
Abstract
Using principal component analysis (PCA) and integrating both individual and household factors, we had previously derived and proposed 3 socioeconomic indices (namely, wealth index, educational index, and housing quality index) that can be used to classify rural Yemeni women into different socioeconomic statuses (SES). In the current article, we examined whether the PCA-derived indices can be used to predict the use of maternal and child health care services in rural Yemen. We used data from subnational representative multistage sampling cross-sectional household survey conducted in rural Yemen in 2008-2009 among women (N = 6907) who had given birth. The resulting component scores for each SES index were divided into tertiles. Logistic regression was used to study the associations between the SES indices and 4 indicators of maternal health care use. Higher tertiles of each socioeconomic index increased the likelihood of adequate antenatal care use, delivery assistance, and contraceptive use, but decreased the likelihood of unmet need for contraception. Key maternal health indicators can be determined by socioeconomic indicators. Therefore, in planning maternal and child health interventions, considering disparities of care by socioeconomic factors should be taken into account.
Keywords
Introduction
While encouraging progress has been made to achieve some set targets of the Sustainable Development Goal 3 (ie, reducing the global maternal mortality ratio, ending preventable deaths of newborns and children under 5 years of age, and ensuring universal access to sexual and reproductive health care services), 1 much remains to be done in some countries. Appeals for accelerated progress in scaling up professional prenatal and natal care as well as family planning services are being made.2,3 In Yemen, maternal and infant mortality and morbidity remain high. Annually 2880 women die, and for every maternal death, approximately 20 more women become disabled as a result of pregnancy and childbirth complications.4,5 Based on the 2013 Yemen National Health and Demographic Survey, almost 42% of women died at home. The neonatal death rate in Yemen was 26 per 1000 live births based on previous survey. 5 The maternal mortality rate is 148 per 100 000 live births, 5 and the infant mortality rate is around 43 per 1000 live births. 5 The situation is shaped by the high Yemen’s fertility rate as one of the highest in the world, with an average of 5 (4.4) births per rural woman. 5
Utilization of reproductive health care has the potential to decrease adverse pregnancy outcomes and improve maternal and newborn health and survival.6-8 Antenatal care (ANC) and natal visits are an opportunity to intervene. 6 The World Health Organization (WHO) recommends that pregnant women should have at least 4 ANC visits at specified intervals provided by skilled attendants. 9 These visits should contain essential interventions and commence as early as possible in the first trimester. 9 The ANC recommendation in Yemen tallies with that of WHO.9,10 Nevertheless, the 2013 Yemen National Health and Demographic Survey estimated that about 70% of births were home delivery; traditional birth attendant delivery 12%; deliveries assisted by an auxiliary nurse/midwife about 2%; and 41% of all women who gave birth in the 5 years preceding the survey were assisted by a relative or friend. Nationally, 60% of mothers who had a live birth in the 5 years preceding the survey reported at least 1 episode of ANC from a doctor, nurse, or trained midwife. This rate was higher in the urban areas at 80% and lower in the rural areas at 51%. 5 Furthermore, the survey reported that 29.2% of women were using modern contraception.
Optimal utilization of ANC may be hindered by various cultural, socioeconomic, and demographic factors, including mother’s age, parental education, household size, parity, lack of revenue, and accessibility, availability, quality, continuity of care.11-14 Furthermore, out-of-pocket expenditures that are associated with health care utilization are another significant barrier for women in accessing health care facilities, especially for low-income families. 12 The influence of socioeconomic status (SES) on the use of maternal and child health (MCH) care services has been studied in many previous studies; however, results appear to vary across and within contexts.15,16 In a previous article, 17 we developed SES indices for women in rural Yemen based on data from a subnational household survey, which we believe are useful for advancing research on the impact of SES on reproductive health in rural Yemeni settings. In the current article, to assess the usefulness of the developed SES indices in reproductive health research, we examine the associations between the constructed indices and 4 indicators of utilization of MCH services: ANC, skilled birth assistance, contraceptive use, and unmeet for contraception.
Methods
Study Design
We drew data from the subnational household cross-sectional survey conducted in Yemen in 2008-2009, which explored ways to improve MCH care in rural Yemen under the scheme of the Home-Based Maternal and Neonatal Care project carried out by UNICEF. In the current article, we have adapted analytical cross-sectional design in order to investigate the associations between our constructed SES indices and the 4 indicators of utilization of MCH services.
