
Abstract
Objective. To examine whether children’s early communication skills at age 3 predict special education outcomes at kindergarten entry. Methods. Data from 139 children eligible for early intervention or early childhood special education services were examined. Early communication was defined separately as expressive and receptive language skills and was measured by the Vineland Adaptive Behavior Scales–Second Edition. Outcome variables were parent-reported measures of special education use and dosage as well as speech therapy receipt and dosage at kindergarten entry. Results. Better expressive language skills at age 3—but not receptive language skills—predicted a significantly reduced likelihood (odds ratio = 0.79) of receiving speech therapy at kindergarten entry. There were no effects of early communication on broader receipt of special education services as well as on special education dosage. Conclusions. Screening of specific domains of early communication skills during routine pediatric care, in conjunction with the evaluations of other professionals involved in the child’s education and health, might be an effective method for identifying children who are likely to receive speech therapy and other special education services at kindergarten entry.
Introduction
Deficits in early communication skills are associated with poor developmental and educational outcomes.1,2 Communication skills relate to the ability to impart and understand meaning. Definitions of communication include social, symbolic, and speech understanding, 3 while definitions that focus on language distinguish between expressive and receptive language. 4 While speech and language deficits are linked to neurodevelopmental conditions such as autism spectrum disorder (ASD),5-7 individual differences in early communication skills are also observed in other populations such as children with delayed language development.8-10 While speech and language development are useful indicators of overall development and cognitive ability, a long-standing debate remains regarding best practices in the screening of speech and language deficits and its application in primary care settings,11-15 despite the existence of and adherence to general recommendations for developmental surveillance and screening.16-18
Increasing attention has been devoted to examining the nature of the link between early communication deficits and special education outcomes in young children. 19 Early intervention and childhood special education reflects specialized services for children who are identified as having a deficit or delay in cognitive, physical, or social functioning that can often affect children’s development and learning. While special education is an important part of a child’s overall education, special education status can lead to children being labeled and stigmatized, even after children no longer require such services. 20 Through effective screening and early intervention, pediatric primary care can potentially reduce the need for costly special education services.
Children who receive special education services often experience comorbid conditions,21,22 suggesting that while children might receive specialized services due to a communication deficit, these children may have other difficulties and/or may be at risk for developing other learning-related disorders, underscoring the need to better understand whether and how early communication skills might be related to broader patterns of receipt of special education services. For example, while speech therapy might be the preferred solution for children identified as having communication difficulties, these same children might require and receive a variety of other services not directly related to speech and language. Accordingly, the present study examined the extent to which communication deficits in early childhood were associated with receiving a broad array of special education services in kindergarten, as well as the intensity (dosage) of these services.
In particular, deficits in early communication are often associated with a diagnosed global developmental delay, which is associated with greater behavioral problems and poorer school adjustment23,24 and may persist throughout schooling if left untreated. In middle childhood, nearly 1 in 5 children have more than one special health care need; these needs are significantly associated with poorer academic achievement and lower motivation to do well in school. 25 The common comorbidity associated with early communication deficits underscores the need to better understand the link between communication skills and the receipt of special education services in this population. Accordingly, the present study also extends previous work by examining the nature of this association in a community-based sample of children with developmental delay or at high risk of developmental delay.
In the present study, we examined whether individual differences in 2 key dimensions of early communication measured at age 3—receptive language (understanding speech) and expressive language (producing speech) 26 —predict special education use and dosage at kindergarten entry. Examining whether and how individual differences in communication skills relate to patterns of special education service utilization at kindergarten entry can enhance our understanding of the factors that predict a successful school transition. We had 2 predictions. First, we predicted that deficits in early communication would be associated with greater use of a broad array of special education services as well as increased dosage of these services. We left open the possibility that receptive or expressive language might be a stronger predictor than the other. Second, we hypothesized that early communication deficits would predict an increased likelihood of speech therapy receipt and dosage at kindergarten entry. Because deficits in early expressive language—but not receptive language—are associated with later language difficulties, 27 we predicted that weaker expressive language skills would predict greater use and dosage of speech therapy.
