3/*3) were classified as PMs (n = 81, 35%), those with one *2 or *3 allele (*1/*2 or *1/*3) were classified as IMs (n = 70, 30%), and those without a *2, *3 allele (*1/*1) were classified as EMs (n = 79, 34%). Patient characteristics were similar between PM, IM, and EM groups, as shown in Table 3. There were significant differences in TC, LDL-c, and ApoB between the three groups of IS patients (P < 0.013, P < 0.013, P < 0.008, respectively), while there was no significant differences in the levels of ALT, AST, SCr, BUN, GLU, TG, HDL-c, and ApoA1. The pairwise comparison showed that the above three indicators were significantly different between the EM group and the PM group (P < 0.02; Table 3). There was no significant difference between the EM group and the IM group, and the EM group and the PM group, except for the above-mentioned indicators.
Clinical characteristics of the EM, IM, and PM groups.

Data were analyzed using the Kruskal–Wallis test.
P<0.05 was considered significant. Boldface indicates statistical significance.
*Compared with the EM group, P<0.02
EM, extensive metabolizers; IM, intermediate metabolizers; PM, poor metabolizers; ALT, alanine aminotransferase; AST, aspartate aminotransferase; SCr, serum creatinine; BUN, blood urine nitrogen; GLU, blood glucose; TC, total cholesterol; TG, triglyceride; HDL-c, high-density lipoprotein cholesterol; LDL-c, low-density lipoprotein cholesterol; APOA1, apolipoprotein A1; ApoB, apolipoprotein B; N.S., not significant.
Independent risk factors for IS recurrence
All the patients treated with clopidogrel (75 mg daily) were followed-up by phone every 3 months after discharge, with recurrence or death as the follow-up endpoint. As of 10 December 2019, there were 151 patients (66%) with follow-up data in this study, and 79 patients (34%) were lost to follow-up. Among them, nine patients (6%) died as a result of stroke and 17 patients (11%) had recurrence. Results of the univariate Cox analysis showed that ApoB was a risk factor for stroke recurrence (Figure 1). Further evaluation of the effect of different genotypes on disease recurrence revealed that PM and IM patients had a higher risk of stroke recurrence compared with EM patients (Figure 2).
