
Abstract
Early care and education (ECE) providers and parents can facilitate physical activity (PA) and reduce screen time in preschoolers. Input from caregivers on barriers and facilitators of PA and screen time is needed to comprehensively address these behaviors and promote children’s health. Four focus groups (3 parent and 1 ECE provider) were conducted. Thematic analysis was performed to identify themes and subthemes. Twenty-eight caregivers (21 parents and 7 ECE providers) participated. Caregivers reported responsibility for modeling and shaping children’s PA and screen time. Parents felt that a busy lifestyle was a PA barrier and encouraged screen time. ECE providers were concerned about certain environmental influences on PA. The groups differed in their view of screen time as either entertainment (parents) or educational (providers). Both types of caregivers were unaware of PA or screen time guidelines. Investigation into opportunities to utilize screen time to serve priorities of both caregivers and promote child PA are needed.
Introduction
Adequate physical activity is important for 2- to 5-year-old children’s physical growth, 1 cognitive development, 2 and later school competence. 3 Physical activity can also influence development of motor skills at this age, 4 which can translate into later physical fitness in adulthood. 5 Despite the importance of physical activity, only about half of children ages 3 to 5 years meet the current physical activity recommendation for preschool-age children. 6 The current recommendation for this age group is 3 hours/day of any intensity activity (light, moderate, or vigorous), which has been endorsed by 4 independent panels from separate countries (Australia, 7 Canada, 8 the United Kingdom, 9 and the United States 10 ). Another important guideline for young children is screen time or activities done in front of a screen (eg, watching TV, using a computer, or playing video games), which is 1 hour or less per day.7,8 However, a recent cross-sectional study of 3- to 4-year-old Canadian children reports that only 24.4% of young children met this guideline. 11 Early screen time in toddlerhood was negatively associated with social skills in kindergarten age in a longitudinal study of 251 children. 12 Therefore, this excess amount of screen time may hinder physical activity engagement and its benefits.
Parents are a large influence on young children’s physical activity and screen time, and previous cross-sectional evidence has indicated that parents’ behaviors can both positively and negatively influence physical activity and screen time.13,14 Despite parents’ large influence and opportunity to model physical activity behaviors for their children, previous qualitative studies have found mothers of 2 to 5 year olds felt that there were many barriers to physical activity. 15 Specifically, mothers felt that they had limited time to engage in physical activity with their children due to household demands and have safety concerns at home for physical activity, hence limiting physical activity opportunities. 15 It may be hypothesized that this opportunity for physical activity may be replaced with screen time, as another qualitative investigation of mothers of children ages 2 to 4 years found that mothers relied on screen time to entertain their children so that they could accomplish household chores. 16 There is limited evidence in this age range of parents utilizing screen time for child physical activity. As it may be difficult to promote physical activity at home with existing demands, other daily settings for children should be considered. Accordingly, cross-sectional evidence has found that parents are more comfortable with their child playing outside and being physically active at their childcare center, or early care and education (ECE) center, rather than at home. 17 Thus, working with parents and ECE providers together may provide an opportunity to enable physical activity and lower screen time in young children.
Of note, about 80% of children in the United States between the ages of 3 and 5 years attend a formal care-based setting, namely, an ECE center. 18 In a national sample, full-time enrollment in ECE centers was associated with higher physical activity, less screen time, and desirable growth in young children compared with those only enrolled part-time. 19 These positive behavioral outcomes may occur because the majority of ECE centers follow a scheduled day and are required by the state to follow guidelines, including limited screen time and providing a certain amount of teacher-led, unstructured, and outdoor opportunities for physical activity. 20 A previous qualitative study found ECE providers felt that physical activity, particularly outdoors, is important for preschoolers. 21 Furthermore, these ECE providers recognized the many benefits from allowing preschoolers to engage in physical activity, 21 which is promising for promoting child physical activity. However, there are varying reports of children obtaining adequate physical activity in ECE centers,22,23 as ECE providers’ views and actual enactment of center policies may vary. 21
There are few data reports on the role of the ECE centers’ physical activity environment or policies and subsequent influences on children’s behavior, and even less is documented regarding screen-viewing policies and practices. A previous natural experiment compared changes in ECE centers following statewide physical activity policies versus a comparator state without statewide polices; those ECE centers in the state with the policy changes demonstrated improvements in the ECE environment, including increased training in physical activity and additional equipment and play environment, but no changes in staff behaviors. 24 As such, ECE providers’ views and implementation of physical activity and screen time policies are important to evaluate.