Method
Participants
One hundred eighty families and their children participated in a small-scale efficacy study examining the effects of a group-based parent training program to reduce behavior problems in children with developmental delay and improve positive parenting practices. Because intervention effects are not the focus of the current investigation, we controlled for treatment condition in all analyses.
Special education is not a one-size-fits-all model and varies considerably across the United States. In the state of Oregon, where the present study took place, any individual can refer a child to the Early Intervention/Early Childhood Special Education (EI/ECSE) program, which is administered by different county offices throughout the state. Each office coordinates a screening/evaluation of the child, results of which determine whether the child is eligible for EI/ECSE services. It is important to note that an affirmative determination of eligibility is not equivalent to a medical diagnosis by a primary care physician. Special education eligibility determination generally involves a multidisciplinary team of professionals, such as preschool teachers and autism specialists who can conduct an evaluation and determine eligibility for services. Children who were deemed eligible to receive EI/ECSE services were recruited for the study from community health and special education clinics. All children possessed an Individualized Family Service Plan (IFSP), which includes information on the services the child will receive that year, who will provide those services (eg, speech-language pathologist, physical therapist, and behavioral specialist), and a timeline for receiving those services. While similar in scope and function, an IFSP differs from an Individualized Education Program (IEP) in that an IFSP is provided for children who have not yet entered elementary school, and review of IFSPs take place every 6 months rather than the annual review process for IEPs.
Of the 180 families who initially participated in the study, full case data were available for 139 families and their children (34 girls, meanage = 36.9 months, SD = 4.6, range = 29-46) at age 3 and at kindergarten entry (77.2% retention rate). Reflecting the demographics of the Pacific Northwest city in the United States in which the study took place, 99 children (71.2%) were Caucasian, 28 children (20.1%) were identified as multi-racial, and 7 children (5.0%) were Hispanic or Latino, with all other race/ethnicity groups comprising <4% of the sample. Median household income was $30 000 (range = $2500-$175 000). The most common diagnoses at age 3 were speech/language (S/L) delay (54.7%), global developmental delay (15.1%), and ASD (15.1%); children were diagnosed by a primary care physician, psychologist, or licensed clinical specialist, or were deemed eligible for services by a multidisciplinary school/early intervention team. While all children possessed an IFSP (and were therefore eligible to receive EI/ECSE services), 29.7% of parents reported that their child had not received EI/ECSE services in the past 6 months (ie, between 2.5 and 3 years of age), likely reflecting variability in the timing of eligibility determination as well as the timing of developing an IFSP for the child prior to identifying and receiving services.
Measures
The project was reviewed and approved by the Institutional Review Board at the University of Oregon (Protocol Number 08242011.089). After parental consent was received, data collection of families and children occurred twice: once at age 3 and again at kindergarten entry (approximately 5 years of age).
Communication
Early communication at age 3 was measured using the receptive and expressive subscales of the Vineland Adaptive Behavior Scales–Second Edition (Vineland-II). 28 The Vineland-II was administered to the primary caregiver via phone interview. Raw scores—a simple count of correct responses—were converted to a V-scale score, which is on an equal-interval scale with a mean of 15 and SD of 3 and permits direct comparisons between children. Correlations between raw scores and V-scale scores were high for both receptive language: r = .90, and expressive language: r = .77, Ps <.001. The correlation between receptive and expressive language was moderate (r = .59, P < .001). Reflecting the presence of developmental delay and related conditions in the study sample, children had relatively lower scores on the Vineland Adaptive Behavior Composite (mean = 82.2 and SD = 12.4, compared with a normative mean of 100 and SD of 15).