Participants and Study Setting
The survey recruited women who had given birth during the past 2 years prior to the survey from selected subnational governorates in Yemen: Dhale, Ibb, Taiz, and Hodeidah governorates by adapting the multistage sampling technique. From these 4 governorates, 6 rural districts were chosen based on their poverty levels as defined by Yemen national categorization. From these 6 rural districts, a list of 42 subdistricts was made and 26 representative subdistricts were chosen. Next, 213 villages were randomly selected from the 26 subdistricts and finally all households in these villages were eligible to be included in the survey. The target group was all reproductive-age females aged 15 to 49 years. The minimum sample size was fixed at 5000 births. This sample size allowed estimation of 50% prevalence with 2% precision and 99% confidence level. It was considered valuable to increase the sample size to more households so as to provide estimates with no much less precision in case of less prevalence. The sample included 7341 households and 7295 women meeting the inclusion criteria. The current analysis included 6907 women with a birth history and who took part in the interviews with a response rate exceeding 95%.
Data Collection
Prior to the main survey, face validity of a questionnaire was established by experts, and a pilot study was undertaken and observed changes were accordingly reflected in the main survey. Trained midwives who worked in the health services of the same areas conducted face-to-face interviews in Arabic. The respondents were contacted in their homes. Educated women respondents filled up the questionnaire, whereas in the case of illiterate women, their answers were filled up by the well-trained midwives in a standard way. The interview instrument was a 64-item structured questionnaire that gathered information on participants’ socioeconomic and demographic characteristics, women’s reproductive history, MCH care utilization during the last pregnancy, childbirth and maternal mortality, as well as neonatal and infant mortality.
Ethical Approval and Informed Consent
Ethics approval for the survey was obtained from Committee for Research at the Ministry of Health, Yemen. In addition, ethics approval was obtained from UNICEF-Yemen review committee. Before starting the interview, women were given the choice to give their informed consent to participate. The study was conducted in accordance with the Declaration of Helsinki ethical principles.
Socioeconomic Measures
In a previous article, 17 we used the various responses from the questionnaire related to individual and household characteristics to construct SES indices for the women participating in the subnational household survey through principal component analysis. That study was motivated by lack of existing SES index for rural Yemeni women; thus, the developed SES indices were aimed at enabling subsequent classification of reproductive-age women into appropriate SES levels and to help in assessing the influence of SES on MCH in these rural Yemeni settings. We derived 3 SES indices (namely, wealth index, educational index, and housing quality index), which all together explained 54% variations in the SES of the women. Then, based on the factor scores of each index, they were categorized into tertiles and these were used for subsequent analyses.
Outcome Measures
We evaluated the ability of the developed SES indices to predict 4 indicators of MCH services utilization, namely, ANC adequacy, skilled birth assistance, contraceptive use, and unmet need for contraception. We developed an ANC adequacy index according to the approach proposed by the WHO, which takes into account the timing, number, and content of ANC (Appendix 1, available online).9,10 In order to measure the utilization of ANC adequacy with reference to the most recent pregnancy, women were asked about their experiences of attending ANC visits, number of visits, timing in relation to pregnancy months, and what kind of care package they received. Regarding the content of ANC, 10 items outlined in the new WHO ANC model were asked in the survey. 18 These items made up a typical minimum ANC content in Yemen and included the following: (1) one item on pregnancy surveillance (pregnancy examination of the woman and her unborn child); (2) one item on preventive measures, including immunization and screening (for anemia, malaria, and sexual transmitted diseases); (3) one item on recognition and management of pregnancy-related complications and coexisting disease; (4) one item on health education and promotion for the women and her family healthy behavior; (5) five items on biomedical assessments (body weight measure, blood pressure measure, urine test, blood test, ultrasound examination); and (6) one item on care provision (iron tablet and folic acid supplement). Adequacy of content of ANC was defined as the total number of items provided to a woman, and we classified this as follows: “Fair” (7 or more items, or more than 70%), “Poor” (0 to 6 items or less than 70%), and “No care.” ANC adequacy variables in the study were categorized into 3 levels of the adequacy of care as follows: women who received care in the first trimester and had 4 or more visits and had received fair ANC content were classified as fair ANC care adequacy; those who received any other care not matching with the WHO fair adequacy level were classified as poor ANC care adequacy; and those with no care were classified as no care.
Based on answers of women describing present use of contraception, an indicator of contraceptive use was dichotomized into: none and using any contraceptive to delay or to avoid getting pregnant. Unmet need was identified in the survey based on the question asking women about their experiences of a present manners and desires relating to contraceptive use, fecundity, and fertility preferences (Appendix 1).
Furthermore, to measure the indicator of skilled birth assistance with reference to the most recent delivery, women were asked whether they had given birth at home without trained assistance, had delivered at home with trained assistance, or delivered in a health care facility.
