
Abstract
Background. McCune-Albright syndrome (MAS) is characterized by hyperpigmented macules, endocrinopathies, and fibrous dysplasia. Hyperthyroidism is the second most common endocrinopathy in MAS and its management is challenging, particularly among infants and toddlers. Traditionally, young infants have been treated with antithyroid medications, but remission is likely and these medications have severe side effects and affect the control of other endocrinopathies. Thus, it is reasonable to consider permanent treatment options at an earlier age. In this article, we performed a retrospective chart review and describe 3 children who underwent thyroidectomy at an early age due to complex presentation. Case Descriptions. Case 1 was a female patient who underwent bilateral adrenalectomy due to adrenal hyperplasia and subsequently underwent thyroidectomy at 5 months of age due to unremitting hyperthyroidism with fibrous dysplasia, multiple fractures, and ovarian cysts with vaginal bleeding. Case 2 was a 20-month-old female on methimazole who acquired influenza A, precipitating a thyroid storm, and subsequently developed central precocious puberty. Case 3 was a 4-year-old female who underwent thyroidectomy because of unremitting hyperthyroidism after methimazole cessation due to declining neutrophils. All 3 children experienced no complications from thyroidectomy. Conclusions. Early thyroidectomy by an experienced surgeon is an option for managing MAS-associated hyperthyroidism, even in very young patients, with excellent results.
Introduction
McCune-Albright syndrome (MAS) arises from post-zygotic somatic mosaicism due to an activating GNAS mutation, and it is characterized by hyperpigmented macules, endocrinopathies, and fibrous dysplasia. As with all other manifestations of MAS, activation of the stimulatory G protein is responsible for thyroid gland hyperplasia, thyroid hormone overproduction, and increased conversion from T4 to T3.1,2 Clinically, this results in hyperthyroidism, goiter, and/or thyroid nodules. Hyperthyroidism is the second most common endocrinopathy in MAS, and its management is challenging, particularly in infants and toddlers.1,3
The rates of hyperthyroidism in MAS vary among studies, which are heterogeneous in terms of patient age and the method of assessing thyroid abnormalities. Hyperthyroidism diagnosis is simple; it involves measuring thyroid-stimulating hormone (TSH) and thyroid hormones. In hyperthyroidism, T4, T3, and free T4 will be elevated for age, whereas TSH will be suppressed due to negative feedback to the pituitary gland. Ultrasound assessment yields abnormal findings in 33% to 66% of MAS patients, including diffuse heterogeneity and hyperechoic and hypoechoic regions. However, only 10% to 30% of MAS patients have abnormal thyroid function, specifically suppressed TSH.2-5
There are 3 accepted strategies for hyperthyroidism management in children: antithyroid medication (eg, methimazole), radioactive iodine ablation, and thyroidectomy. 6 However, there are presently no specific guidelines for hyperthyroidism management in cases of MAS. Although most patients respond to antithyroid medication, hyperthyroidism is likely to recur on discontinuation of the medication; thus, more permanent options may be preferable, such as radioactive ablation or surgery. However, many experts use antithyroid medications until the patient is old enough to undergo a more permanent treatment modality.1,3
In the present retrospective chart review, we describe the cases of 3 children who underwent thyroidectomy at an early age due to complex presentation.
Case Series
We performed a retrospective chart review of 3 children with MAS who underwent thyroidectomy as toddlers at Texas Children’s Hospital. Hyperthyroidism was diagnosed based on thyroid hormone levels. This retrospective review of a limited case series was performed in accordance with the policies and procedures of the institutional review board of Texas Children’s Hospital. Informed written consent was obtained from the parents for cases 2 and 3. Written informed consent could not be obtained from the parents for case 1, despite all reasonable attempts, and every effort has been made to protect the patient’s identity.
Case 1
A female patient underwent bilateral adrenalectomy due to adrenal hyperplasia and subsequently underwent thyroidectomy at 5 months of age due to unremitting hyperthyroidism and difficulty gaining weight. She had no complications after total thyroidectomy including no damage to the recurrent laryngeal nerve or iatrogenic hypoparathyroidism. Prior to thyroidectomy, the patient had exhibited vaginal bleeding, bilateral ovarian cysts, and elevated estradiol without elevated gonadotropins. She was not a candidate for aromatase inhibitor treatment due to elevated liver function test results.
Two months after thyroidectomy, the ovarian cysts were decreased in size and the vaginal bleeding resolved. The patient also had neonatal cholestasis due to anatomic abnormalities; liver biopsy revealed a nearly completely absent portal tract, absence of hepatic early branches, and a single poorly formed bile duct. She exhibited improvements of transaminase and bilirubin levels after thyroidectomy. The patient’s overall clinical course improved for a period of time after thyroidectomy. However, she intermittently required intubation and suffered multiple catheter infections, and thus required tracheostomy at the age of 8 months. Her complex course also included fibrous dysplasia, multiple fractures, and left ventricle hypertrophy.