Furthermore, there is limited literature regarding ECE providers’ views on screen time, even though ECE screen time may be an important contributor to children’s total screen time. 25 As most prior studies focused on perspectives of only one caregiver (either parents or ECE providers) or on one behavior (physical activity or screen time), there is narrow investigation of opportunities to concurrently facilitate physical activity and decrease screen time within the child’s entire day.
Considering the differing views and priorities of parents and ECE providers, additional investigation into both types of caregivers’ views on barriers and facilitators to these behaviors is needed in order to fully assess the influences on young children’s physical activity and screen time. Identifying these barriers and facilitators could lead to the development of more effective interventions to increase children’s physical activity. The purpose of this study was to solicit and compare parent and ECE provider input about barriers and facilitators to children’s physical activity and screen time, awareness of relevant regulations and recommendations, and caregiver-identified opportunities to leverage screen time to increase young children’s physical activity.
Methods
Pause and Play
In 2015, Louisiana’s Department of Education implemented new ECE center regulations regarding physical activity and screen time. Specifically, ECE centers must create both a written physical activity policy and procedure (stating that the center provides at least 1 hour of physical activity per day including both teacher-led and free play) and an electronic device policy (stating that the center allows no more than 2 hours a day of screen time). 26 Prior to these policies, there was no statewide physical activity and screen time requirements for ECE centers to obtain or renew licensure. The “Pause and Play” study, a multilevel community-academic engagement project, was created in response to these new state regulations and to facilitate enactment of these guidelines. 26 This mixed-methods study included longitudinal data collection of children in 10 ECE centers alongside qualitative focus groups to determine parents’ and ECE providers’ perspectives on children’s physical activity and screen time. In the longitudinal study, the demographics, accelerometry data, and screen time habits of children were collected both at home and at ECE centers before and after the implementation of the new guidelines. The results of the quantitative portion are presented elsewhere.22,27 This article presents qualitative data from the focus groups conducted as the part of the qualitative portion of this mixed-methods study.
While investigating baseline data from before the enforcement of new state licensing regulations, it was found that most children met the physical activity guideline and the screen time guideline during a classroom observation 27 and that most ECE centers allowed limited amounts of screen time. 27 The use of educational screen time was associated with more total physical activity among children. However, the children’s average amount of screen time at home was significantly higher than the guideline. 27 These findings together suggest that both parents and ECE providers are contributing to physical activity and screen time at this age. The qualitative focus groups were conducted to provide context to barriers and facilitators to children’s physical activity and screen time from the perspectives of parents and ECE providers.
Participants
The study aimed to recruit 16 to 30 participants in total, including 3 to 4 focus groups each comprising 8 to 10 people. At the start of the study (2015), there were 187 ECE centers available to recruit in the selected parish (county) of a southeastern US state, according to information provided by the Department of Education. Parents and ECE directors and staff (ECE providers) from this parish (county) were recruited via email, mail, fax, phone, and in-person. Inclusion criteria for participation included being either a director or staff member of a licensed ECE center within the specific parish or being a legal guardian and/or primary caretaker of a child aged 3 to 5 years who was enrolled in a licensed ECE center (hereafter referred to as parent), able to understand and speak English, and willing to be audio-taped during the focus group (for transcription purposes). Exclusion criteria included persons who were non-English speakers, who reported a cognitive impairment that interfered with participation in a group discussion, or who was an ECE provider or a parent of a student of the 10 ECE centers that were assessed for the longitudinal data collection portion of the study 22 ; the purpose of excluding these was to obtain views on physical activity and screen time independent from those exposed to the longitudinal study. Non-English speakers were not included as the project did not have the resources or staff available to facilitate the focus groups in a different language or to translate materials to a different language. All participants who expressed interest were able to be included as none met the exclusion criteria.
Procedures
Focus groups were held between January and March 2017, including 3 focus groups with parents and 1 with ECE providers. Additional information about the focus group procedures is provided in Supplementary File 1 (available online). Shortly following consent, participants completed a demographic questionnaire. Two trained staff members, with one serving as the moderator, facilitated the focus groups. The trained staff members served as a neutral party and had not met the parents or ECE providers prior to the focus groups. The same trained research staff members facilitated and moderated each focus group. All focus groups were audio recorded and transcribed. The moderator script was developed by AES using previous research 26 and based on the overall research question and aims of the Pause and Play study. The moderator led the focus group discussion with a series of scripted, open-ended questions to facilitate focused discussion related to parents’ and ECE providers’ general health concerns and, specific to physical activity and screen time, their views on barriers and facilitators of these behaviors and knowledge of current policies (see Table 1). Each focus group lasted approximately 60 minutes. Participants received $20 as compensation for their time.