Receipt of Special Education Services
A questionnaire on special education service utilization was administered during a home visit at kindergarten entry. Parents reported on whether the child had a primary and secondary diagnosis related to a developmental delay. Parents then indicated whether the child received services for the primary or secondary diagnosis in the past 6 months. The list of services included speech therapy, occupational therapy, sensory integration, physical therapy, behavioral programming, adaptive physical education, play therapy, music therapy, therapeutic listening, and other. We examined 3 sets of outcome variables. (1) Special education use was defined as the number of distinct services that the child received (ie, number of yes counts). Then, for each service marked as received, parents reported on the number of sessions per month. Special education dosage was defined as the number of sessions per month across all services received. (2) Special education use and dosage were also calculated after excluding speech therapy in order to examine whether early communication was related to utilization of special education services unrelated to speech and language. (3) Because of the investigation’s focus on early communication, speech therapy receipt and dosage were also examined separately as outcomes.
Covariates
Child- and family-level covariates included a dummy indicator for treatment status in the original study, child age at testing (at kindergarten entry), child gender, maternal education, and household income. Household income was reported using 2 methods: an open-ended format and selecting from 13 predefined income ranges. For the 16 children with mothers who did not respond to the open-ended question but selected an income range, the midpoint of the selected range was used to populate missing values. Because household income exhibited a log normal distribution, values were logarithmically transformed for use in the regression models. As research indicates a link between early communication deficits and a diagnosed S/L delay 8 or ASD, 7 dummy variables for S/L delay and ASD diagnoses at age 3 were also included as covariates. Finally, we controlled for teacher-reported academic competence at kindergarten entry (assessed using the Academic Competence subscale of the Social Skills