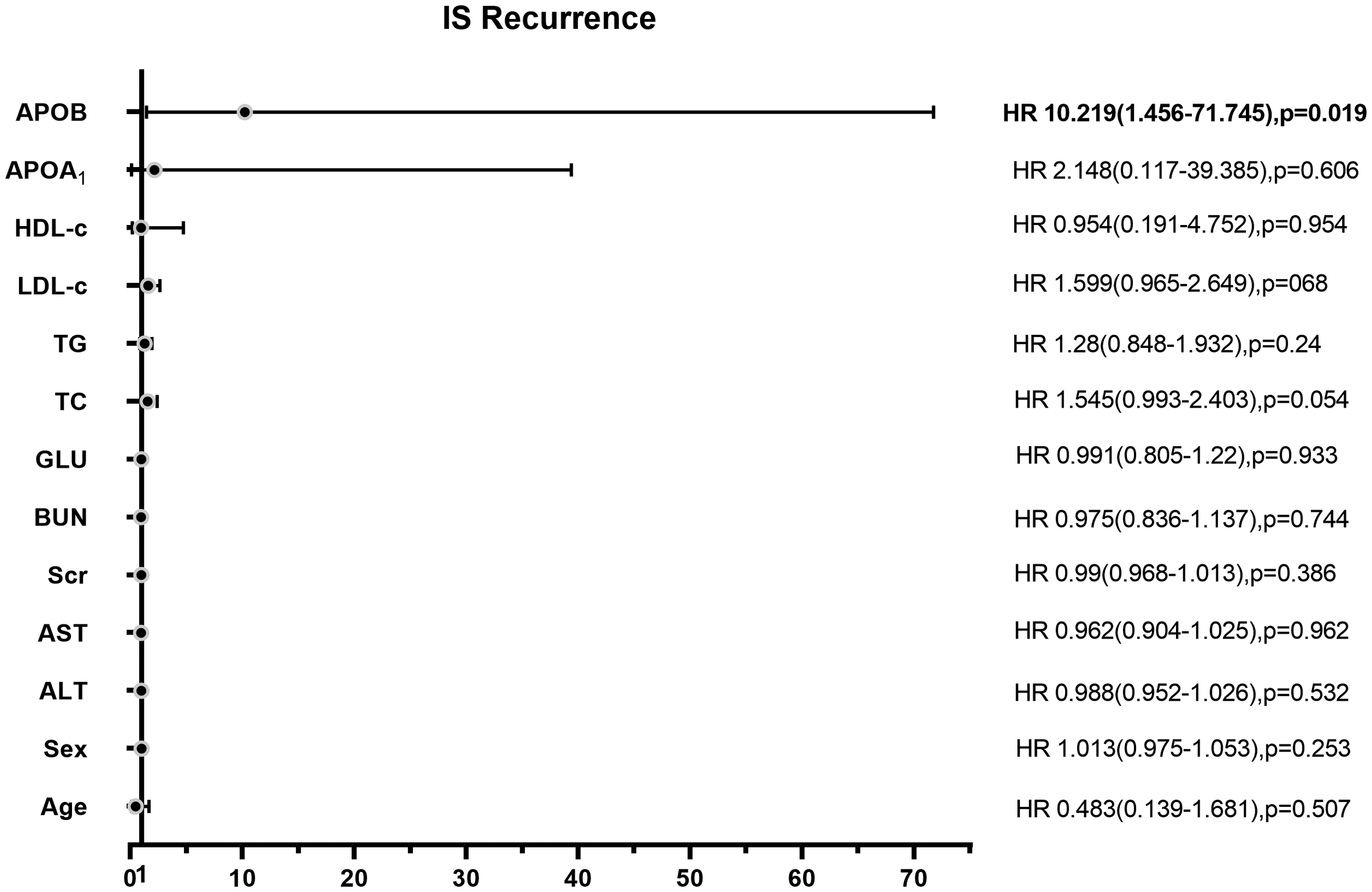
Cox regression analyses of the association between ALT, AST, Scr, BUN, TG, TC, LDL-c, HDL-c, APOA1, ApoB, and IS recurrence. Associations are presented as hazard ratios and 95% confidence intervals.

Cumulative recurrence-free rates of extensive metabolizers, intermediate metabolizers, and poor metabolizers and calculation of the risk of recurrence.
Discussion
The CYP2C19 gene contains nine exons and eight introns, which are located within the cytochrome P450 gene cluster on chromosome 10q24. This gene encodes a 490-amino acid long protein of approximately 56 kDa, which is a major liver enzyme. To date, CYP2C19 has been widely studied as an important drug metabolism gene, which plays an important role in the metabolism of the anticonvulsant drugs mefenidine, omeprazole, diazepam, and some barbiturates.13,15 CYP2C19*2 and CYP2C19*3 are the two most common mutations, resulting in the inactivation of transcriptional splice mutations and the formation of terminators, which disrupt the activity of transcriptional proteins. Both of these mutations can lead to a loss of metabolic function.16,17 Recently, emerging studies have revealed the important role of CYP2C19 gene polymorphism in several diseases including IS and subclinical atherosclerosis.18,19 Gu et al. 13 considered that the AA genotype and A allele of CYP2C19 G681A may be related to the occurrence and recurrence of cerebral ischemic stroke. Salagacka-Kubiak et al. 18 suggested there is some interaction between gender, CYP2C19*2 polymorphism, and pathogenesis of Helicobacter pylori infection development. However, the conclusions are inconsistent. For example, Lee et al. 20 believed that CYP2C19 PMs are not associated with IS and its subtypes. However, few studies have further linked the CYP2C19 gene polymorphism to endogenous substance metabolism. To the best of our knowledge, this is the first study to investigate the effect of CYP2C19 polymorphism on the lipid profile in IS patients. Because serum lipids are important risk factors for the onset of IS, 7 we sought to explain the effect of CYP2C19 gene polymorphism on the incidence of IS by studying the lipid levels in different metabolomes.