Moderator Script for Focus Group Discussions a .

Abbreviation: ECE, early care and education.
Questions are presented in the order they were asked within the focus group.
Measures
Parents completed a demographic survey to describe basic information about themselves and their child including age, sex, height, weight, race/ethnicity, marital status, household size, education, employment status, and annual household income. Parents’ body mass index (BMI) was calculated using the self-reported information and the standard formula (kg/m2), and child BMI percentile was calculated for age and sex. 28
ECE providers reported their age, sex, height, weight, race/ethnicity, role in their ECE center, and characteristics of their center (including number of children enrolled and policies related to physical activity and screen time) on a demographic survey. ECE providers’ BMI was also calculated using the standard formula (kg/m2) using their self-reported height and weight. ECE providers were asked on this same questionnaire to how much free play and screen time was allowed for the children. Categorical responses were provided for active play time (45 minutes a day or less, 46-60 minutes a day, 60-90 minutes a day, 90-120 minutes a day, and more than 120 minutes a day); structured (or teacher-led) activities (1 time per week or less, 2-4 times per week, 1 time per day, and 2 or more times per day); and screen time allowed at ECE center (more than 2 hours per day of total screen time, 1-2 hours per day of total screen time, 30 minutes to 1 hour per day for total screen time, less than 30 minutes per day for total screen time, and no screen time). These response categories were based on previous measures evaluating ECE center policy.29,30
Data Analysis
The primary endpoints of the focus group discussions were qualitative themes from the parent and ECE provider perspective on barriers and facilitators to children’s physical activity and screen time, and awareness of current policy. Two independent researchers, CB and JSR, analyzed the transcripts for content analysis. Content analysis included the following: (1) generation of key words and phrases repeated independently in another focus group; (2) grouping of variables based on coalescing concepts and themes; and (3) review of the theme groupings to ensure consistency and relevance of the proposed unifying concepts. After themes were created by CB and JSR, a third researcher (AES) reviewed themes to confirm that content was appropriately analyzed and themes found focused on the aim of the study (barriers and facilitators to child behavior). The procedure used was similar to the analysis of other parent focus groups, which focused on identifying barriers and facilitators to behavior. 31 Saturation was reached when themes repeated across multiple focus groups. Saturation was assessed a priori for the directors, but the parent focus groups continued until saturation was reached. All data analysis occurred using NVivo software (Version 10, QSR, Victoria, Australia).
Ethical Approval and Informed Consent
Pennington Biomedical Research Center’s Institutional Review Board approved this study (Study Number #6218). Informed consent was obtained verbally before participation. The consent was audio recorded.
Results
Twenty-eight participants across 4 focus groups enrolled and participated, with group sizes ranging from 3 to 13 participants (Focus Group 1 = 3 parents at a library, Focus Group 2 = 5 parents at a library, Focus Group 3 = 13 parents at an ECE center, Focus Group 4 = 7 ECE providers at a library). Most participants completed the demographic questionnaire (89% of parents and 100% of ECE providers). Three parents did not complete the demographic questionnaire with differing reasons including another parent was also a participant, refusing the survey, and not returning the survey. Of the total sample, most were female (94% of parents, 100% of directors), and the sample was diverse in terms of age, race, and socioeconomic status (Tables 2 and 3). The range of parent ages was 24 to 59 years. Much of the sample (67%) were African American. About half had less than a high school diploma or GED (56%) and did not know their child’s height or weight (56%). Most reported a height and weight that would classify them as overweight (28%) or obese (56%).
Descriptive Characteristics of Parents (n = 18) a .