Improvement System 29 ) in order to rule out the possibility that lower academic achievement, rather than early communication, might be predicting special education outcomes. Because teacher response rates were lower than parent response rates, we included a teacher report missing dummy variable and recoded missing values as the mean of valid non-missing values.
Analytical Method
We examined our research question using 3 separate but complementary analytical models: early communication predicting special education use (Model 1a) and dosage (Model 1b), early communication predicting special education use (Model 2a) and dosage (Model 2b) after excluding speech therapy, and early communication predicting speech therapy receipt (Model 3a) and dosage (Model 3b). Testing our models in this order allowed us to examine whether our results depend on the specificity (ie, broad to specific) of the operationalization of our special education service utilization variables. With the exception of the model predicting speech therapy receipt (which employed a logistic regression), ordinary least squares regression was used to test all models. Table 1 presents descriptive statistics for all included variables. Analyses were conducted in Stata 13.1.
Descriptive Statistics for Variables in Models a .
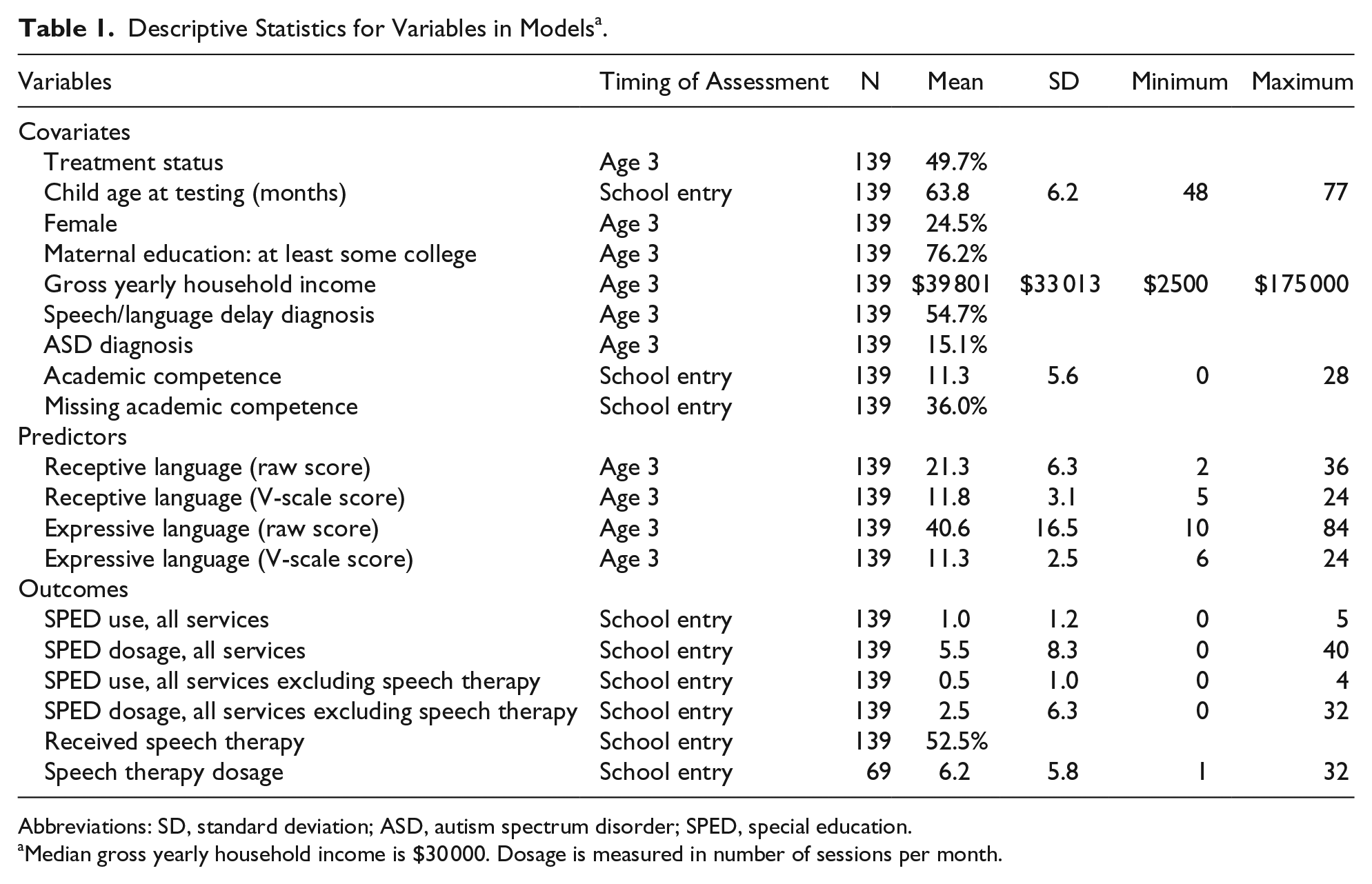
Abbreviations: SD, standard deviation; ASD, autism spectrum disorder; SPED, special education.
Median gross yearly household income is $30 000. Dosage is measured in number of sessions per month.
Results
Results are presented in Tables 2 to 4. Contrary to our first hypothesis, early communication was unrelated to special education use and dosage. As shown in Model 1a (Table 2), while a 1 SD increase in expressive language skills—but not receptive language—was associated with a 0.18 SD decrease in special education use (β = −08, P = .09), this finding did not reach conventional significance levels. As shown in Model 2a (Table 3), when predicting special education use excluding speech therapy, this marginal effect disappeared completely (β = −04, P = .35). As shown in Models 1b and 2b, we found no significant effects of communication (expressive or receptive) on dosage of special education services.
Point Estimates of Predictors of Special Education Service Utilization: All Services a .