Data Analysis
Data were examined by descriptive statistics (frequencies and percentages). We applied logistic regression to analyze the associations between each of the SES indices and the 4 MCH care utilization indicators. The associations between the SES indices and utilization of adequate ANC, contraceptive use, and unmet need were analyzed using binary logistic regression. For the analysis purpose, ANC adequacy indicator was coded 1 if the utilization of care was classified as fair adequate according to the WHO index and 0 otherwise. While the contraceptive usage was coded 0 for none, and 1 for use of any contraceptive, unmet need for contraception was coded 0 for met need and 1 for unmet need for contraception.
Nevertheless, the association with health care–seeking behavior during delivery was analyzed using multinomial logistic regression as that variable had 3 categories. For the multinomial logistic regression for health care–seeking behavior, we estimated the odds of choosing either a facility delivery or a home delivery with the medical assistance of a trained practitioner versus a traditional home delivery without trained medical assistance. In the analysis, women who delivered at home without trained assistance were coded 1, women who delivered at home with trained medical assistance were coded 2, and women who delivered in a health care facility were coded 3.
For each of our 4 dependent variables, we constructed 2 models: model 1 contained no covariates and examined the association between each of the SES indices and each of the dependent variables; model 2 included each of the SES indices and all household and individual covariates, namely, women’s age at birth, stillbirth, spontaneous abortion, chewing qat, tobacco usage, under-age marriage, and family marriage. For fitting regression model 2, we used enter criteria method to create fully adjusted models to analyze the appropriate regression of each health services utilization outcome. The estimated odds ratios were accompanied by their respective 95% confidence interval (CI). Statistical significance was fixed at <.05. SPSS version 19 was used for statistical analyses.
Results
Characteristics of the Study Population
Socioeconomic characteristics of the surveyed households were reported in our previous article. 17 Data were available for 6907 women who had birth history and had taken part in the interviews living in 7341 households. The average age of the sampled women was 31.9 (9.7 standard deviation) years. Approximately 6247 (90%) of the women were 18 years and older. Majority of the heads of households 3930 (57%) had no education, while 2977 (43%) had at least a primary school education.
In terms of economic status, there was polarity in the economic status of the women households. Those on the lowest level of SES formed 1788 (26%) and those on the highest level of SES 2220 (32%).
Furthermore, 660 (10 %) of the women had under-age pregnancy (ie, pregnancy under 18 years of age); 1867 (27.1%) family marriage (ie, a marriage with man who is related as second cousin or closer); 1506 (22%) had used tobacco; 2841 (41.2%) had chewed qat; 2120 (31%) had family planning; and 3863 (56%) had ANC (Table 1).