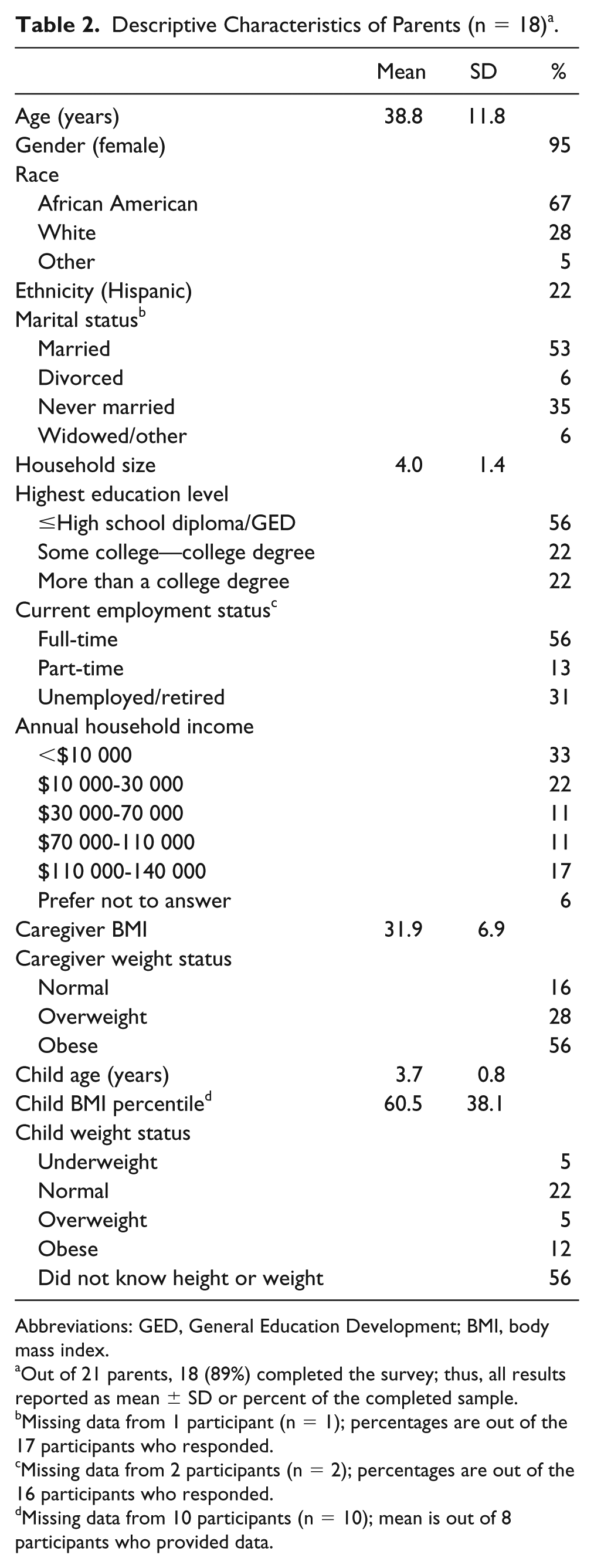
Abbreviations: GED, General Education Development; BMI, body mass index.
Out of 21 parents, 18 (89%) completed the survey; thus, all results reported as mean ± SD or percent of the completed sample.
Missing data from 1 participant (n = 1); percentages are out of the 17 participants who responded.
Missing data from 2 participants (n = 2); percentages are out of the 16 participants who responded.
Missing data from 10 participants (n = 10); mean is out of 8 participants who provided data.
Descriptive Characteristics of ECE Providers (n = 7).

Abbreviations: ECE, early care and education; BMI, body mass index.
The age range of ECE providers was 24 to 56 years, and 57% were white. Many ECE providers were employed by a privately owned or operated ECE center (71%). ECE providers served as either the owner/director (43%), teacher (29%), assistant director (14%), or the director of the ECE center (14%). Over half reported that their centers provided more than 2 hours/day of active play to children (71%), that their centers provided structured (or teacher-led) activities that occurred 2 or more times per day (57%), and that screen time was not allowed in their center (57%). In total, most ECE providers reported that their center provided more than the required 60 minutes of daily active play time (86%), and all ECE providers reported that they met the recent screen time guideline (providing fewer than 2 hours per day of screen time, 100%).
Thematic Findings
Four major themes, with up to 3 subthemes, were identified following the thematic coding of the focus group transcripts: (1) influences on physical activity and screen time; (2) physical activity barriers and facilitators; (3) screen time barriers and concerns; and (4) policies, rules, and regulations related to physical activity and screen time. These themes and corresponding quotes are presented in Table 4.
Focus Group Themes and Supporting Quotes From 4 Groups of ECE Providers and Parents of Children Ages 2 to 5 Years Regarding Their Views on Barriers and Facilitators to Children’s Physical Activity and Screen Time.

Abbreviation: ECE, early care and education.