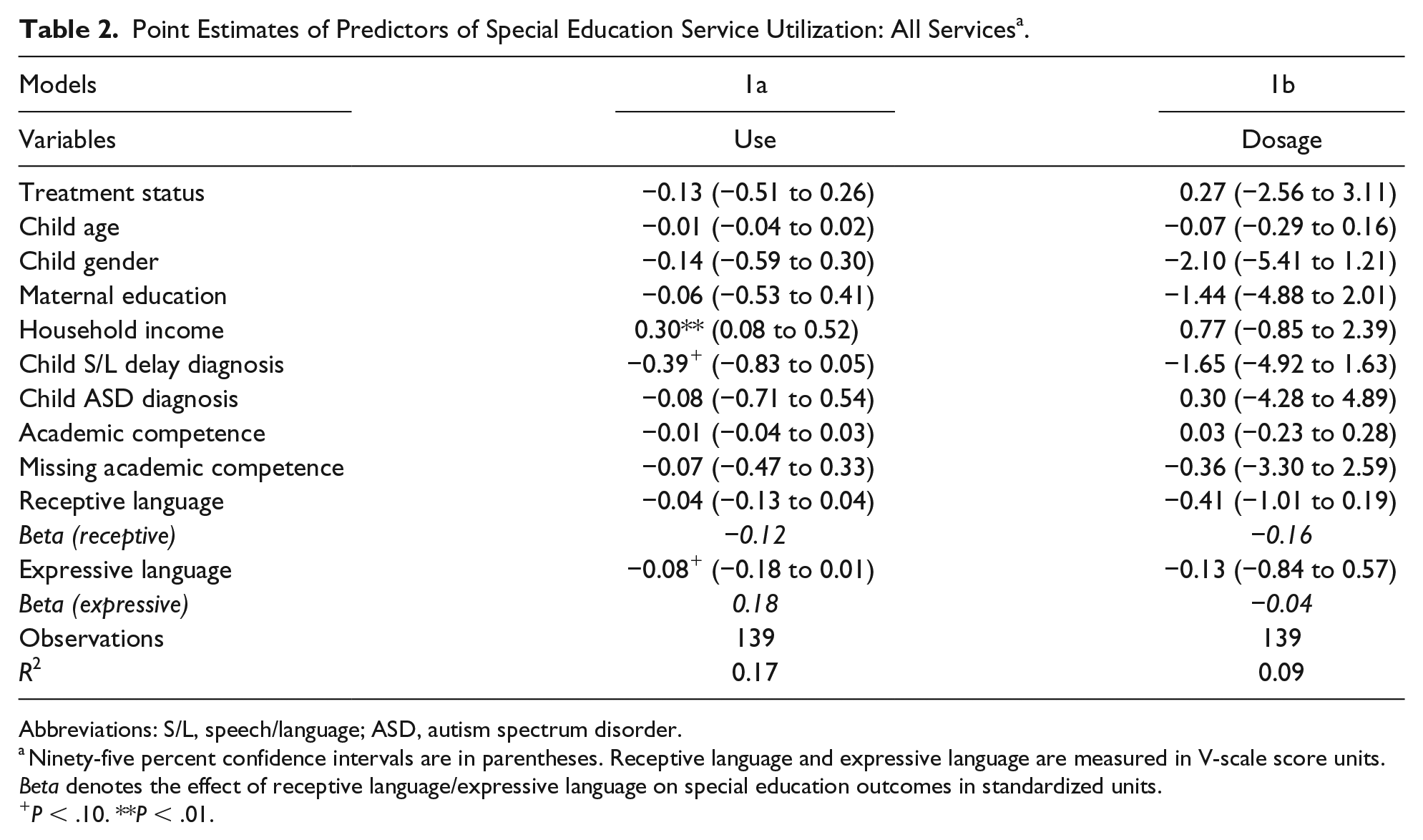
Abbreviations: S/L, speech/language; ASD, autism spectrum disorder.
Ninety-five percent confidence intervals are in parentheses. Receptive language and expressive language are measured in V-scale score units. Beta denotes the effect of receptive language/expressive language on special education outcomes in standardized units.
P < .10. **P < .01.
Point Estimates of Predictors of Special Education Service Utilization: All Services Excluding Speech Therapy a .

Abbreviations: S/L, speech/language; ASD, autism spectrum disorder.