Maternal and Child Health Services Indicators According to Women’s Background Characteristics Among Women From Rural Yemen, 2008-2009.
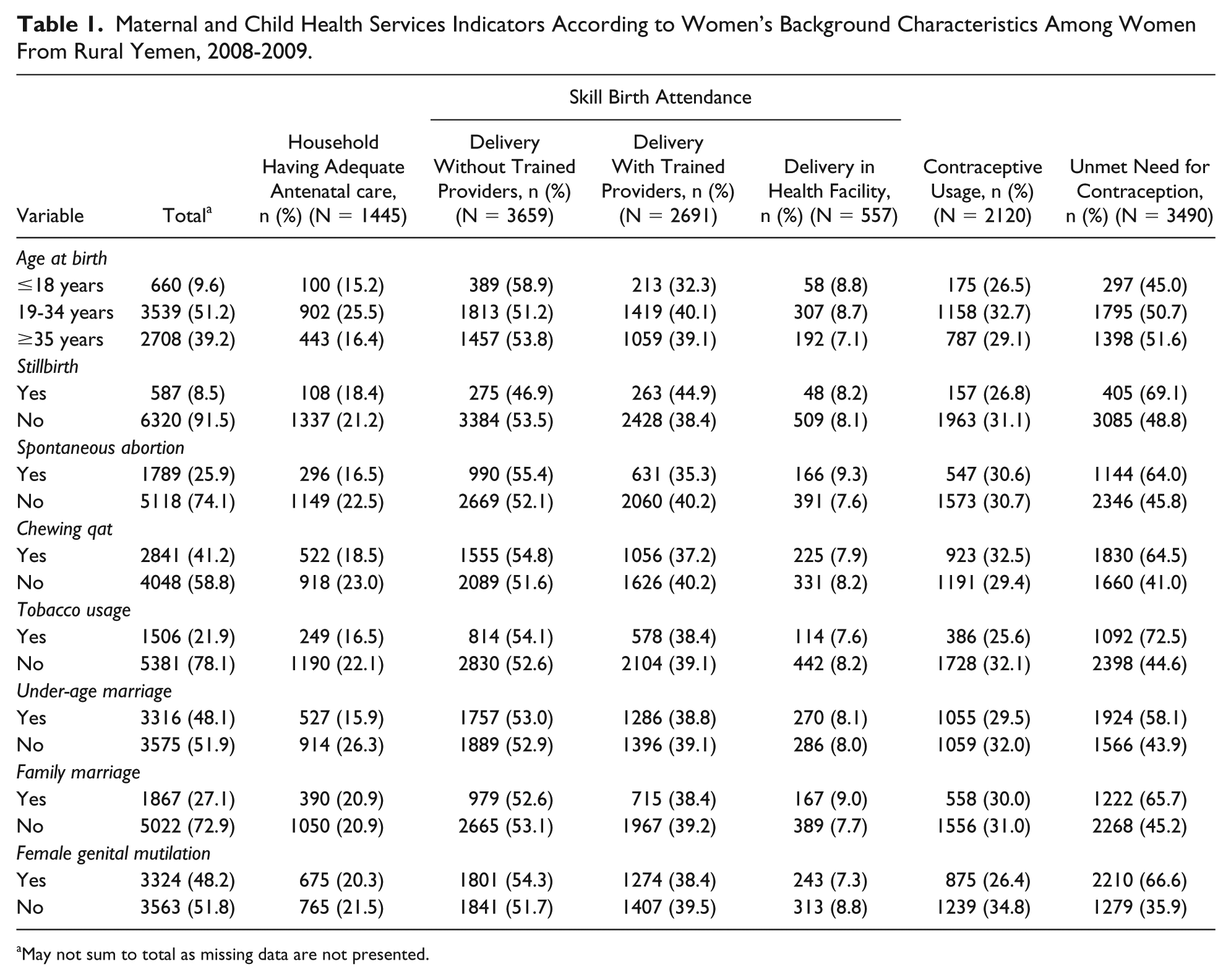
May not sum to total as missing data are not presented.
Antenatal Care Use
The use of ANC services was low, with 3044 (44%) women not having any ANC. Usage of adequate ANC according to the WHO index was 1445 (21%). The results of the association between the SES indices and ANC are presented in Table 2, which showed that higher tertiles of wealth and educational indices but not housing quality index were associated with utilization of fair adequate ANC (adjusted odds ratio [AOR] = 3.34, 95% CI = 2.76-4.04, and AOR = 3.68, 95% CI= 3.15-4.31, respectively).
Associations Between SES Indices and Adequate Antenatal Care Utilization, Contraceptive Usage, and Unmet Need for Contraception Among Rural Yemeni Women of Reproductive Age (ORs and 95% CIs).

Abbreviations: SES, socioeconomic status; OR, odds ratio; CI, confidence interval; WHO, World Health Organization.
All variables were simultaneously adjusted.
Reference category.
Birth Delivery Assistance
Only 557 (8%) of women had facility delivery as a birth delivery assistance option, while home delivery with skilled birth attendant was 2691 (39%), making the rest of delivery at home without any skilled birth attendant. Women of households with higher tertiles in any of the SES indices (wealth, educational, and housing quality) were significantly more likely to choose a facility delivery and a home delivery with the assistance of a trained practitioner versus a traditional home delivery without trained assistance (Table 3).
Associations Between SES and Birth Delivery Choice Among Rural Yemeni Women of Reproductive Age (ORs and 95% CIs).

Abbreviations: SES, socioeconomic status; OR, odds ratio; CI, confidence interval.
Reference category.
Use and Unmet Need for Contraception
Overall, 4787 (69%) of women had used any contraceptive method, while 3490 (50.5%) have unmet need for contraception. Higher tertiles in any of the SES indices were associated with more likelihood of using any contraceptive methods (Table 2). On the other hand, higher tertiles in each of the SES indices were associated with less likelihood of having unmet need for contraception (Table 2).
Discussion
Findings and Interpretation
In this study, using previously developed SES indices (namely, wealth, educational, and housing quality indices) for women from rural Yemen 17 to predict indicators of maternal and child care utilization, we found that higher tertiles of wealth and educational indices, but not housing quality SES index, were associated with more likelihood of having fair adequate ANC. Higher tertiles in each SES index were associated with more likelihood of using birth contraception as well as having a facility and home delivery with the assistance of a trained practitioner versus a traditional home delivery without trained assistance. On the other hand, higher tertiles in each SES index were associated with less likelihood of having unmet need for contraception.