Influences on Physical Activity and Screen Time
Parents and ECE Providers’ Shared Influence on Physical Activity and Screen Time
Overall, participants felt that both parents and ECE centers shared the responsibility of providing positive examples of physical activity and appropriate screen time behaviors for children to model. Several parents acknowledged that their time can be limited with their children. Some parents and ECE providers felt that ECE providers could be a larger influence on their children. ECE providers reiterated this sentiment, expressing perceived responsibility to provide physical activity opportunities for children in consideration of the parents’ busy schedule and limited time.
Parent Modeling of Physical Activity and Screen Time
There was specific attention paid to the parental influence on modeling physical activity and screen time. Both parents and ECE providers mentioned that parents can potentially be negative influences on preschoolers’ physical activity and screen time by making screen time readily available. Parents specifically acknowledged the influence their own modeling of behaviors can have on children’s activity.
Both parents and ECE providers recognized that they have a complementary role influencing child physical activity and screen time. Participants understood that parents were the main facilitators of behavior, but the high amount of time children spend at ECE also influences behavior development making ECEs in a unique position to help children.
Physical Activity Barriers and Facilitators
Barriers to Physical Activity
Barriers to preschoolers’ physical activity both at home and at ECE environments were discussed. Specific to the home environment, parents acknowledged that they themselves could be barriers to physical activity and mentioned that when they get home from work, they are often too tired to engage in physical activity with their preschoolers and instead turn to screen time.
Both parents and ECE providers identified safety and the weather as other barriers to physical activity. Parents felt that an insufficient number of accessible sidewalks and parks, and a lack of safety measures in existing parks, created a barrier for children’s outdoor physical activity. ECE providers noted that even when following all safety guidelines in the ECE center, accidents can easily happen when children are playing outside; therefore, limiting play time outdoors is seen as a safety precaution by some centers. Weather was also mentioned as a barrier to children’s physical activity. Most participants said that weather conditions, such as extreme temperatures and rain, prevent children from playing outside and restrict the children’s indoor play.
Facilitators of Physical Activity
Even though a few parents mentioned that their preschoolers were naturally physically active on their own, both parents and ECE providers acknowledged that they have the potential to positively influence children’s physical activity. Parents and ECE providers both felt that engaging in physical activity with the children and providing more opportunities for them to be physically active were the best ways to encourage preschoolers’ natural desire to be active.
Screen Time Barriers and Concerns
Child’s Current Screen Time and Barriers to Reducing Screen Time
At home, parents reported using screen time as a way to distract their child so that they are able to complete necessary tasks around the house or elsewhere, or so that they can rest. Therefore, parents felt that the main barrier to reducing their child’s screen time was the parent’s own need for screen time in order to relax or use as a distraction while the parent was performing other tasks.
In general, ECE providers felt that the main barrier to reducing preschoolers’ screen time is that screen time has become a fundamental part of both the educational system and society as a whole. For example, some ECE providers said that testing for elementary school placement is on a computer so children who are not familiar with the technology are at a disadvantage. Accordingly, ECE providers felt that preschoolers must be exposed to some screen time.
Screen Time–Related Concerns
Unlike ECE providers, some parents believed that screen time did not have any educational value. The majority of parents expressed concern over the screen time content and did not want to expose their preschoolers to inappropriate topics for their age group. In addition to what may be seen during screen time, parents and ECE providers were concerned with unwanted associations their children may develop with screen time.
The main barriers to reducing screen time differed by type of participant, with parents feeling screen time is necessary to complement their busy lifestyle and ECE providers expressing that screen time is essential for the child’s education progress. Despite different barriers, both parents and ECE providers were concerned about children’s potential actions associated with screen time including undesirable language and food associations.
Policies, Rules, and Regulations Related to Physical Activity and Screen Time
Home
Overall, parents did not have any policies for physical activity at home. Some parents did mention having routines that incorporated physical activity but not set rules. Regarding screen time, most parents said that they did not have set rules at home regarding their preschoolers’ screen time but do set family routines that leave little room for screen time. Some parents may monitor or limit when they feel their children engage in too much screen time and adjust to the situation.
ECE Center
The majority of parents knew that their ECE centers had physical activity regulations, yet only some parents were aware of the specific regulations. Despite most not knowing their ECE center’s physical activity regulations, parents noticed the physical activity opportunities their children was receiving at the ECE center.