Ninety-five percent confidence intervals are in parentheses. Receptive language and expressive language are measured in V-scale score units. Beta denotes the effect of receptive language/expressive language on special education outcomes in standardized units.
P < .05. **P < .01.
Point Estimates and Odds Ratios of Predictors of Special Education Service Utilization: Speech Therapy Only a .

Abbreviations: S/L, speech/language; ASD, autism spectrum disorder; N/A, not applicable.
Ninety-five percent confidence intervals are in parentheses. Receptive language and expressive language are measured in V-scale score units. Beta denotes the effect of receptive language/expressive language on special education outcomes in standardized units. Coefficients for Model 3a represent odds ratios from a logistic regression. Beta values for Model 3a denote the percent change in odds for a one standard deviation increase in receptive language/expressive language scores; this was calculated using the listcoef command in Stata.
P < .10. * P < .05.
Data supported our second hypothesis that early communication would be related to speech therapy receipt and dosage. As shown in Model 3a (Table 4), a 1 SD increase in expressive language scores at age 3 was associated with a 44.8% decreased likelihood of receiving speech therapy at kindergarten entry (odds ratio = 0.79, 95% confidence interval = 0.64-0.97, P = .02). However, receptive language was unrelated to speech therapy use. As shown in Model 3b, there were no significant effects of communication (expressive or receptive) on speech therapy dosage. Finally, a post hoc analysis was conducted that controlled for special education use at age 3. The pattern of results was virtually identical to those presented in Tables 2 through 4.
Discussion
In a community-based sample of children eligible for early intervention or early childhood special education services, stronger expressive language skills at age 3, but not receptive language skills, predicted a decreased likelihood of receiving speech therapy at kindergarten entry. This effect remained significant after controlling for treatment status, child- and family-level characteristics, and kindergarten academic competence. The present study yields important insights into the componential nature of early communication and language skills and replicates previous work demonstrating that deficits in expressive language are related to later language difficulties. 27 Expressive language fluency requires not just comprehension but also production of words; the greater cognitive and linguistic demands associated with expressive language might explain why deficits in speech production are linked with a greater likelihood of speech therapy receipt.
That said, it is important to acknowledge that some children might exhibit hyperlexia (strong expressive language and weak receptive language), which is likely to reflect an underlying neurodevelopmental condition such as ASD rather than natural variation in language abilities. Furthermore, some children might experience speech production difficulties (ie, apraxia or articulation disorders), which have little (if anything) to do with the cognitive demands associated with expressive language. As described earlier, while ASD and S/L delay were among the most common diagnoses in our community-based sample of children eligible for special education services, it is important not to overgeneralize our findings to all children, as the nature and degree of language difficulties can vary widely depending on the child’s underlying condition.
Our finding that early expressive language skills predicted speech therapy use in particular, but not a broader array of special education services, should be considered in light of our previous research demonstrating such a link between early communication and special education use in middle childhood. 19 We surmise that special education status at kindergarten entry might be attributable to a primary deficit in a specific functional domain, while special education status later in childhood might reflect a combination of developmental, behavioral, and learning difficulties that arise in part due to the greater breadth and complexity of schooling experiences as children get older. Early elementary educators are more likely to be proactive in initiating home contact regarding children’s experiences in special education compared with educators in later grades, indicating that meaningful differences exist in how educators, families, and students perceive and experience special education. 30 Future investigations can elucidate the nature of this link by examining longitudinal data across a longer time period.
Increasing attention has been devoted to understanding pediatricians’ knowledge and attitudes regarding special education. Findings from a study revealed significant knowledge gaps among pediatricians and pediatric residents regarding facts about special education and IEPs. Notably, the study found that while 85% of those surveyed agreed that pediatricians should assist families in obtaining special education services for children, <50% thought that they should assist in the development of a child’s IEP. 31 These findings underscore the importance of involving all professionals, not just pediatricians, in the coordination of a child’s individualized education plan and health care with their parents.