Case 2
A healthy 20-month-old female with café au lait macules and fibrous dysplasia presented with tachycardia and elevated thyroid lab results. Thyroid ultrasound revealed diffuse enlargement with heterogeneous echotexture, and increased color flow peripherally and within the isthmus, right lobe (4 mL; 3.3 × 2 × 1.3 cm), and left lobe (2.4 mL; 2.8 × 1.3 × 1.4 cm). The patient underwent a nuclear uptake scan, which revealed iodine uptake of 29% at 4 hours and 47% at 24 hours (normal thyroid iodine uptake reference values: 5% to 15% at 4 hours and 10% to 25% at 24 hours). The thyroid had a slightly asymmetric appearance, but without significantly asymmetrical uptake, hence not suggestive of a discrete hyperfunctioning nodule. The uptake scan was consistent with hyperthyroidism secondary to MAS, since the patient was negative for thyroid-stimulating immunoglobulins.
Due to elevated thyroid hormones, the patient was not treated with radioiodine ablation. After 5 weeks of methimazole treatment, she acquired influenza A, precipitating a thyroid storm. Maximum doses of methimazole and steroids yielded minimal improvement; therefore, the patient underwent total thyroidectomy at 24 months of age. While receiving medical management for hyperthyroidism, the patient presented vaginal bleeding and ovarian cysts that were treated with nonsteroidal aromatase inhibitor (letrozole). She eventually exhibited elevated gonadotropin levels, significantly advanced bone age, and crossed percentiles in length-for-age, thus treated for central precocious puberty with gonadotropin-releasing hormone (GnRH) agonist (Lupron) and letrozole. Eighteen months after her thyroidectomy, the patient exhibits appropriate suppression of puberty hormones, without signs of puberty. She has significant fibrous dysplasia and she sustained multiple fractures (Figures 1 and 2; Table 1).
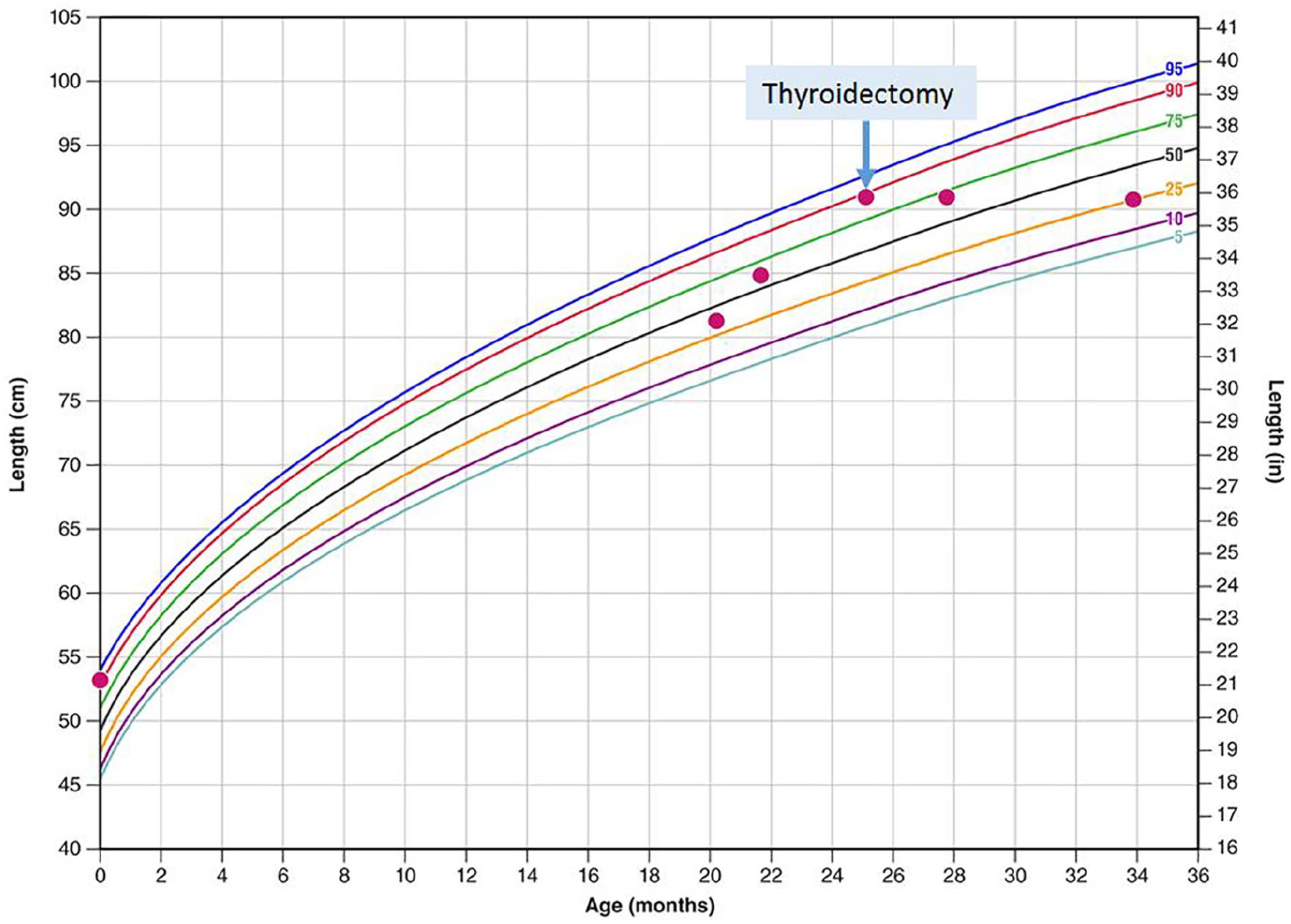
Growth chart of case 2, before and after thyroidectomy (arrow) at 24 months of age.