Epidemiological studies have revealed that the numerous risk factors for atherosclerosis include environmental factors and genetic components, such as hypertension, diabetes, and hyperlipidemia. Increased blood pressure variability increases the stress on blood vessels and leads to endothelial dysfunction, thereby promoting early target organ damage. Similarly, variability in fasting blood glucose (FBG) is associated with future cardiovascular events. 21 The 2019 America College of Cardiology/American Heart Association (ACC/AHA) guidelines for Primary Prevention of Cardiovascular Disease 22 state that type 2 diabetes mellitus and hypertension are important risk factors for atherosclerotic cardiovascular disease (ASCVD). In the United States, the number of ASCVD deaths caused by hypertension exceeds any other variable ASCVD risk factors. 23 In another meta-analysis of prospective studies, 24 a log-linear association was observed between systolic blood pressure (SBP) levels <115 to >180 mmHg and diastolic blood pressure (DBP) levels <75 to 105 mmHg and the risk of ASCVD. The analysis shows that each SBP increase of 20 mmHg and each DBP increase of 10 mmHg may double the risk of death from stroke, heart disease, or other vascular disease. Our study analyzed the prevalence of diabetes and hypertension in patients with IS and healthy controls. It has become clear that screening and treatment of hypertension and diabetes are important and effective in stroke prevention. 7
Serum lipid levels are reportedly associated with the risk of IS; however, it remains controversial whether individual levels of blood lipids can be used as independent risk factors for IS. 25 Lipid metabolism can affect the progression of arteriosclerosis. ApoB-lipoprotein accumulates subendothelially and initiates a sterile inflammatory response involving all classes of innate and adaptive immune cells that have a response that is dominated by monocyte–macrophages. These inflammatory cells, together with proliferating smooth muscle cells and extracellular matrix, promote subendothelial injury or plaque formation that initiates atherosclerosis. These cellular events lead to the formation of the very small minority of plaques that account for acute atherothrombotic vascular events, including unstable angina, myocardial infarction, sudden cardiac death, and IS. 26 Based on other reports, in addition to the common factors such as LDL-c and HDL-c, ApoB and ApoA1 may be better indicators of the risk of cardiovascular and cerebrovascular diseases compared with conventional risk factors.27,28 A meta-analysis 29 also indicated that ApoB is a more accurate marker of cardiovascular risk compared with LDL-c. Through screening by univariate and multivariate logistic regression, our study showed that ApoB levels are associated with a higher incidence of IS compared with TG, TC, and LDL-c, and that ApoA1 is negatively correlated with the onset of IS. Our results are similar to previous research. However, whether it is an independent risk factor for IS onset requires an additional study with a larger sample size.
Studies have consistently shown that high TC levels and LDL-c levels are associated with an increased risk of ASCVD, and high HDL-c levels are associated with a reduced the risk of ASCVD.21,22,29–31 LDL-c, TC, HDL-c, and TG are all transferred genetically. Analysis of lipid metabolism levels via molecular and genetic pathways will provide new therapies and preventive measures for ASCVD.31,32 Hindy et al. 31 analyzed 188,578 individuals using genome-wide and custom genotyping arrays, and they identified 157 loci that were associated with lipid levels, including multiple CYP genes. The study indicated that loci that were associated with blood lipid levels were associated with cardiovascular and metabolic characteristics such as blood pressure and body mass index. CYP450, lipoxygenase, and cyclooxygenase are the main catalytic enzymes that are involved in blood lipid metabolism. The polyunsaturated fatty acids (PUFAs) that are produced by these three enzymes are endogenous lipid signaling molecules. 33 The PUFA products of CYP450 mainly include epoxy fatty acids and arachidonic acid, both of which are involved in biological regulation as important lipid signaling molecules.11,34 Epoxyeicosatrienoic acid (EET) is a vasoactive substance that is produced by the CYP2C gene subfamily, and it catalyzes the production of arachidonic acid. It is mainly stored in vascular endothelial cells and participates in biological metabolism through esterification to phospholipids.35–37 EET can affect vascular tone and change blood pressure, and it has a role in promoting fibrinolysis. 38 Studies have shown that soluble epoxide hydrolase (sEH), a downstream enzyme that is involved in the CYP monooxygenase eicosanoid pathway, and its metabolic products (fatty acid diols) are overexpressed in the colon of obese mice. The roles of the CYP/sEH pathway may provide new treatment ideas for a variety of metabolic diseases. 38