As for ECE providers and physical activity regulations, there were mixed reports on whether or not the center had specific physical activity recommendations or regulations for engaging children in physical activity. However, most ECE providers were aware of opportunities built into the ECE daily schedule or culture that provided opportunities for physical activity, such as going outdoors.
As for screen time, the majority of parents were aware of their ECE centers’ screen time policies. Most of the parents said that their center had a zero tolerance policy for screen time, meaning they did not allow any form of screen time at all, while some of the parents said that their ECE center used a minimal amount of screen time and only for educational use. Many parents were pleased with these policies. The majority of ECE providers reported that their centers had policies of no screen time, but some said their ECE centers did allow minimal screen time or used it for educational use.
National and State
In general, parents were not aware of national recommendations or regulations for preschoolers’ physical activity. ECE providers believed that there were national recommendations for physical activity from the American Academy of Pediatrics but were unaware of the exact recommendations.
Most of the parents were aware that national screen time recommendations for preschoolers did exist but were unsure on the exact recommendations. In general, parents were aware that it is recommended to limit the amount of screen time for their preschoolers. ECE directors were aware that screen time regulations did exist but felt that they did not need to keep up with them because their ECE centers offered either minimal screen time or no screen time at all.
Discussion
The focus group findings highlight several key differences between the ECE providers and parents’ views on young children’s physical activity and screen time, notably regarding engagement and regulation. The focus group sample was diverse and included participants from different races and socioeconomic backgrounds, with many of the participants identifying themselves as coming from a low-income household. Both parents and ECE providers identified each other and themselves as being responsible for and having influence over children’s physical activity and screen time. However, ECE providers mainly viewed screen time as an educational requirement, while parents saw screen time as entertainment. Regarding rules and regulations, parents did not have any formal rules in the home for physical activity or screen time, but most parents and ECE providers were aware of ECE center regulations. ECE providers were unaware of the exact national guidelines for physical activity and screen time but believed that they complied with them. Neither parents nor ECE providers mentioned the recent change in the Louisiana Department of Education ECE center regulations regarding physical activity and screen time. 26 Also, neither type of caregiver described opportunities to substitute screen time for physical activity. These findings highlight the importance of disseminating guideline and policy information on these behaviors to both types of caregivers (parents and ECE providers) as a strategy to promote healthy child development.
Parents and ECE providers acknowledged that they share a responsibility to encourage physical activity and exemplify being active themselves for the children. A recent systematic review of qualitative studies involving parent, ECE providers, and 2- to 6-year-old children’s views on barrier and facilitators to young children’s physical activity and sedentary behavior found that collaboration between parents and ECE providers could become an area of tension and hinder working together. 32 However, in the present focus groups, there was an understanding of the need for harmony between the 2 groups. For some parents, this focus on harmony came from acknowledging the high amount of time their child spends at the ECE center, similar to parental sentiments on the influence of ECE centers in another qualitative investigation. 33 In the present focus groups, ECE providers acknowledged the shared responsibility and empathized with the parent’s constraints at home. Other qualitative research involving parent and ECE providers has found that ECE providers from ECE centers were empathetic to the parents’ busy lifestyle, 34 which may be due to the close connection of the ECE providers with parents within their community. Communication was not mentioned as frequently in the present sample but is another important part of creating a harmonious parent—ECE provider relationship as found in a recent systematic review of qualitative studies involving physical activity. 32 As the focus of this study was on child-level outcomes, these themes may not have emerged unlike in another qualitative study that specifically focused on collaboration between parents and ECE providers. 34 Therefore, understanding this shared responsibility is a promising step forward for parents and ECE providers to working together for child health.
Barriers and facilitators to physical activity in children were identified both at home and at the ECE center. Parents and ECE providers both identified weather and safety as potential barriers to children’s physical activity, which have been previously identified as barriers to physical activity in a cross-sectional study of 388 parents and 151 ECE providers. 17 A cross-sectional study of 408 slightly older children (ages 5 to 18 years) also in Louisiana found that precipitation was associated with lower rates of meeting physical activity guidelines, 35 though parents and ECE providers in this focus group study were also concerned about heat. Accordingly, ECE weather policies have been found to be barriers of physical activity in Midwestern ECE centers, 21 as some ECE providers preferred to stay indoors to avoid being uncomfortable outdoors (eg, hot, cold, getting dirty).