Hand film of case 2 at a chronological age of 21 months, showing a phalangeal bone age of 5 years and fibrous dysplasia (normal bone replaced by fibrous tissue that causes bones to expand; arrows).
Thyroid Laboratory Test Results, Puberty Hormones, and Growth Over Time for Case 2.

Abbreviations: TSH, thyroid-stimulating hormone; LH, luteinizing hormone; FSH, follicle-stimulating hormone.
Case 3
A 4-year-old female exhibited unremitting hyperthyroidism after methimazole cessation due to declining neutrophils, and subsequently underwent thyroidectomy with no complications. Initially, her thyroid ultrasound was significant for a diffusely abnormal thyroid with lobular contours and heterogeneous echotexture without the thyroid being impressively enlarged. She underwent a nuclear thyroid uptake scan, which showed normal uptake (17% at 4 hours and 22% at 24 hours). Thus, the patient was not a candidate for radioiodine ablation. She was also being treated with nonsteroidal aromatase inhibitor (letrozole) for peripheral precocious puberty that was started prior to her thyroidectomy. She had significantly advanced bone age and fractures with fibrous dysplasia (Figure 3).

Hand film of case 3 at a chronological age of 4 years and 8 months, showing a phalangeal bone age of 6 years and 10 months and fibrous dysplasia (arrows).
Discussion
The patients in these 3 cases exhibited clinical features remarkably similar to those of MAS at the time that the decision was made to perform thyroidectomy. Early recognition of hyperthyroidism in a patient with MAS is important since untreated hyperthyroidism can lead to complications including advanced bone age with premature growth plate fusion, which may exacerbate the decreased height associated with early sexual development, if present. 4 Additionally, long-term hyperthyroidism may cause osteoporosis and increased fracture risk, which is a particular concern in children with MAS and fibrous dysplasia. 3 All 3 of our patients suffered fractures as toddlers and exhibited precocious puberty and advanced bone age. Importantly, these patients are also at risk for rare life-threatening complications, such as thyroid storm and arrhythmias. 6
Although hyperthyroidism in MAS usually responds to thionamides, remission is unlikely. Thus, it is preferable for the patient to undergo definitive treatment. In the past, it has been recommended that thyroid surgery be delayed until an older age, since it may be difficult in very small children. 3 Our presently described observations suggest that thyroidectomy should be considered as an option earlier.
This analysis is retrospective, and we are unable to conclude that early thyroidectomy is the best approach for all institutions. We also cannot predict which children are at risk of unremitting hyperthyroidism. Nevertheless, our experience indicates that early thyroidectomy by an experienced surgeon is an alternative for managing MAS-associated hyperthyroidism, even at a very young age, with excellent results. Such treatment may have a substantial impact on the patient’s clinical course, especially their adult height.
As per the American Thyroid Association guidelines, the rate of complications may be reduced if thyroidectomy is performed by a high-volume thyroid surgeon—defined as a surgeon who performs 30 or more cervical endocrine procedures annually. 7 At our center, we implement standardization of surgical technique with 2 surgical faculty members involved in each case. In all 3 of our cases, thyroidectomy was performed by pediatric surgeons. Prior to proceeding with thyroidectomy, the best treatment option was discussed within our multidisciplinary program that includes experts in endocrinology, pediatric surgery, otolaryngology, pathology, radiology, and oncology. Before this can be considered an official practice guideline, additional studies are needed with larger pools of patients, at multiple centers with a full spectrum of pediatric care.
Footnotes
Author Contributions
Clinician/Surgeon for Case 1: Nadia Merchant, Johanna M. Viau-Colindres, David E. Wesson, Monica E. Lopez, Lefkothea Karaviti
Clinician/Surgeon for Case 2: Andrea E. Balazs, David E. Wesson, Monica E. Lopez, Lefkothea Karaviti
Clinician/Surgeon for Case 3: Kelly A. Hicks, David E. Wesson, Monica E. Lopez, Lefkothea Karaviti
All the authors contributed to editing the manuscript. Nadia Merchant and Lefkothea Karaviti provided the main ideas, outline, and wrote the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.