Our findings indicating that higher levels of the SES indices were associated with the usage of fair adequate ANC agree with previous reports.19-22 These pervious results demonstrate that women who are economically disadvantaged or those who have low educational level may experience less optimal utilization of adequate ANC compared with women with better economic or educational status.19,20,23-26 Some studies have shown that high SES and educational attainment empowers women to seek modern health services. Such women can often afford to pay for health services and any associated travelling costs. 20
However, other studies show no evidence of such an association. 27 It has been assumed in earlier studies that SES measurement may be indicator specific; therefore, different SES measures have different correlation with each of indicators.28,29 These views are in line with the study conducted by Magadi et al, who showed no evidence of such an association perhaps due to the variety of variables involved in the analysis and the multivariate character of the statistical analysis. 30
Women at higher levels of each of the SES indices were significantly more likely to choose a facility delivery or a home delivery with the assistance of a trained practitioner compared with women at lower SES indices. Several previous studies have reported similar findings,20,25,30 an indication that higher SES both economically and educationally empower women to seek institutional and better maternal delivery health services. Such empowerment provides women an opportunity to attain a higher level of health awareness, better ability to pay for health services and other related costs, and more autonomy and ability to make choices on maternal services to use.20,27
Women of higher SES were significantly more likely to use contraception compared with women in lower indices. With regard to unmet need for contraception, poor and less educated women were more likely to have unmet need for contraception than more wealthy and educated women. These findings similarly compare with results from other previous studies.31,32 The clear SES predictive effects of contraceptive use are in line with findings of study conducted by Becker et al, who has postulated that lower status of wealth and education undermined women’s autonomy, leading to women’s inability to follow through on an individual choice of contraceptive use and lesser utilization of modern reproductive health care. 11
Strengths and Weaknesses of the Study
The sample size of the study was large and thus was sufficient to uncover any real estimate of association between the SES and the study outcomes. Furthermore, the high participant response rate made our observations reasonably generalizable across different rural settings in Yemen. This is the first study from rural Yemen that has assessed the utility of comprehensive SES indices (combining both individual- and household-level wealth indicators) in predicting indicators of utilization of MCH care services. Therefore, this study provides an important platform for the advancement of research on the role of SES in utilization of reproductive health care in rural Yemen. The study does have some limitations: data on indicators of MCH services utilization were collected from women with reference to their latest childbirth during the 2 years preceding the survey. Maternal recall of events within 2 years prior to the survey is subjected to recall bias, particularly for items of ANC content. Given the cross-sectional design whereby data on SES and the outcomes were collected at the same time, we cannot infer causal associations between the SES indices and indicators of MCH services utilization.
Relevance of the Findings: Implications for Clinicians and Policy Makers
The findings of this study provide a basis for a number of policy implications and recommendations for decision makers that aimed at meeting many of the health care needs of the socioeconomically disadvantaged women, children, and families in rural Yemen. One is that SES was found to have an important influence on the use of MCH services, and this indicates the need for policy decision makers to improve female educational opportunities by applying national policies that are able to address literacy gender equity in rural Yemen. Such policies would encourage female education and sooner or later enhance gender wealth equalities, women’s autonomy, and MCH services use. Second, socioeconomically disadvantaged women were found to be less likely to use MCH services suggests that adapting interventions to focus on subgroups of population where there are high needs and ensuring equity in MCH services would ultimately reduce inequalities in MCH services utilization.
Conclusion
In this study, we have shown that our previously developed SES indices for rural Yemeni women, incorporating individual and household wealth indicators, can be used to predict women utilization of a range of indicators of MCH care services. This effort highlights the importance of multicomponent SES indices for reproductive research in rural Yemen. Consideration of SES in the development of appropriate public health interventions and relevant policies aimed at mitigating the negative influences on MCH in rural Yemen is paramount.
Supplemental Material
Supplementary_Material – Supplemental material for Using Household Socioeconomic Indicators to Predict the Utilization of Maternal and Child Health Services Among Reproductive-Aged Women in Rural Yemen
Supplemental material, Supplementary_Material for Using Household Socioeconomic Indicators to Predict the Utilization of Maternal and Child Health Services Among Reproductive-Aged Women in Rural Yemen by Abdullah Nagi Alosaimi, Bright Nwaru, Riitta Luoto, Abdul Wahed Al Serouri and Halima Mouniri in Global Pediatric Health
Footnotes
Author Contributions
This article was designed, analyzed and written by Alosaimi Abdullah under the supervision of Bright Nwaru and Riitta Luoto. Alserouri Abdelwahed, and Halima Mouniri did the surveys in the provinces. All authors commented and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.