While the measure of early communication used in the present study has well-validated norms, it is not designed for screening purposes and does not have established clinical cutoff scores. The American Academy of Pediatrics has provided guidance for clinicians on developmental surveillance and screening, with regular evaluations recommended at 9-, 18-, and 30-month well child visits. 17 However, there remains a lack of a consensus regarding the optimal design and implementation of speech and language screening in preschool children in pediatric care settings. For example, measures of specific language impairment, a disorder characterized by below-average language ability but normal nonverbal skills, also suffer from a lack of precision and clarity regarding cutoff points used to determine specific language impairment status. 32 A risk modeling approach accounting for child and family factors assessed at 12 months of age has been shown to predict language difficulties at 4 years of age, 33 indicating that a holistic examination of multiple factors at various points in development might be a fruitful approach. Our findings indicate that the measurement of early communication—particularly when receptive and expressive language skills are assessed separately—has the potential to facilitate the identification of children who are at increased risk of requiring speech therapy and related services as early as kindergarten.
The lack of significant effects on dosage of special education services might be due to data limitations rather than reflecting a true null effect. In the present study, dosage was operationalized as the number of sessions per month, but data were unavailable on the length and purpose of each session. Based on anecdotal evidence from clinicians, we know that parents may struggle to accurately report the services that are being offered and delivered to their children, thereby potentially underestimating receipt and dosage of special education services. Examining detailed information regarding the duration and intensity of each service would yield further insights into the link between communication and special education outcomes.
Future studies should also consider whether and how differences between schools can expand our understanding of how early communication skills predict later special education use. To illustrate, in the present study, 71.5% of parents reported that their kindergarten child was enrolled in a school with special education eligibility. Of the 92 children for whom teacher-reported data were available, 65.2% of kindergarten children were enrolled in general education classrooms, 18.5% in self-contained special education classrooms, and 16.3% in inclusion/mainstream classrooms. While these data on classroom placement can provide a broader context of the child’s early schooling environment, the utility of this information can often be questionable. Schools vary in the amount and type of special education services that are offered. We know that some schools offer a full continuum of services, while other schools (such as in rural districts or under-resourced areas) do not. Moreover, schools might have different methods for reporting service use and dosage that make it difficult to compare special education data across schools. Other variables that might affect the interpretation of our findings include the degree of parental advocacy and the learning philosophy of a particular district superintendent or school principal, none of which are related to the actual support needs of the child. Therefore, while classroom placement might not be an accurate proxy for condition severity, future studies should seek to collect and examine more fine-grained classroom placement data in order to better contextualize findings.
Other limitations of our data should also be addressed. We did not have access to data on family history of communication difficulties, as well as information on perinatal factors such as prematurity status or birth weight, which have been shown to be related to later communication deficits. 34 An examination of these factors would yield a more complete understanding of how early communication is linked to special education outcomes. Finally, all of our measures relied on parent and teacher report; examining direct assessments of communication skills and administrative data regarding service utilization would help confirm and extend the results of the present investigation.
In conclusion, expressive language skills at age 3 predicted speech therapy receipt at kindergarten entry in a community-based sample of children eligible for early intervention or early childhood special education services. Screening of specific domains of early communication skills during routine pediatric care, in conjunction with the evaluations of other professionals involved in the child’s education and health, might be an effective method for identifying children who are more likely to receive speech therapy at kindergarten entry.
Footnotes
Acknowledgements
We thank Charlotte Winter for her support in preparing the data for analysis, Cheryl Mikkola for her support in the preparation of this manuscript, and the Oregon Parent Project staff for their assistance. We would also like to thank all the families and children who participated in this project.
Author Contributions
MHK: Contributed to analysis and interpretation; drafted the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. LLM: Contributed to conception and design; contributed to acquisition and interpretation; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in part by a grant from the National Institutes of Health (R01 HD059838) awarded to the second author.