Despite concerns over weather, parents and ECE providers both noted that their involvement in the child’s activities and taking the child to physical activity–specific locations, like the park, could help facilitate more physical activity. A previous cross-sectional study found that parents were more comfortable with children playing outside at the ECE center compared with outside at home, 17 but these focus groups did not reiterate this sentiment. ECE providers did feel that outdoor physical activity was beneficial and that this location facilitated more activity, similar to another qualitative study in ECE providers. 21 Children may benefit from visits to nature/forests with parents, as a cross-sectional study of 821 preschoolers found that visits to nature/forests were associated with lower sedentary time. 36 The same study found that parents of lower educational backgrounds used yards or areas more frequently than parents of higher educational backgrounds, and this frequency was associated with lower sedentary time, 36 which is an important convenient option as half of the current sample had a lower educational level. Outdoor physical activity may also ameliorate concerns about indoor physical activity, which have limited physical activity opportunities from safety concerns as reported in another qualitative study of mothers of preschoolers. 15
As for ECE provider involvement, a quasi-experimental study of ECE centers found that after training providers to increase children’s physical activity, teacher-led physical activity increased and children engaged in less sedentary behavior and more light physical activity. 37 This finding demonstrates ECE providers’ potential influence to facilitate more active classrooms. Together, parents and ECE providers identified unmodifiable (weather and heat) and modifiable (place and involvement) barriers and facilitators to physical activity. Additional investigation is needed into ways that modifiable behaviors, such as educating ECE providers on methods for engaging children in physical activity, could be used to increase children’s physical activity.
Parents and ECE providers have different views on the use of screen time in children’s daily life and long-term mental and physical development. Parents felt the main barrier to reducing screen time in the short term was that screens are already incorporated into the families’ daily life, which is a similar sentiment to other qualitative studies investigating the parental view on screen time. 38 In a systematic review of qualitative studies in older children (11-18 years old), most studies reported that parents were conflicted but mainly cited cognitive and psychosocial concerns from excess screen time, 39 which is different than the concerns expressed in the present study of inappropriate language and eating while watching the screen. These cognitive and psychosocial concerns may not be as apparent in children ages 3 to 5 years but may emerge in later childhood, or parents of preschool-aged children have different parenting priorities compared with parents of older children.
In contrast to parents’ concerns, ECE providers viewed the use of screen time as early preparation for later school outcomes and felt that children must be exposed to screens and technology to be successful later on in school and society as a whole. Conversely, parents did not report utilizing screen time as an educational tool. In the baseline analysis of the Pause and Play study, the use of educational screen time at ECEs was associated with higher total physical activity among children 22 ; hence, these ECE providers’ views on screen time may be a result of their own experiences using screen time to facilitate healthier behaviors. Overall, there is a discrepancy in the caregivers’ views of the use of screen time. Further studies on the educational use of screen time at home and at the ECE center may be warranted to understand how screen time can serve priorities of both caregivers.
Overall, both parents and ECE providers were unaware of specific policies and regulations but had their own rules and informal, unwritten policies related to physical activity and screen time. Other qualitative investigations have found parents of preschoolers believe that their child is sufficiently active so they do not set specific rules related to physical activity, 40 hence the lack of formal rules regarding physical activity. As for the regulations or policies at the ECE center level, parents believed that their ECE centers had policies for both physical activity and screen time but were unsure of the exact policies, which is similar to a cross-sectional study of 98 parents who reported their ECE center had an outdoor activity policy but could not provide specifics. 41 ECE providers had mixed reports on their centers’ physical activity regulations, but most ECE providers were aware of their centers’ specific screen time policies, with the majority of the centers having policies that allowed zero screen time (57%). Notably, none of the parents or ECE providers mentioned the recent change to Louisiana regulations regarding physical activity and screen time, though most reported that they believed their center was following the guidelines. It is unclear when these policies began to be implemented in these respective ECE centers and the extent to which these ECE providers were aware of the change in regulation. As other studies have seen improvements in ECE center environments following the enactment of statewide ECE physical activity and screen time policies, 24 assessment of the ECE center environment may show other changes from the policy enactment.
In this sample, the ECE providers were relatively more knowledgeable about physical activity benefits and policies compared with screen time policies, potentially due to their prior training and education. In a cross-sectional study of 107 ECE centers, it was found that over half of ECE centers in the United States provide training to increase child physical activity, 42 but there is currently no requirement for ECE providers to receive education related to screen time recommendations or specific national guidelines. ECE providers may only be provided with professional education related to physical activity and not receive additional information related to these other guidelines. In a previous study, ECE provider physical activity training facilitated more child physical activity, 37 hence additional training on appropriate use of screen time and guidelines may support less screen time or convert entertainment screen time to educational screen time. Given the rapidly evolving screen time environment of young children and the high amounts of screen time in many children’s daily life, ECE providers and parents alike may need supplementary training on screen time guidelines.