The CYP2C19 and CYP2C9 genes are currently the most widely used CYP genes in ASCVD patients, and they are commonly used as metabolic enzymes for clopidogrel and warfarin. Polymorphisms in both genes are often associated with disease progression and poor prognosis. CYP2C9 is the main catalytic enzyme of EET, and its polymorphisms are closely related to the activity of EET derivatives. 39 Previous studies found that CYP2C9 gene polymorphisms are associated with serum TC and LDL-c levels in young adult patients with epilepsy. 12 In humans, the CYP2C19 gene expression level is about 10% of the CYP2C9 gene, but these two genes have 91.2% sequence uniformity. 40 Recently, studies have found that EETs and CYP2C19 were upregulated in triple-negative breast cancer (TNBC) tumors, which correspond to the fatty acid binding proteins, adipocyte signaling, and metastasis-related processes, which preliminarily confirmed the role of CYP2C19 gene’s endogenous metabolic regulation. 41 CYP2C19 *2 and *3 alleles are the most common mutation sites in CYP2C19, and they can cause transcriptional inactivation and may lead to abnormal metabolic function by destroying the activity of the transcribed protein. 17 By comparing the differences in the indices of the three different metabolomes, our study found significant differences in TC, LDL-C, and ApoB. Further comparison between the two groups showed that a difference between the above three indicators mainly exists between the EM and PM groups. Our results suggest that IS patients with poorly metabolizing CYP2C19 genotype have higher serum lipid levels, which are mainly manifested as an increase in TC, LDL-C, and ApoB levels. We conclude that CYP2C19 gene polymorphisms may affect the lipid metabolism in patients with IS.
As mentioned above, ApoB has become an important indicator for predicting the incidence of IS, and most current studies focus on the prediction risk for acute IS.26–29 Our article further analyzes the follow-up data from stroke survivors who were treated with clopidogrel. Compared with other blood lipid variables, ApoB has a certain significance in predicting IS recurrence. A high ApoB levels may have a higher risk of disease recurrence. In addition, we performed several analyses of different metabolizers of the CYP2C19 gene polymorphisms, which yielded similar results, and thus, strengthened our conclusion that PMs are independently associated with the risk of IS recurrence. We suggest that IS patients with at least two *2 or *3 alleles may have a higher risk of stroke compared with the EMs with the CYP2C19 genotype in stroke survivors who were treated with clopidogrel. Because most of the patients in this study had acute IS, which is often accompanied by severe symptoms such as loss of consciousness and hemiplegia, patients’ follow-up data collection was difficult, and several patients’ disease progression could not be tracked. Furthermore, this study had a small sample size, which requires more research and follow-up data to confirm and validate our findings.
Conclusion
CYP2C19 gene polymorphisms may be related to lipid metabolism in patients with IS. We suspect that IS patients who are poor CYP2C19 metabolizers may have a higher risk of disease recurrence. Because our study has a limited sample size, further studies in a large population are needed to confirm these findings.
Footnotes
Author contributions
Rui Zhao designed the study and revised the paper. Yun-xue Bai wrote the majority of the paper, tested the samples, and was responsible for the statistical analysis. Ruicheng Huang and Lagen Wan collected the clinical data from the subjects and provided help with the statistical analysis.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
All studies described in this article were performed after obtaining approval of the ethics committee and institutional review board at the First Affiliated Hospital of Nanchang University. Studies were conducted in accordance with national law and the Declaration of Helsinki 1964 (and subsequent revisions). Informed consent was obtained from all participants in the study.
Funding
This study was supported by a project supported by Natural Science Foundation of Jiangxi Province, China (Grant No. 20192 BAB205088).