Strengths of the study included the diversity of focus group participants. Both the parent and ECE provider groups represented a variety of socioeconomic groups and ethnicities, including 67% African American for parents and 43% for ECE providers, and 55% of parents had an annual income below $30 000 per year. This diverse sample helped illustrate barriers and facilitators across different groups, but the groups were not large enough to compare responses by different race or income groups. Another strength was the inclusion of both parents and ECE providers, and physical activity with screen time, since caregiver and behavior are significant influences on the young child’s daily life. Evaluating these behaviors simultaneously may help provide additional understanding into the substitution and change in these behaviors both inside and outside of the home. Limitations include the lack of information on the child’s physical activity and screen time, and experience and training related to physical activity and screen time provided at the ECE centers. This information would provide more insight into the current activity of the child and the background of the ECE providers. This study was conducted alongside an observational study, which did evaluate screen time at home, inside the ECE centers, and objectively measured physical activity that can be used for comparison. 22 The main limitation of the study is that the research participants represent a small sample of ECE providers and parents and reflect the regulations for one state. Thus, the findings of the present study may not be generalizable to a national sample but do provide a useful example in a state that recently strengthened its regulations.
Future studies should focus on understanding the ways screen time can serve priorities of both types of caregivers, namely, as an education tool or potentially to facilitate physical activity itself. Parents and ECE providers did not acknowledge that replacing screen time with another sedentary behavior, such as reading or coloring activities, might still limit child physical activity. Further investigations should evaluate opportunities for caregivers to utilize screen time as physical activity, such as exergames or watching educational dance videos. Parent and ECE providers’ personal preferences regarding physical activity and screen time were not collected in this study, though this information could introduce new avenues for increasing children’s physical activity. As both parents and ECE providers were unaware of most regulations and national recommendations, better dissemination strategies are needed to inform both caregivers on adequate amounts of these behaviors. Moreover, expanding this exploration of ECE providers and parents in other states, municipalities, and countries would provide a comprehensive view of how these caregivers can work together for child health. Overall, future investigation is needed to identify specific ways parents and ECE providers can work together throughout the day to create healthier environments for children.
Conclusion
In total, there were several differences between parent and ECE provider perspectives on physical activity and screen time, notably in the use and perceived educational value of screen time. Parents and ECE providers acknowledged their dual influence on young children’s physical activity and screen time throughout the day, which is promising for their working relationship and opportunities to collaborate. Parents and ECE providers were unaware of policies or guidelines on children’s physical activity and screen time, highlighting the need for educational outreach on these topics for both types of caregivers to facilitate adequate physical activity and reduce screen time among young children. Further exploration is needed into altering modifiable behaviors to increase young children’s physical activity and improve their health.
Supplemental Material
supplement_material – Supplemental material for Young Children’s Screen Time and Physical Activity: Perspectives of Parents and Early Care and Education Center Providers
Supplemental material, supplement_material for Young Children’s Screen Time and Physical Activity: Perspectives of Parents and Early Care and Education Center Providers by Elizabeth D. Joseph, Chelsea L. Kracht, Jessica St. Romain, Andrew T. Allen, Caroline Barbaree, Corby K. Martin and Amanda E. Staiano in Global Pediatric Health
Footnotes
Author Contributions
EDJ and CLK contributed to data interpretation and drafted the manuscript. JSR and CB contributed to data acquisition, analysis, and interpretation. ATA contributed to data acquisition. CKM contributed to study conception, design, and data analysis. AES contributed to study conception, design, data analysis, and drafting of manuscript. All authors provided critical review of the manuscript and gave final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The “Pause & Play” project was supported by Award Number U54MD008602 for the Gulf States Collaborative Center for Health Policy Research (Gulf States-HPC) from the National Institute on Minority Health and Health Disparities of the National Institutes of Health. AES was supported in part by 1 U54 GM104940 from the National Institute of General Medical Sciences of the National Institutes of Health, which funds the Louisiana Clinical and Translational Science Center. CKM is supported in part by the NORC Center Grant P30DK072476 entitled “Nutrition and Metabolic Health Through the Lifespan” sponsored by NIDDK. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.